
Abstract
Objectives:
Head and neck squamous cell carcinoma (HNSCC) management is complex due to its unique anatomical location and multimodal treatment strategies. Multidisciplinary teams (MDT) including surgeons, radiation and medical oncologists, speech pathologists, nutritionists, physical and occupational therapy specialists, and nursing personnel are critical for optimal care. Despite the benefits of MDTs, effective collaboration among teams can be challenging, leading to fragmented or skewed care. We developed an online curriculum with the goal of increasing knowledge, competence, and confidence of MDTs caring for HNSCC patients.
Methods:
An online continuing medical education (CME) curriculum was available to all healthcare professional. Physician participants were categorized as surgeons, oncologists, radiologists, or pathologists. Participants completed pre- and posteducation questions. The effectiveness of the curriculum was evaluated based on question performance, self-reported confidence levels, and a qualitative questionnaire assessing program impact and participant satisfaction.
Results:
All modules were available through an online platform (www.medscape.com) for 8 years (2015-2022). A total of 24 631 physicians participated. All physician specialties demonstrated improved knowledge, competence, and confidence levels, with the highest gains observed in understanding treatment mechanisms and the ability to create customized care plans. Physicians intended to modify their treatment plans (83%), committed to making these changes in actual practice (92%), and expect improved impact in their practice (86%).
Conclusions:
The online HNSCC-focused curriculum significantly improved knowledge and confidence levels among MDT members. These findings underscore the value of CME to support well-coordinated MDTs and optimize HNSCC management.
Introduction
Head and neck squamous cell carcinoma (HNSCC) is one of the most common malignancies globally, with ~946 500 new diagnoses globally in 2022. 1 The unique anatomical location of HNSCC affects a plethora of vital functions including mastication, swallowing, speech, and facial expression among others. 2 Disease management, especially for advanced disease, involves multimodal treatment with different combinations of surgical resection, definitive or adjuvant radiotherapy, and primary, neoadjuvant, or adjuvant systemic therapy (chemotherapy, targeted therapy, and/or immune checkpoint inhibition). 3 However, significant treatment-related morbidities and toxicities exist along with varied outcomes due to complex anatomy and tumor biology.4 -7
The survival and function/quality of life has improved significantly for HNSCC patients due to new therapeutic advances, particularly with the incorporation of immunotherapy in the curative and palliative setting.8 -12 However, new therapeutic strategies have increased the complexity of management. Therefore, HNSCC management involves multiple disciplines, including pathologists, radiologists, head and neck surgeons, medical oncologists, radiation oncologists, speech and language pathologists, nutritionist, physical and occupational therapists, and nursing.13,14
It is well documented that multidisciplinary care improves patient outcomes and achieves lower morbidity and better survival rates.13,14 A well-coordinated multidisciplinary team (MDT) approach has emerged as the gold standard for HNSCC care, with the implementation of MDT care resulting to increased overall and disease-specific survival. However, the establishment of MDTs and maintaining efficient communication and collaboration between its members can often be challenging. 15 Patients often encounter fragmented and uncoordinated care, leading to compromised treatment, distress, and dissatisfaction.16 -18 Paired with the various disease- and treatment-related stressors, the lack of proper care coordination can negatively impact patients’ quality of life and treatment compliance. 17
To improve MDTs’ care for patients with HNSCC, we created a curriculum of continued medical education (CME) activities offered through an online platform. The primary objective of the study was to assess the educational impact of the curriculum.
Materials and Methods
An online curriculum of 12 online, CME-certified modules was developed by Medscape Oncology and the Society for Immunotherapy in Cancer. Modules focused on 6 core competencies: mechanism of action, treatment guidelines, clinical trial data, mitigating adverse events, identifying biomarkers, and creating a customized care plan. All modules were available to any healthcare practitioner (HCPs) through an online platform (www.medscape.com) for 8 years (2015-2022). Participants were classified by profession and specialty. Access to Medscape’s content via membership was required to participate. Anonymous data collection was performed and thus the study did not necessitate IRB review. Consent for data collection was part of the Medscape membership agreement. Participants, including physicians and other HCPs, listed their area of specialty, which was categorized as either oncology, surgery, radiology, pathology, or other. The analytical sample focused on physician participants who identified as oncologists, surgeons, radiologists, and pathologists. Participants’ qualifications were verified using the AMA and/or NPI databases, when possible.
Within each module, participants were asked the same set of questions prior to exposure to content (pre-assessment) and following exposure (postassessment). To qualify for analysis, participants had to complete both the pre-assessment and postassessment, which consisted of the same set of questions. A repeated-pairs design evaluated the impact of the activity, so that each participant served as their own control.
According to their performance, each participant was characterized in 1 of 3 categories: (1) improved—participant answered at least 1 more question correctly after the educational session relative to pre-education, (2) reinforced—participant answered the same number of questions correctly after the educational session relative to pre-education, (3) needs education—participant answered no questions correctly or fewer questions correctly after the educational session relative to pre-education.
Participant’s level of confidence was evaluated on a scale of 1 to 5. Confidence was considered increased, if the confidence rating increased between pre-education (rating 1-4) and posteducation by at least 1 point. Confidence was considered maintained if the confidence rating was equal between pre- and posteducation evaluations. Confidence was considered decreased, if the confidence rating was decreased between pre- and posteducation by at least 1 point.
A qualitative questionnaire was also administered after completing at least one of the modules, to evaluate program impact and participant satisfaction. Participants were asked: (i) if they plan to make 1 or more practice changes (eg, modify treatment plan, change screening/prevention practice), (ii) if they are committed to make those changes, (iii) if they agree that the content learned from this activity will impact their practice, (iv) if they agree that the activity supported achievement of each of the learning objectives (LOs), (v) if they agree that the program was presented effectively and was free of commercial bias, (vi) if they would recommend the activity to others.
Summary statistics were used to describe the analytical sample. Paired-samples t-test was conducted to assess overall number correct and confidence change statistical significance. A McNemar’s test is conducted to assess question-level and LO-level statistical significance. The statistical level of significance was set to 0.05. Cohen’s d is used to estimate the magnitude of the educational impact (modest: <0.20, small: 0.20-0.49, moderate: 0.50-0.79, large: ≥0.80). Statistical analysis was performed using the Rserve analytics extension in Tableau (R version 3.6.2; The R Project for Statistical Computing [R Foundation for Statistical Computing]). Visualizations were also created in Tableau.
Results
Modules were viewed 48 921 times in total, including 25 831 physicians (10 976 surgeons, 5687 medical oncologists, 90 radiologists, 1391 pathologists, and 7687 other physicians) and 21 506 other HCPs. Test takers were 19 186 in total, with the number of participants per module varying from 424 to 9432.
Oncologists
Across all 6 core competencies, oncologists improved their knowledge ranging from +9% to +56% relative change (P < .05; ranging from P < .005 to P = .018). The largest improvement was seen in the creation of a customized care plan (Figure 1). Further, 97% of oncologist either experienced an improvement or reinforcement of their confidence. In terms of integration of immunotherapy into a treatment plan, oncologists had a +58% relative change in their confidence (P < .005). Finally, over the course of the 7 year program, the percentage of oncologists reporting either improved or re-enforced subjective competence in managing patients with HNSCC in the MDT setting after reviewing the curriculum increased by ~10% between 2015 (79%) and 2022 (87%).
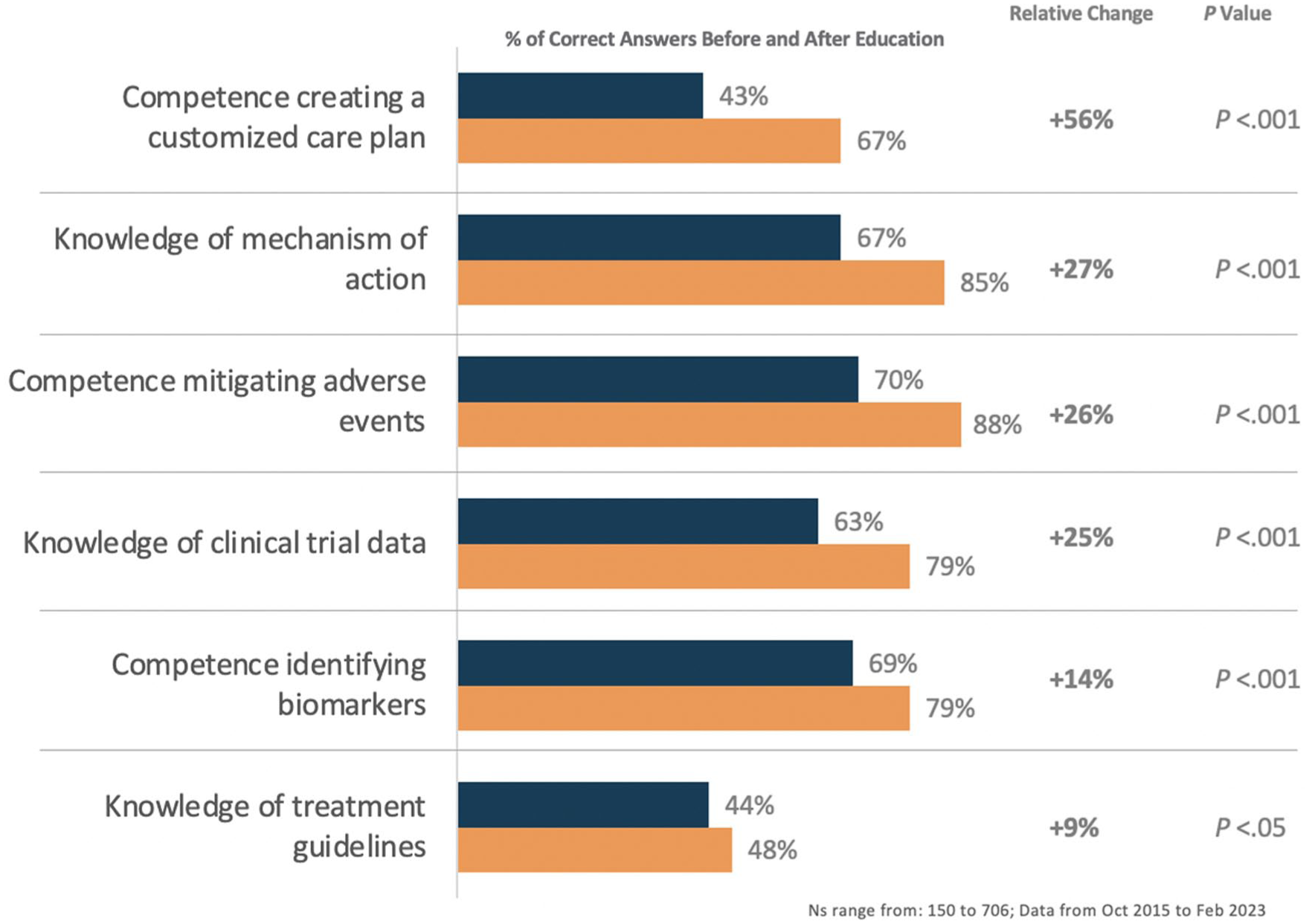
Oncologists’ improvement in knowledge/competence throughout activities.
Surgeons
Across all 6 core competencies, surgeons had an improvement in the percentage of correct answers before and after education, ranging from +25% to +66% (Figure 2). Knowledge of treatment guidelines (24%-34%) was the only theme where the increase was not significant (P = .066). The greatest improvement was observed in creating a customized care plan and understanding of the mechanism of action. Additionally, surgeons had a +86% relative change in their confidence integrating immunotherapy in the treatment paradigm (7% pre-education, 13% posteducation; P < .005).
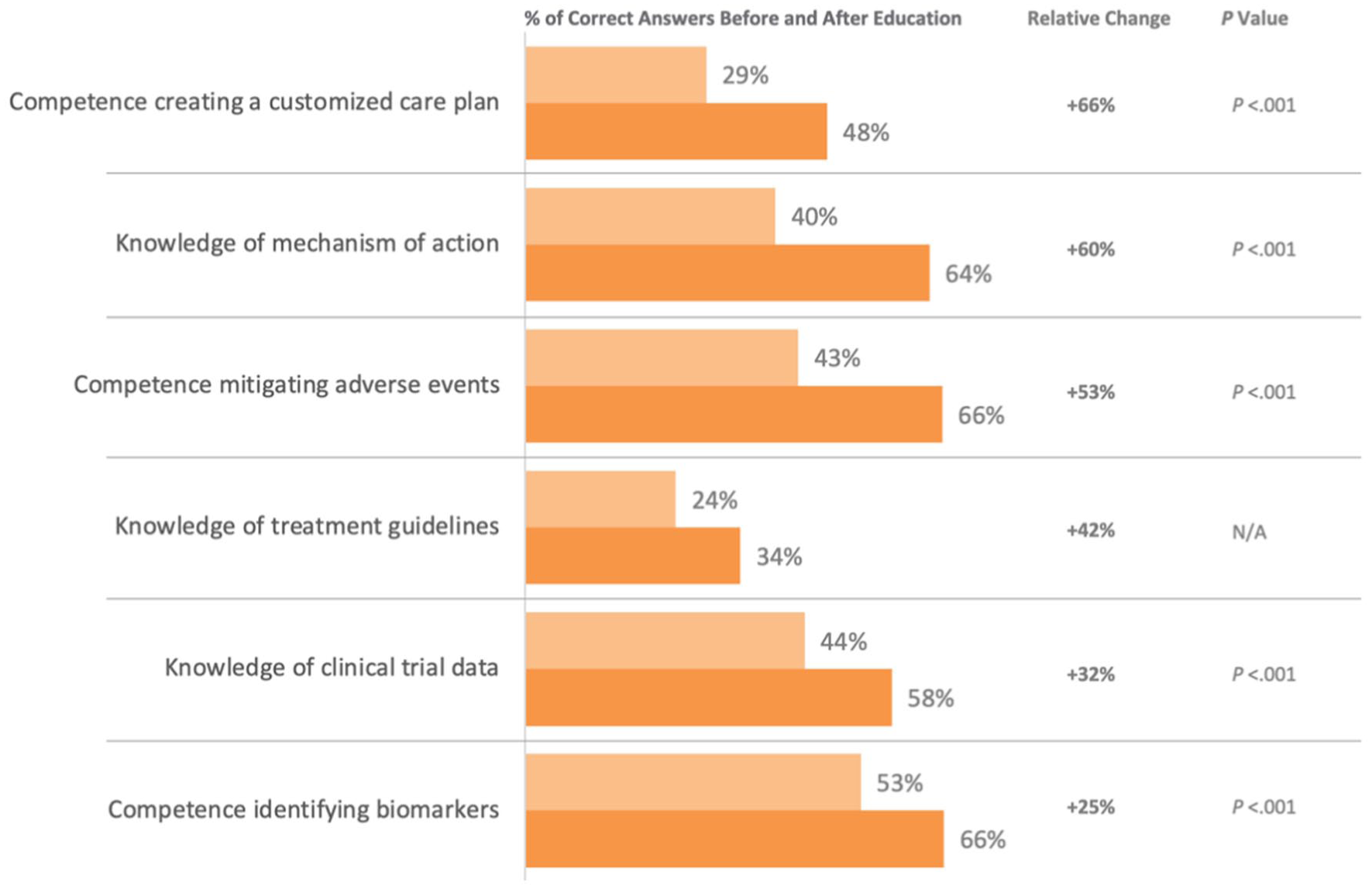
Surgeons’ improvement in knowledge/competence throughout activities.
Radiologists
Radiologists had a +25% relative change in their confidence integrating immunotherapy in their treatment paradigm (4% pre-education, 5% posteducation; P = .285). The percentage of correct answers before and after education increased across all 6 disciplines, with the relative change ranging from +11% to +72%; Figure 3). Competence in mitigating adverse events (P = .033) and knowledge of the mechanism of action (P = .033) were the themes where radiologists had the greatest improvement.
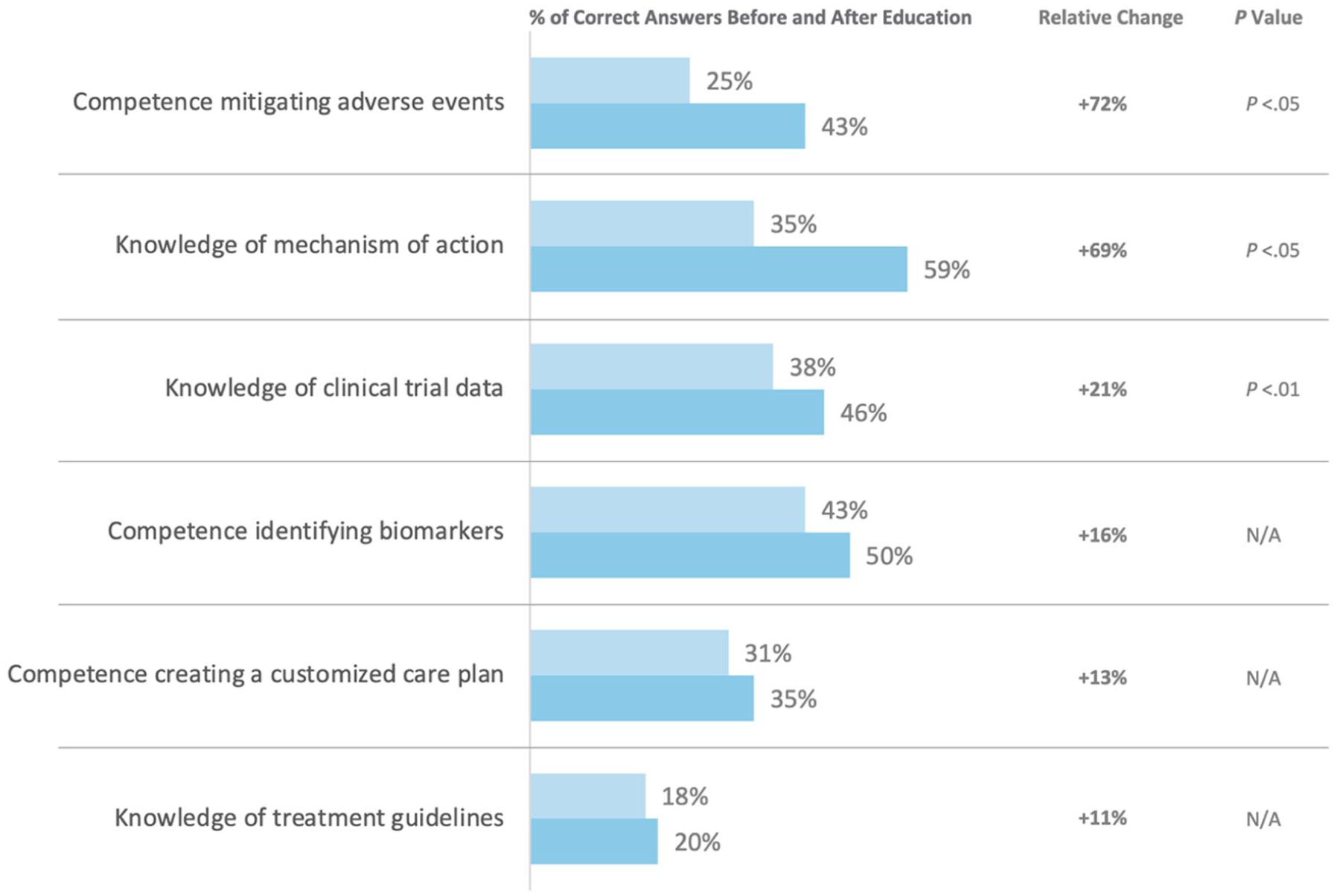
Radiologists’ improvement in knowledge/competence throughout activities.
Pathologists
Pathologists had a +100% relative change in their confidence integrating immunotherapy in their treatment paradigm (3% pre-education, 6% posteducation; P = .003). The percentage of correct answers before and after education increased across all 6 core competencies, with the relative change ranging from +22% to +61%; Figure 4). Knowledge of the treatment guidelines was the only competency where the postcorrect increase 21%-30%) was not significant (P = .180).
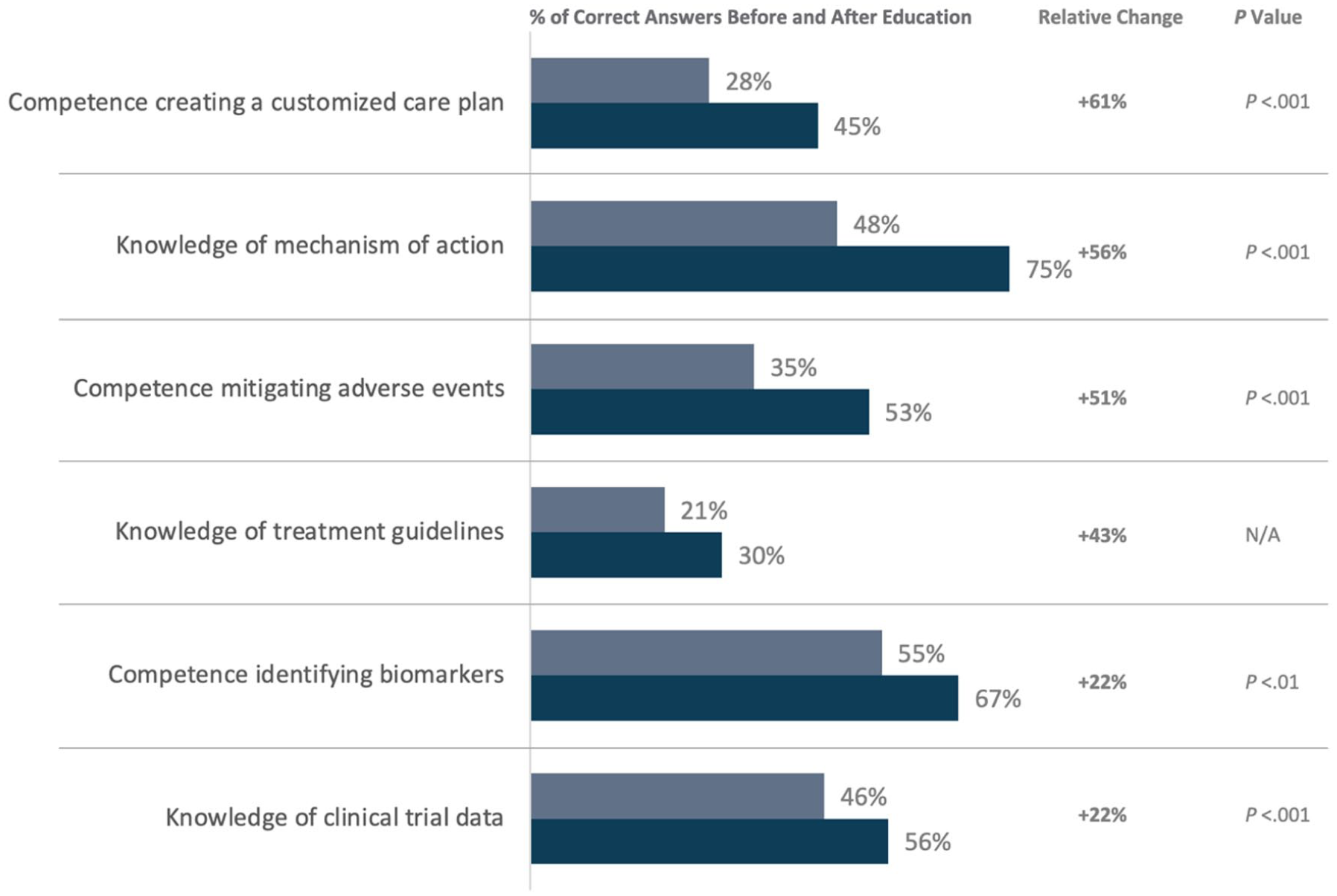
Pathologists’ improvement in knowledge/competence throughout activities.
Overall, most physician participants reported a positive experience. This includes a plan to modify treatment plans (83%), committed to making those changes (93%), and having a positive impact on their practice (86%; Figure 5). Satisfaction rates were high; 91% agreed that the activity supported the achievement of each of the LOs and considered the activity free of commercial bias and 90% would recommend this activity to others. Ninety-five percent confidence intervals (CIs) for all 4 specialty groups by educational theme are presented in Supplemental Table 1.
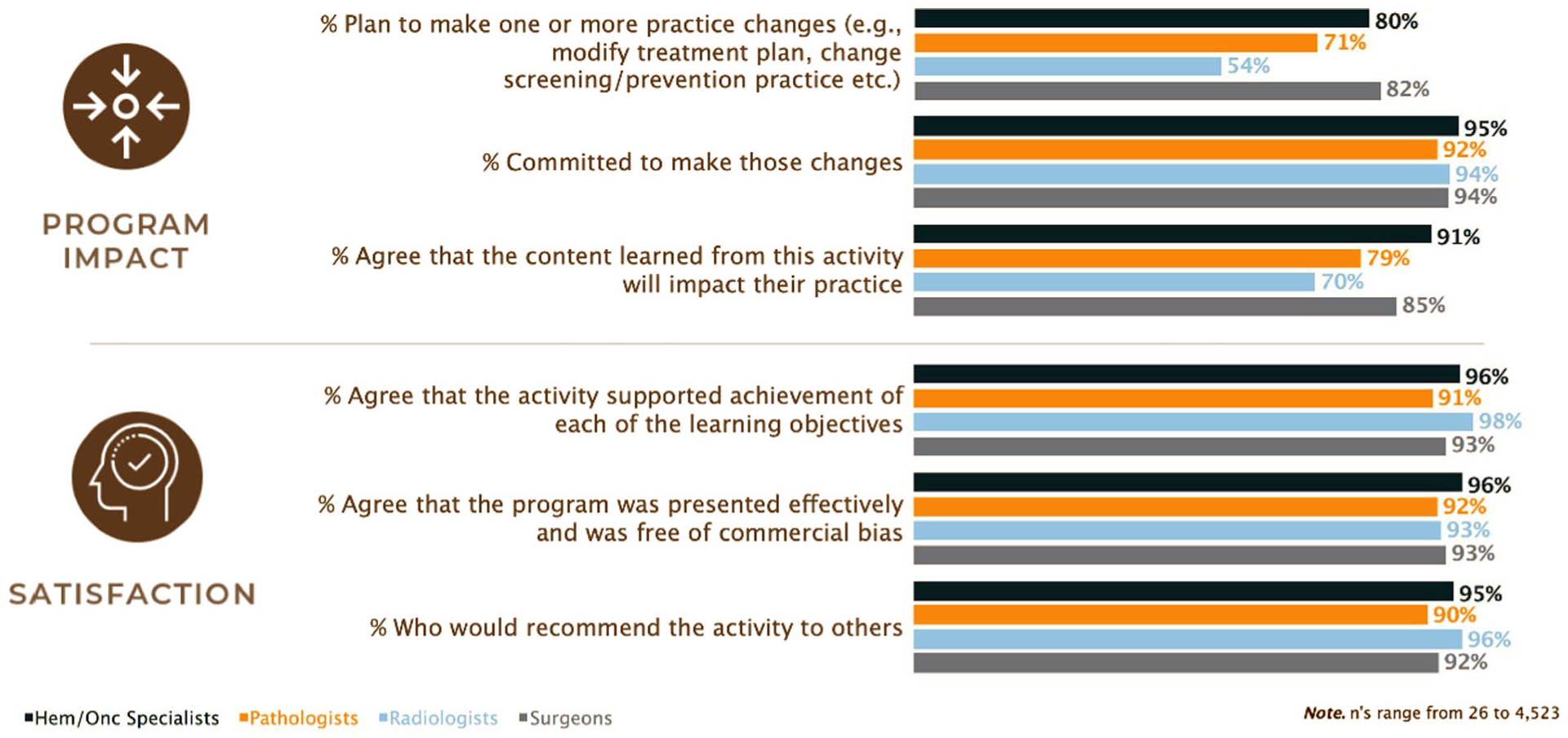
Impact and satisfaction from participating in at least one of the modules, by specialty.
Discussion
The importance of MDTs is increasingly recognized in many disciplines of cancer care.19,20 Efforts have been made to establish HNSCC-specific MDTs with the goal of improving communication and collaboration across the various specialties.13,14,21 However, the implementation of multidisciplinary care remains a challenge, particularly in nontertiary care settings. 15 We aimed to assess the educational impact of an online collaborative curriculum to improve the care of HNSCC patients. Our results demonstrated that participation led to a significant improvement in knowledge and confidence levels across various physician specialties, including surgeons, oncologists, radiologists, and pathologists. These findings suggest that the online modules effectively enhanced the team members’ understanding of key aspects of HNSCC management, which is crucial for providing comprehensive and coordinated care.
The requirement for both pre- and postassessment completion was used to prevent any analytic dilution due to incomplete cases. This, in line with the CONSORT-22 statement 22 ensures that reported gains genuinely reflect knowledge or confidence improvements rather than artifacts of drop-out or partial participation. Given the study’s scale, missing data are minimized by design, and the exclusion of incomplete cases is justified to maintain analytic validity. Real-world educational uptake naturally reflects the distribution of specialties and their clinical engagement with HNSCC. The larger number of oncologists and surgeons versus radiologists/pathologists is true to the MDTs typically involved in head and neck cancer care, validating the external generalizability of the findings. One critical core competency is knowledge of the mechanism of action of different treatments. All physician specialties in this study experienced substantial improvements based on their pre- and postassessment results. It is reasonable to assume that a better understanding of treatment mechanisms empowers team members to make more informed decisions and collaborate more effectively in tailoring treatment plans for individual patients. As expected, oncologists had the highest pre-education baseline and achieved the smallest relative improvements from this core competency. Nevertheless, the gain in other specialists was dramatic. Additionally, both surgeon and oncologists had an increased ability to create a customized care plan. This finding highlights the curriculum’s impact on enhancing critical decision-making skills that are central to the comprehensive care of HNSCC patients. Of note, while CIs are presented (Supplemental Table 1), it is important to acknowledge that this data are subjective and based on participant reports rather than objective measurements or statistical estimates of a population parameter, and thus the CIs are not as informative as in other types of studies.
While our study demonstrated positive outcomes in terms of knowledge, competence, and confidence improvement, certain limitations deserve acknowledgment. We were unable to mandate all participants from completing both the pre- and posttest assessments. Only 41.6% of all participants completed an assessment. While this response rate is typical for a voluntary program, we do not know if the participants who did not complete the assessment would achieve the same level of competence and confidence as the participants who completed the assessment. Also, the lack of long-term follow-up hinders our ability to assess the sustainability of the observed changes in knowledge and practice. Future studies could consider incorporating long-term assessments to determine whether the benefits of the online curriculum endure over time. The study’s effectiveness is limited to the participants’ self-reported intentions to change practice. While self-assessment is valuable, objective measures of clinical practice changes and patient outcomes would provide more robust evidence of the curriculum’s impact on patient care. Randomized control groups or nonintervention arms are not always feasible or ethical in open-access CME, especially as withholding potentially practice-changing education could compromise care quality. However, using each participant as their own control through a pre/postdesign is a gold standard within educational research, allowing for robust paired comparisons and minimizing individual confounders. Further, while selection bias is inherent in voluntary educational studies like the present one, the wide reach of the platform—spanning over 24 000 physicians across multiple specialties—demonstrates a highly representative and impactful real-world sample. Medscape is an internationally recognized platform, not solely U.S.-based, and is routinely accessed by a broad and diverse healthcare audience, including those driven to update their knowledge. The inclusion of motivated, self-directed learners possibly one of the study’s strengths, considering that in actual clinical practice, those who seek continuing education are the practitioners most likely to implement evidence-based improvements, directly benefiting patient care.
Conclusion
Despite these limitations, our study findings are promising as evidenced by the high satisfaction rates and participants’ willingness to change their practice based on newly acquired knowledge. Our findings suggest that the online curriculum can play a vital role in strengthening the MDT approach to HNSCC care. These results may also translate to other cancers who also require MDT interaction. Further research with long-term follow-up and objective outcome measures is warranted to confirm the sustained benefits of such educational interventions. Ultimately, the establishment of well-coordinated MDTs, supported by continuing education, remains crucial in optimizing HNSCC management and improving patient quality of life.
Supplemental Material
sj-docx-1-ear-10.1177_01455613251407707 – Supplemental material for A Multi-Year Collaborative Curriculum Improves Multidisciplinary Team Members’ Ability to Comprehensively Care for Patients With Squamous Cell Carcinoma of the Head and Neck
Supplemental material, sj-docx-1-ear-10.1177_01455613251407707 for A Multi-Year Collaborative Curriculum Improves Multidisciplinary Team Members’ Ability to Comprehensively Care for Patients With Squamous Cell Carcinoma of the Head and Neck by Jason Tasoulas, Haleh Kadkhoda, Charlotte Warren, Davecia Ragoonath-Cameron, Jared Weiss, Jacob Cohen, Michelle A. Worst, Robert L. Ferris and Siddharth Sheth in Ear, Nose & Throat Journal
Footnotes
Ethical Considerations
This article does not contain any studies with human or animal participants.
Author Contributions
Jason Tasoulas: conceptualization, methodology, analysis, manuscript preparation, review and editing. Haleh Kadkhoda: methodology, data collection, analysis, manuscript preparation, review and editing. Charlotte Warren: methodology, data collection, analysis, manuscript preparation, review and editing. Davecia Ragoonath-Cameron: methodology, data collection, analysis, manuscript preparation, review and editing. Jared Weiss: conceptualization, methodology, manuscript review and editing. Jacob Cohen: methodology, data collection, analysis, manuscript preparation, review and editing. Michelle A. Worst: methodology, data collection, analysis, manuscript preparation, review and editing. Robert L. Ferris: conceptualization, methodology, manuscript review and editing. Siddharth Sheth: conceptualization, methodology, manuscript review and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Siddharth Sheth reported personal fees from Naveris, Medscape, and research funding from AstraZeneca, Merck, Inovio, Exelexis, Regeneron. Dr Siddharth Sheth belongs to the speaker’s bureau of Exelexis. Dr Robert L. Ferris reported personal fees from Adagene, Aduro Biotech, Bicara Therapeutics, Brooklyn Immunotherapeutics, Catenion, F. Hoffmann-La Roche, Federation Bio, Genocea Biosciences, Kowa Research Institute, EMD Serono, Everest Clinical Research, Mirati Therapeutics, Nanobiotix, Novartis, PPD, Sanofi, and Zymeworks; grants from AstraZeneca/MedImmune, Bristol-Myers Squibb, Merck, Novasenta, and Tesaro; serving on the advisory boards of Coherus BioSciences, Eisai Europe, Genmab, Hookipa Biotech, Instil Bio, Lifescience Dynamics, MacroGenics, MeiraGTx, Merus, Numab Therapeutics, OncoCyte, Pfizer, Rakuten Medical, Seagen, SIRPant Immunotherapeutics, and Vir Biotechnology; and serving on the data safety monitoring board of Mirror Biologics, all outside the submitted work. No other disclosures were reported.
Data Availability Statement
Data can be made available upon reasonable requests to the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.