
Abstract
In a patient whose sudden vision loss is suspected on the side of a previously operated sphenoid or ethmoid sinus, an ischemic insult to the optic nerve may occur due to a compressing mucocele, especially when there is bony dehiscence of the orbital apex. We report a case of a 41-year-old healthy male patient who had a history of previous sinus surgery, and visited the emergency department for an abrupt left ocular pain following visual loss of the affected eye. The patient’s left eye’s best corrected visual acuity (BCVA) was hand motions with a reduced light reflex. A sphenoethmoidal sinus cell (Onodi cell) mucocele with bone dehiscence in the left orbital apex was seen on computed tomography. Upon suspicion of compressive ischemic optic neuropathy, urgent endoscopy-assisted endonasal marsupialization of the Onodi cell mucocele with high-dose pulse intravenous dexamethasone was performed. The pathology showed an inflamed nasal mucosa, confirming a mucocele. On the second postoperative day, his BCVA slightly improved in counting fingers at 30 cm. However, even though the nasalized Onodi cell remained intact, his eyesight did not show further improvement. The optic nerve may be directly insulted when a mucocele in the Onodi cell takes place, especially when there is bony dehiscence in the orbital apex. Despite accelerated surgical marsupialization and high-dose steroids, the chance of visual recovery remains very low, as demonstrated in our case.
Introduction
Paranasal sinus mucoceles are epithelial-lined mucus sacs that can develop in any paranasal sinuses. 1 In most cases, paranasal sinus mucoceles often do not cause any pain or symptoms and are sometimes incidentally detected by routine head and neck imaging. 2 However, mucus accumulation can lead to an increase in pressure inside the cyst. 3 In some cases of severity, the cyst can lead to the defects of surrounding bony wall, where cystic elements exert direct pressure on adjacent tissues. 4 In cases with such condition, the individual may eventually manifest symptoms, depending on the specific structures that are under compression.2 -4
Here, the authors present a case of acute unilateral optic neuropathy due to an ischemic insult to the optic nerve, which is concluded to have been the result of a direct compression in the orbital apex area caused by a postoperative mucocele in the sphenoethmoidal cell, named as the Onodi cell.
Case Report
A 41-year-old male patient visited the emergency department (ED) with sudden-onset headaches on the left side, left ocular pain, following left visual loss. Other than hypertension, he had no medical history. The patient had a history of receiving bilateral functional endoscopic sinus surgery in the clinic of another surgeon for the treatment of chronic rhinosinusitis with nasal polyp, 12 years before the visit.
The headache and ocular discomfort developed the day before the visit, which worsened followed by sudden blindness in his left vision on the day of his visit to the ED. His vital signs were stable and afebrile with normal white blood cell counts of 7320/µl; however, there a slight elevation in C-reactive protein (CRP) of 1.98 mg/dl was noticed.
The patient was immediately referred to the ophthalmology department. His best corrected visual acuity (BCVA) was 0.9 in the right eye, while the left eye only perceived hand movements. The wide fundus examination of both eyes (Supplemental Figure 1) and intraocular pressures were within the normal range, measured at 11 mm Hg in both eyes by Goldmann applanation tonometer. The optical coherence tomography showed a normal retina and a thickness of the retinal nerve fiber layer on both eyes, indicating that there was no damage to both structures. However, his left pupil was dilated and had a sluggish reaction to light, indicating a relative afferent pupil defect (RAPD). Additionally, there was weak pain when moving the left eyeball with the orbital forceps, indicating an inflammatory condition of the optic nerve or extraocular muscles.
The brain computed tomography (CT) did not show any acute lesion. However, an opacification in the left posterior ethmoid sinus adjacent to the left optic nerve was noticed (Figure 1A). Consequently, the patient was referred to otorhinolaryngology department, and nasal endoscopy showed diffuse nasal polyps mucopurulent discharge on both sides. Afterward, a contrast-enhanced sinus CT scan and a Gd-enhanced magnetic resonance imaging (MRI) were ordered. On contrast-enhanced CT, a non-enhancing cystic lesion was observed in the posteriorly extended ethmoid sinus located above the sphenoid sinus (termed as the Onodi cell) (Figure 1B and C, asterisks). Furthermore, multiple areas of bony dehiscence were observed in the orbital apex, exposing the canalicular segment of the optic nerve and the cavernous segment of the internal carotid artery in direct contact with the cystic lesion (Figure 1B and C, arrowheads). On MRI, the cystic mass in the left Onodi cell showed a low signal intensity (SI) of T1, a high SI of T2, and non-enhancement pattern (Figure 2D and E, asterisks). Noticeably, the left optic nerve exhibited a “flattening sign,” in which the size of the nerve was reduced compared with the contralateral optic nerve (Figure 2D and E, arrows). Taken together, the authors concluded an acute compressive optic neuropathy due to an Onodi cell mucocele compressing the left optic nerve.
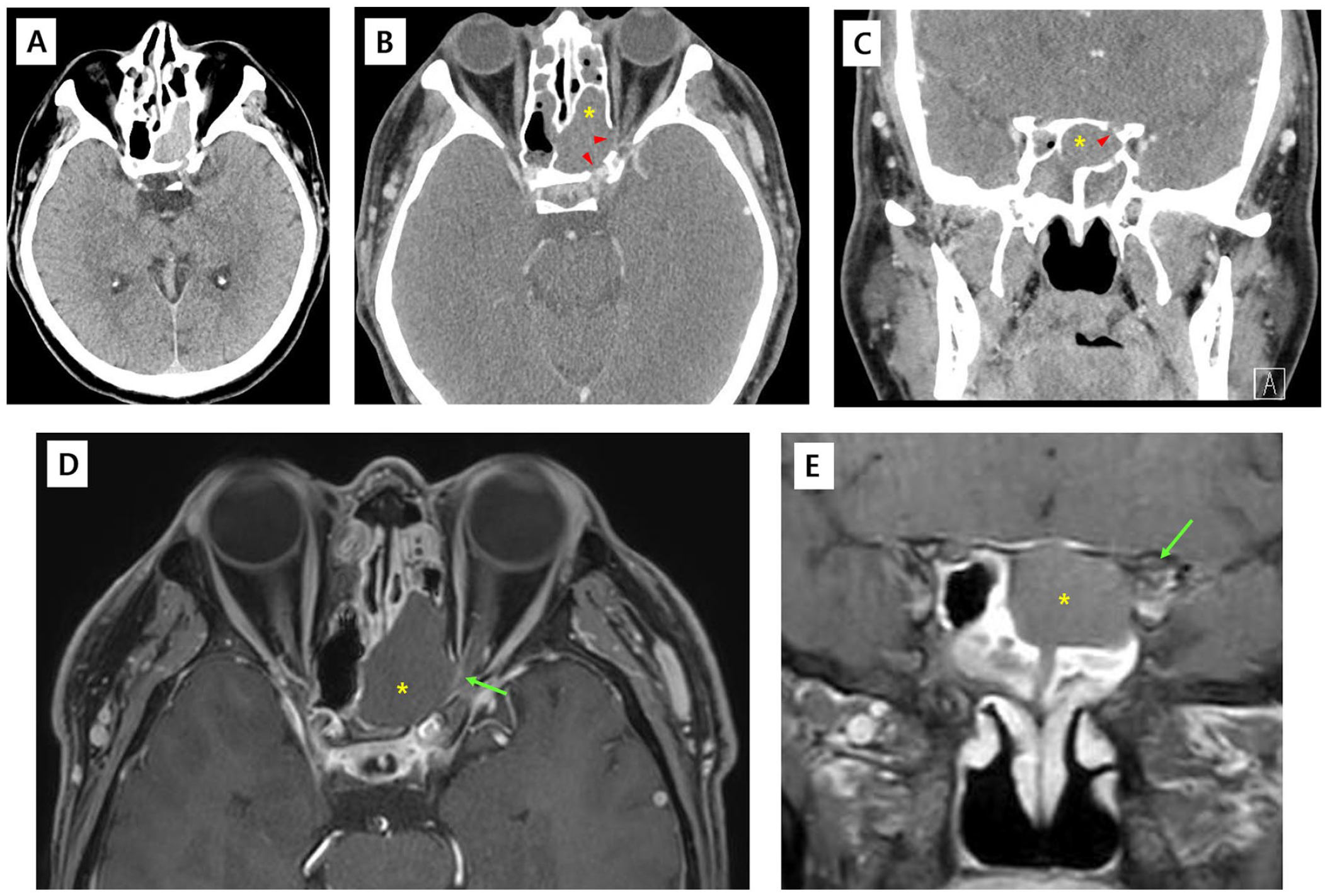
Initial CT and Gd-enhanced MRI of a 41-year-old male with acute visual loss of the left eye. (A) The non-contrast-enhanced brain CT in the emergency department showed no acute hemorrhagic lesion in the intracranial and orbit; however, a dehiscence of posterior wall of left posterior ethmoid sinus filled with opacification was seen. (B and C) A contrast-enhanced CT image reveals a cystic lesion not enhanced within the left posterior ethmoid sinus located above the sphenoid sinus (Onodi cell) (asterisk), showing partial dehiscence and thinning (arrowheads), especially at the orbital apex and posterior aspect, exposing the left optic nerve and cavernous segment of the ICA. (D and E) Gd-enhanced T1-weighted MRI showing the left optic nerve (D and E, arrow) directly in contact with the non-enhancing cystic lesion in the Onodi cell, the flattening of the left optic nerve was notable in the coronal image (E, arrow).
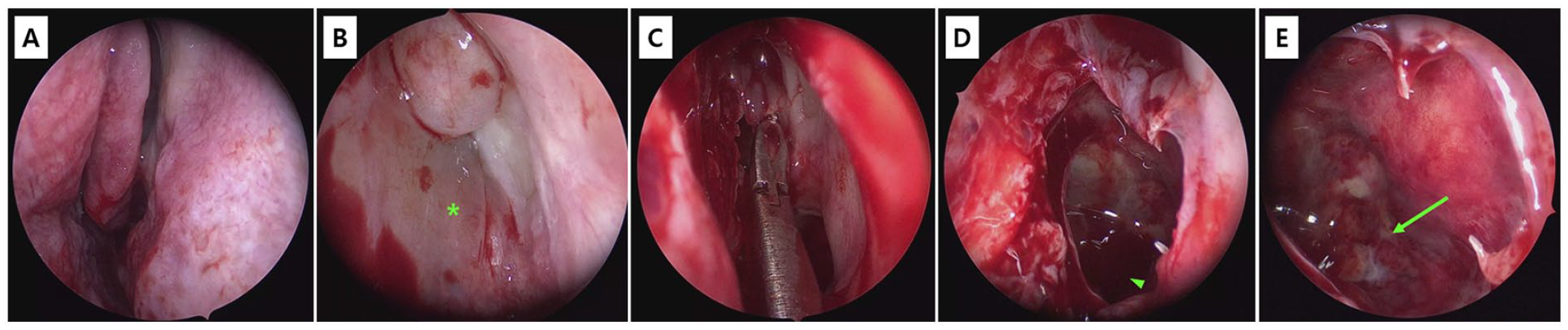
EEM of the sphenoethmoid (Onodi) cell mucocele. A surgical step-by-step image of an urgent EEM of the Onodi cell mucocele to release the intraluminal pressure in the hope of visual recovery has been demonstrated. (A) The left nasal cavity was patent with no mucoid discharge; however, a synechia was observed between the middle turbinate and the lateral nasal wall, following resection of the scar band, opening the middle meatus patency (B). (B) In the left anterior ethmoid sinus, a thick polypoid anterior surface of the mucocele was identified (B, asterisk). (C and E) With Blakesley Nasal Forceps, the anterior and inferior walls of the cyst were completely opened and widened, which led to a brownish-colloid sluggish fluid collection. The accumulated fluid was completely evacuated and the Onodi cell was irrigated with normal saline. (E) The mucosa of the posterolateral portion of the mucocele showed areas of severe purulence and inflammation, especially located in the bony dehiscence area of the orbital apex (E, arrow).
Thus, an urgent endoscopic endonasal marsupialization (EEM) and mucocele decompression under general anesthesia was performed (Figure 2A-E). Briefly, the mucocele located in the left posterior ethmoid sinus was identified, and the anteroinferior wall of the cyst (Figure 2B) was completely marsupialized with cutting forceps and microdebriders, with a brownish-sluggish fluid collection was identified (Figure 2D) and complexly evacuated. A paired swab culture was carried out on the accumulated fluid inside the mucocele, but no bacterial growth was detected. After the evacuation of fluid contents, a reddish-swollen mucosa with focal areas of pyoceles and purulence were identified, particularly in the superior posterolateral aspect within the cystic lesion (Figure 2E), where purulence was completely eradicated with saline irrigations. The resected cystic wall was sent for pathology, which later showed a nasal mucosal epithelium densely infiltrated with neutrophils and lymphocytes, confirming the diagnosis of an inflamed mucocele.
During the same time, a high-dose intravenous (IV) steroid pulse was initiated, in which 250 mg of IV methylprednisolone (MP) was administered every 6 hours, for 3 days after 6 weeks of tapering with oral MP. Additionally, the patient was given 2 g of IV ceftriaxone daily during hospital stay for 3 days, which was converted to 2 weeks of 500 mg amoxicillin with tablets of 125 mg clavulanic acid three times a day.
Immediately after surgery, there were no changes in patient visual acuity. On postoperative day (POD), 1 all non-absorbable nasal packing materials were removed, and the patient was asked to apply an intranasal fluticasone furoate spray twice a day with daily nasal rinse. On POD, 2 BCVA was improved to counting fingers at a distance of 30 cm (CF30) with subsiding pain, whereas RAPD persisted. On POD, 3 the patient was discharged.
Despite prompt treatment, the patient’s visual acuity was still CF30 at POD 2 months after the completion of systemic steroid therapy. The patient was prescribed to maintain the administration of the intranasal steroid for up to 1 year, to prevent re-stenosing of the nasalized ethmoid sinus. Although there was no recurrence of the mucocele on the CT scan (Figure 3A and B, asterisks), and the nasalized patency of the ethmoid sinus was secured (Figure 3C, arrowheads), some scar changes in the mucosa covering the optic nerve were noticed (Figure 3D, arrow), and his visual acuity did not show further improvement at 1-year follow-up.
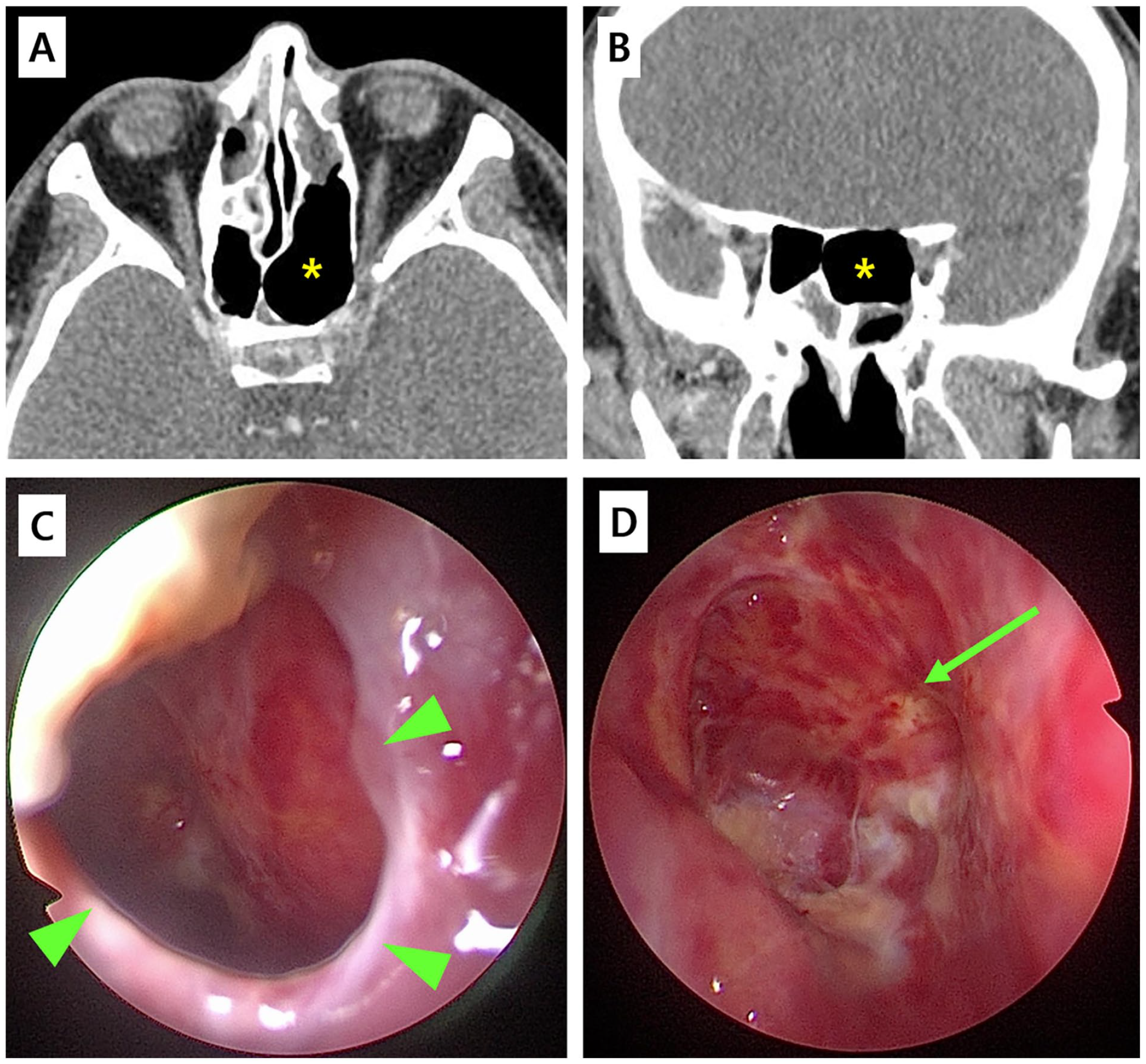
A 1-year postoperative outcome following EEM of the sphenoethmoid (Onodi) cell mucocele. (A and B) On contrast-enhanced CT, it is observed that the opacification in the posterior ethmoid sinus (Onodi cell) has been completely evacuated and void (A and B, asterisk), showing no signs of mucosal thickening in the Onodi cell. (C and D) In nasal endoscopy, the marsupialized anterior wall of the mucocele (opened and widened) was well intact (C, arrowheads), and the posterior ethmoid sinus (Onodi cell) was fully communicated with the nasal cavity, showing the mucosa covering the optic nerve (D, arrow).
Discussion
In cases of rapidly developing unilateral optic neuropathy, possible etiologies can be demyelinating disorders, focal inflammation on the optic nerve or nerve sheath, trauma, and ischemia. 5 In our case, the mucocele situated within the Onodi cell exhibited direct contact with the optic nerve through bony dehiscence at the orbital canal and orbital apex. This observation highlights the possibility of ischemic, infectious, or inflammatory conditions within the mucocele to directly affect the optic nerve, as many previous literatures have identified this association as “rhinogenic optic neuritis.”6 -9
One possible etiology is that the enlarged mucocele may directly put pressure on the optic nerve or impede its blood supply, resulting in the development of optic atrophy.10,11 An additional aspect to take into account is the possible impact of inflammation inside the contents of the Onodi cell mucocele. The focal inflammation on the Onodi cell mucosa might possibly directly spread via a bony dehiscence area in the orbital apex, ultimately resulting in the development of optic neuropathy, as some literature states this condition as “rhinogenic optic neuropathy.”8,9 Although the mucocele content did not display a definite purulence, there were some mucosal swellings with focal areas of pyoceles, especially in the posterolateral aspect of the Onodi cell mucosa, which is adjacent to the optic canal and optic nerve (Figure 2E, arrow). Also, the extraocular discomfort and modest CRP elevation may further support the presence of a concomitant inflammatory condition. Thus, an ischemic insult due to compression and a direct spread of inflammation may have resulted in the acute visual loss in our case.
In patients presenting with an orbital complication due to a paranasal sinus mucocele directly in contact with orbital contents, a surgical intervention is indicated, whereby the walls of these cystic lesions are surgically removed and widened, a process called “marsupialization” of the mucoceles.2 -4 In previous investigations, a more profound visual loss upon symptom initiation was associated with poorer visual recovery, and the shorter duration of less than 24 hours between symptom initiation and the implementation of surgical drainage has significantly affected better visual recovery.4,12 However, their analysis concluded that urgent surgery might not be sufficient to recover the patient’s vision, suggesting the possibility of other factors associated with visual recovery, thus requiring further investigation. 12
Moreover, regarding the extent and invasiveness of the surgical intervention, most previously published cases had the drainage of the mucocele, 4 while few authors proposed a more extensive surgical approach of including an optic nerve decompression.7,8 In retrospect, a consecutive optic nerve decompression might have improved in better visual recovery. However, whether optic nerve decompression is necessary in patients who do not respond to EEM or presenting with substantial vision loss shall be elucidated in future investigations.
Conclusion
Our case demonstrates a patient with abrupt vision loss on the side of a previously operated ethmoid sinus, in which an acute optic neuropathy was concluded as a result of a compressing mucocele in the Onodi cell. Despite accelerated surgical marsupialization and high-dose corticosteroid administration, the likelihood of visual recovery remains very low.
Supplemental Material
sj-tif-1-ear-10.1177_01455613231214705 – Supplemental material for Sudden Unilateral Visual Loss Due to an Onodi Cell Mucocele
Supplemental material, sj-tif-1-ear-10.1177_01455613231214705 for Sudden Unilateral Visual Loss Due to an Onodi Cell Mucocele by Yong Jun Yoo, Gyu Tae Kim and Marn Joon Park in Ear, Nose & Throat Journal
Footnotes
Authors’ Contributions
Concept and design: Marn Joon Park; Acquisition, analysis, or interpretation of data: All authors; Drafting of the manuscript: Yong Jun Yoo and Marn Joon Park; Critical revision of the manuscript for important intellectual content: Marn Joon Park; Administrative, technical, or material support: Yong Jun Yoo and Gyu Tae Kim; Supervision: Marn Joon Park.
Availability of Data and Materials
All relevant data are included in the manuscript. The raw clinical and image data used and analyzed during the current study available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
Inha University Hospital institutional review board (IRB) authorized this study (Investigation No.: 2023-08-005).
Consent for Publication
The IRB waived the patient’s informed consent requirement, due to the retrospective study design and absence of any personal identifiable information.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.