
Abstract
Rhinogenic optic neuropathy (RON) results from ethmoid or sphenoid sinus inflammation or infection causing optic nerve impairment. 1 Treatment often requires endoscopic surgery and vision restoration occurs in select cases. There is no clear evidence for the benefit of optic nerve decompression (OND) in these situations. We present a unique case of RON caused by an Onodi cell mucocele for which isolated endoscopic mucocele drainage was not enough and further OND was needed to improve vision.
Keywords
Case Report
A 63-year-old patient with a history of chronic rhinosinusitis with nasal polyps (CRSwNP) and sinus surgery 30 years ago presented to the emergency department with acute right-sided visual loss. While awaiting treatment, he noted the shadow of a curtain over the inferior visual field. He also had dull eye pain on medial and lateral gaze. Examination was significant for visual acuity of 20/800 eccentrically, a 1+ afferent pupillary defect (APD), decreased color saturation, full ocular motility, and normal intraocular pressure (IOP). His external examination was unremarkable without proptosis or compartment syndrome. Nasal elevation of right optic nerve head and temporal pallor was seen on dilated fundus examination.
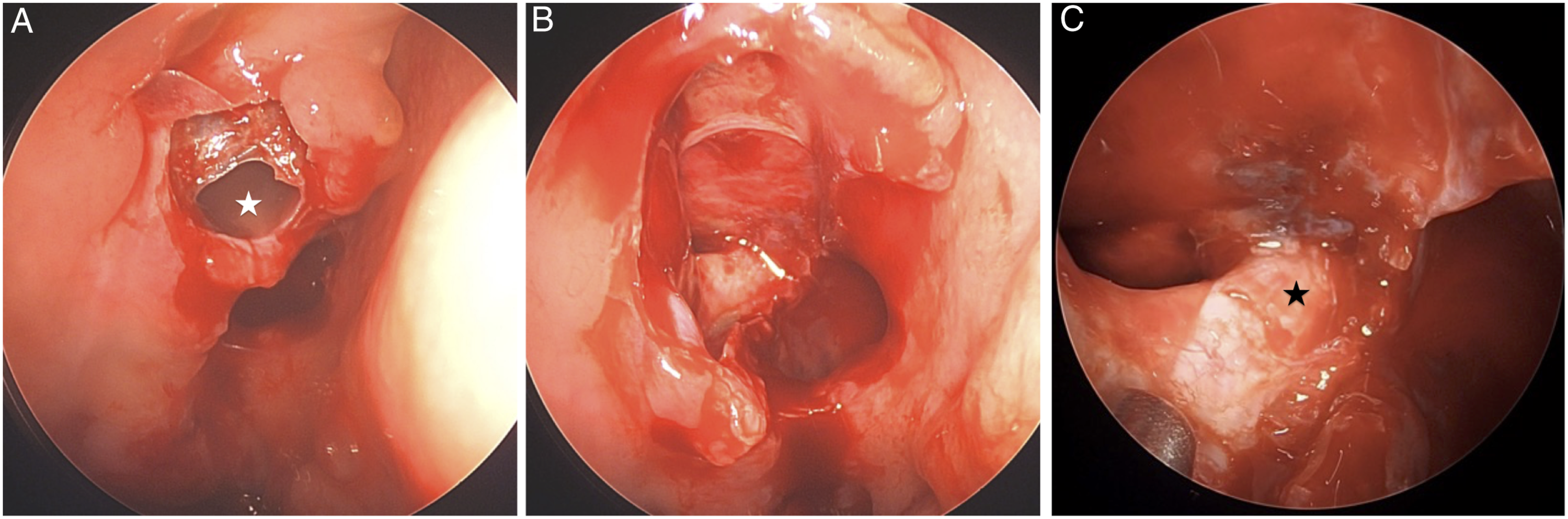
Computed tomography (CT) and magnetic resonance imaging (MRI) demonstrated a large right posterior ethmoid mucocele with associated dehiscence of the posterior orbital roof, right optic canal, and right anterior clinoid process. Additionally, there was mass effect and compression on the intracanalicular segment of right optic nerve (Figures 1A-C). He was placed on systemic antibiotics, and additional workup for inflammation was negative. The otolaryngology team was subsequently consulted, and the patient’s vision had deteriorated to no light perception (NLP). Decision was made to perform endoscopic right posterior ethmoidectomy, right sphenoidotomy, and drainage of right orbito-ethmoid mucocele for decompression of the optic nerve (Figures 2A and B). The preoperative computed tomography (CT) imaging demonstrates a large right posterior ethmoid mucocele with associated dehiscence of the right optic canal and compression of the intracanalicular segment of right optic nerve on both axial view A, and coronal view B. Magnetic resonance imaging (MRI) demonstrates increased signal and compression of the right optic nerve on T2 axial view with contrast C. Postsurgical CT shows persistent compression of intracanalicular segment of the right optic nerve in the right optic nerve canal from bony dehiscence of the medial wall D. The white star denotes the Onodi cell, and the white arrow points to the bony dehiscence abutting the optic nerve. The black star marks the course of the optic nerve. The intraoperative view shows the right posterior ethmoid mucocele with a white star centered in the mucocele A. After decompression, the ethmoid skull base, lamina papyracea, and sphenoid sinus are seen superiorly, laterally, and posteriorly, respectively, B. The intraoperative endoscopic view after right optic nerve decompression shows bone removed from the entire medial portion of the optic nerve with a black centered on the optic nerve C.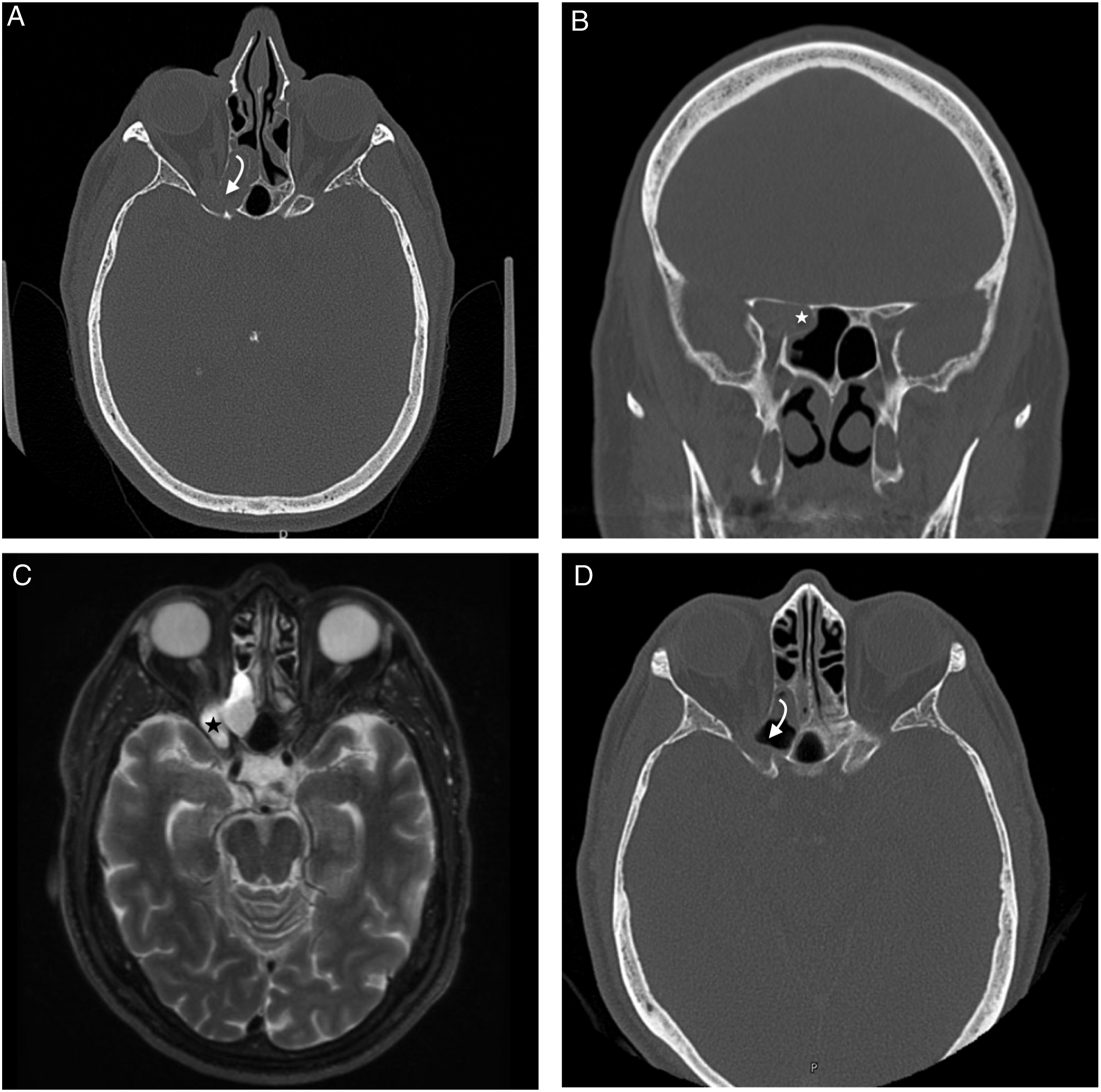
The following morning, the patient reported light perception and decreased right eye pain. However, given the continued visual deficit, a repeat CT orbits was ordered for concern of need of further decompression. This demonstrated persistent compression of the intracanalicular segment of the right optic nerve from bony dehiscence of medial wall (Figure 1D). The patient was taken again for endoscopic right orbital apex and optic nerve decompression (Figures 2C and D). The periorbita and annulus of Zinn were incised, and orbital fat was allowed to herniate into the nasal cavity. The postoperative CT demonstrated adequate medial decompression of the optic nerve (Figures 3A and B). The following two days, prior to discharge, the patient had further visual field improvement, first with perception to hand motion and then the development of peripheral vision. On the postoperative visit at five weeks, the patient demonstrated visual improvement to 20/60 with a residual relative pupillary afferent defect. The computed tomography (CT) imaging after optic nerve decompression demonstrates a medially decompressed optic nerve on axial A, and coronal B slices. The white arrow points to the medial aspect of the optic nerve.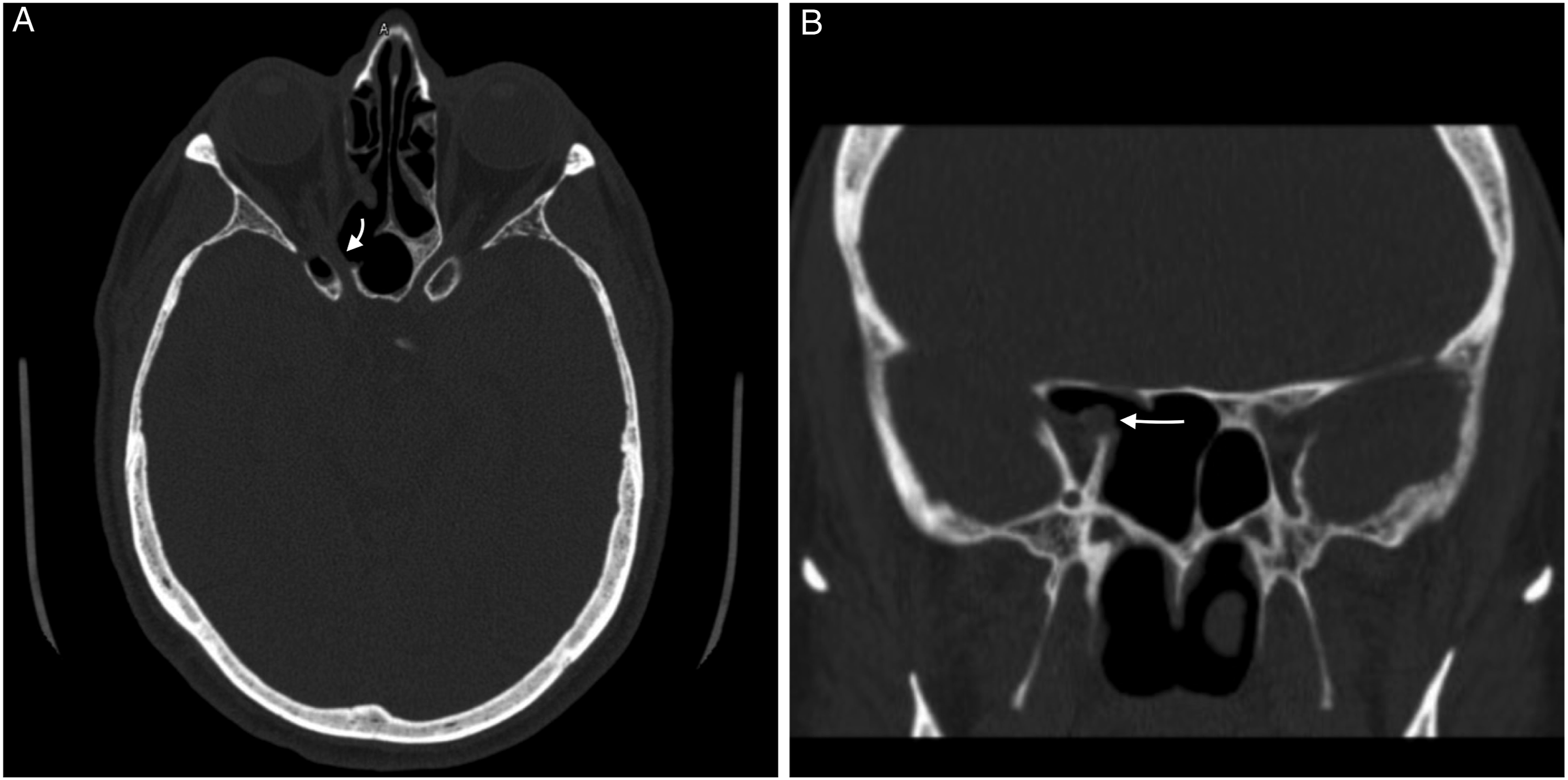
Discussion
The urgency and extent of endoscopic sinus surgery for RON, particularly for patients with NLP, is poorly defined. Otsuka et al 1 investigated the impact of ethmoid or sphenoid mucocele drainage on postoperative visual acuity for RON in 15 patients. Factors associated with clinical improvement included younger age and preoperative visual acuity. A recent study of RON demonstrated the time from visual symptom onset to surgery and headache are significantly associated with visual recovery. 2 Interestingly, Neo et al 3 presented a case of RON and NLP in a patient with a dehiscent Onodi cell without an associated mucocele who experienced visual recovery after OND. They suggest the adjacent sinus cell bony dehiscence may lead to spread of inflammation to the optic nerve. In our case, the patient developed NLP secondary to an Onodi cell mucocele with lateral dehiscence, and isolated mucocele drainage was inadequate. While the evidence is limited, vision loss from RON may be multifactorial from both compression and inflammation disseminating through the bony dehiscence.3,4 While there are no literature-based timing cutoffs for OND timing after RON, there is some insight from research on traumatic optic neuropathy (TON). In a retrospective study by Wohlrab et al, 5 4/9 (44.4%) of patients with NLP secondary to TON recovered vision after OND within 48 hours of injury compared to 1/7 (14.3%) who underwent decompression after 48 hours of injury. They suggest performing decompression within 48 hours of injury to improve visual outcomes. 5 Cases of NLP secondary to RON may benefit from a similarly expeditious approach.
Given the sparse evidence and the correlation of visual recovery with preoperative deficit in patients with RON, it is important to consider OND, in additional to mucocele drainage, for cases with NLP, particularly if there is imaging evidence for optic nerve compression or contiguous sinus cell inflammation and dehiscence.
Footnotes
Author Contributions
Noah Shaikh, MD: study design, acquisition of data, data analysis and interpretation, manuscript drafting, and critical revision, John Nguyen, MD: acquisition of data, data analysis and interpretation, manuscript drafting, and critical revision, Christopher Eric Bailey, MD, PhD: acquisition of data, data analysis and interpretation, and critical revision, Ami Patel, MD: acquisition of data, and data analysis and interpretation, Brian Ellis, MD: acquisition of data, and data analysis and interpretation, Chadi A. Makary, MD: study design, acquisition of data, data analysis and interpretation, manuscript drafting, and critical revision.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This case report was reviewed and determined exempt by the institutional review board (IRB) of West Virginia University (WVU).