
Abstract
Keywords
Introduction
Optical coherence tomography (OCT) is a noninvasive imaging modality that uses near-infrared light to obtain cross-sectional, high-resolution images of living tissues. OCT can image biologic tissues with penetration depths up to 2 mm and imaging resolutions ranging between <1 and 20 µm, permitting visualization of tissue morphology and individual cells. Furthermore, OCT can be used as a real-time imaging modality that operates without the need for contrast or ionizing radiation. Due to these characteristics, it is a useful imaging technique for studying biologic tissues and monitoring response to pharmacologic interventions.1,2
While tabletop OCT systems are commonly used for imaging external tissues, endoscopic OCT probes and microscope-integrated OCT devices have been designed for accessing internal structures, including those of the ears, nose, and throat. Within the field of otolaryngology, these OCT systems have been experimentally applied for diagnosing laryngeal and oral cancer and for studying the middle and inner ear.3-5 To date, only a few studies have utilized OCT for imaging the sinonasal mucosa in patients. OCT may be particularly well-suited for intranasal use due to its ability to be performed in the confines of the nasal cavity and provide direct, noninvasive, and high-resolution imaging of mucosal morphology and inflammatory cell infiltration.
OCT is now recognized as the standard of care for the diagnosis of retinal diseases and is also frequently used within the field of cardiology for endovascular imaging.6,7 While OCT is commonly used within these fields because of its ability to improve diagnostic accuracy and impact clinical decision-making, it remains unclear if this technology can provide similar benefits when investigating the sinonasal mucosa.6,7 Therefore, the objectives of this systematic review are to summarize the current applications and potential uses of OCT for evaluating sinonasal pathologies in patients and identify gaps requiring additional research.
Methods
The Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) statement was followed. 8 Studies using OCT to image the sinonasal cavity mucosa were identified from the PubMed, Embase, Cochrane Library, Web of Science, and Scopus databases by searching for all published articles from inception until January 2023. The following search phrase was used in each of the databases: “Optical Coherence Tomography” AND (sinonasal OR intranasal OR sinus OR nose OR sinusitis OR rhinitis OR olfactory). Protocol registration for this systematic review was not performed.
The titles and abstracts of all retrieved articles were screened by 2 reviewers (IB and JR). Original research studies including randomized controlled trials, non-randomized prospective studies, retrospective cohort and case-control studies, case series, case reports, and conference proceedings were included for full-text review if they reported on the use of OCT for imaging the sinonasal mucosa of human patients in vivo. After full-text review, studies which only reported imaging of animal or human tissues ex vivo or in vitro were excluded. Studies which utilized OCT to image other aspects of the sinonasal cavity, including the internal nasal valve, eustachian tube, or airway cross-sectional area without imaging the sinonasal mucosa were also excluded. Finally, studies were excluded if they reported on non-original research, were published in a language other than English, did not report a sample size or were not peer reviewed.
The included studies were independently evaluated by 2 reviewers (IB and JR) to assess the strength of evidence according to the Oxford Centre for Evidence-Based Medicine 2011 guidelines. 9 The quality of evidence was evaluated according to the Grading of Recommendations Assessment, Development and Evaluation (GRADE) guidelines. 10 Risk of bias was evaluated using the Joanna Briggs Institute (JBI) critical appraisal tool specific for each study’s design. 11 Disagreements on these measures were resolved by discussion, and a third reviewer (KH) was consulted if necessary. Information collected from each study included sample size, OCT device, lateral and axial resolutions, study objectives, and main qualitative and quantitative findings related to OCT imaging. The included studies were qualitatively analyzed. Pooling of data and meta-analysis was not performed due to the clinical heterogeneity of the included articles.
Results
A total of 2620 studies were identified in the literature search, including 1662 original records after removing duplicates. After title and abstract screening, 1600 articles were excluded as they were determined to not report on OCT use for imaging the sinonasal mucosa of patients in vivo. Full-text review of the remaining 62 studies resulted in 53 articles meeting our exclusion criteria and 9 articles being included in qualitative analysis. A summary of the article selection process and reasons for exclusion can be found in the PRISMA flow diagram (Figure 1). 8 For articles which reported results from multiple diagnostic modalities, only findings related to OCT imaging are described in this review. The study design, sample size, level of evidence, GRADE, JBI score, OCT device, imaging resolutions, study objectives, and main findings of each study are summarized in Table 1. Quantitative results are expressed as means ± standard deviation. α was set at .05 for statistical significance in all included studies.
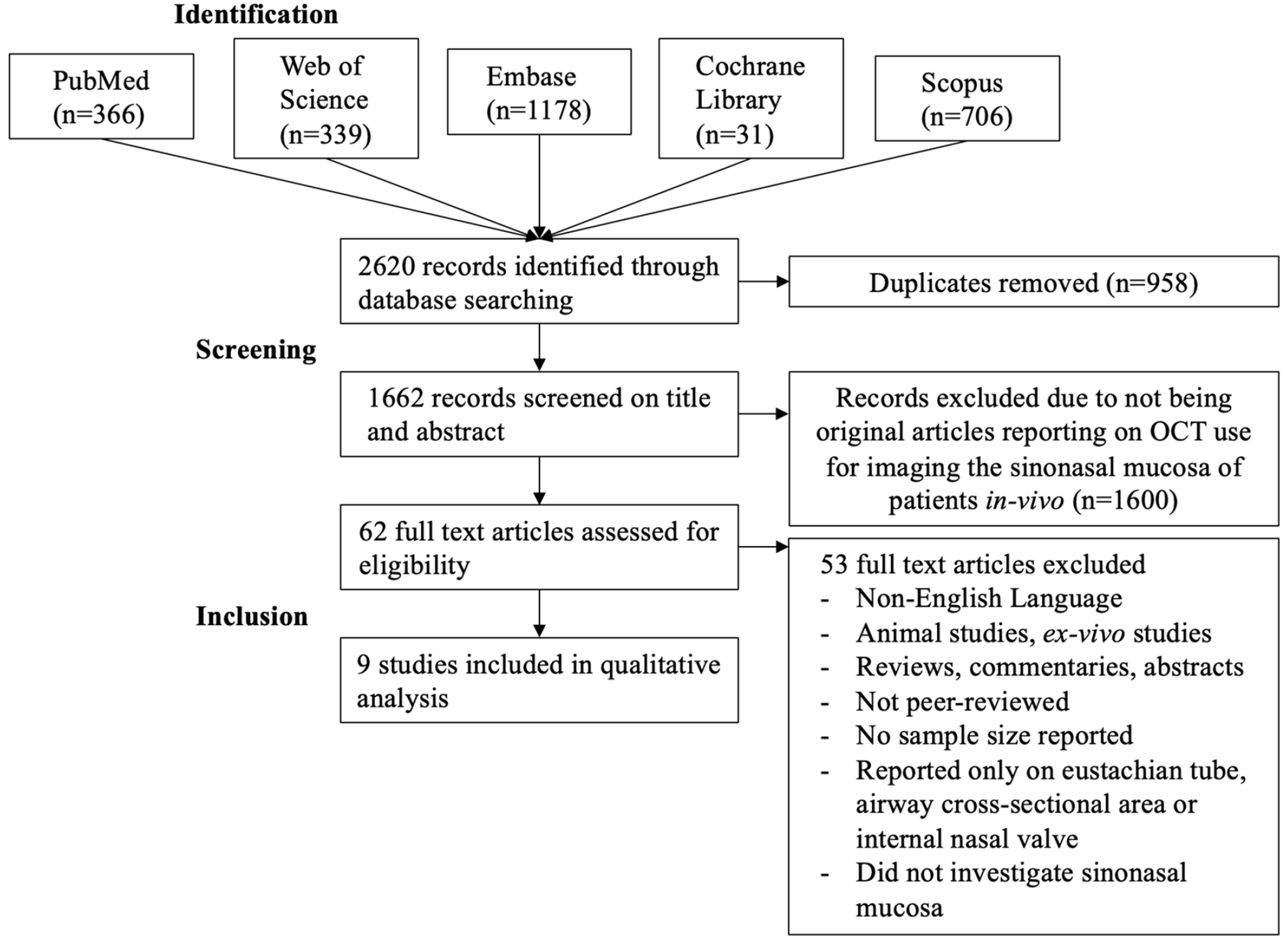
PRISMA flow diagram.
Summary of the Included Studies.
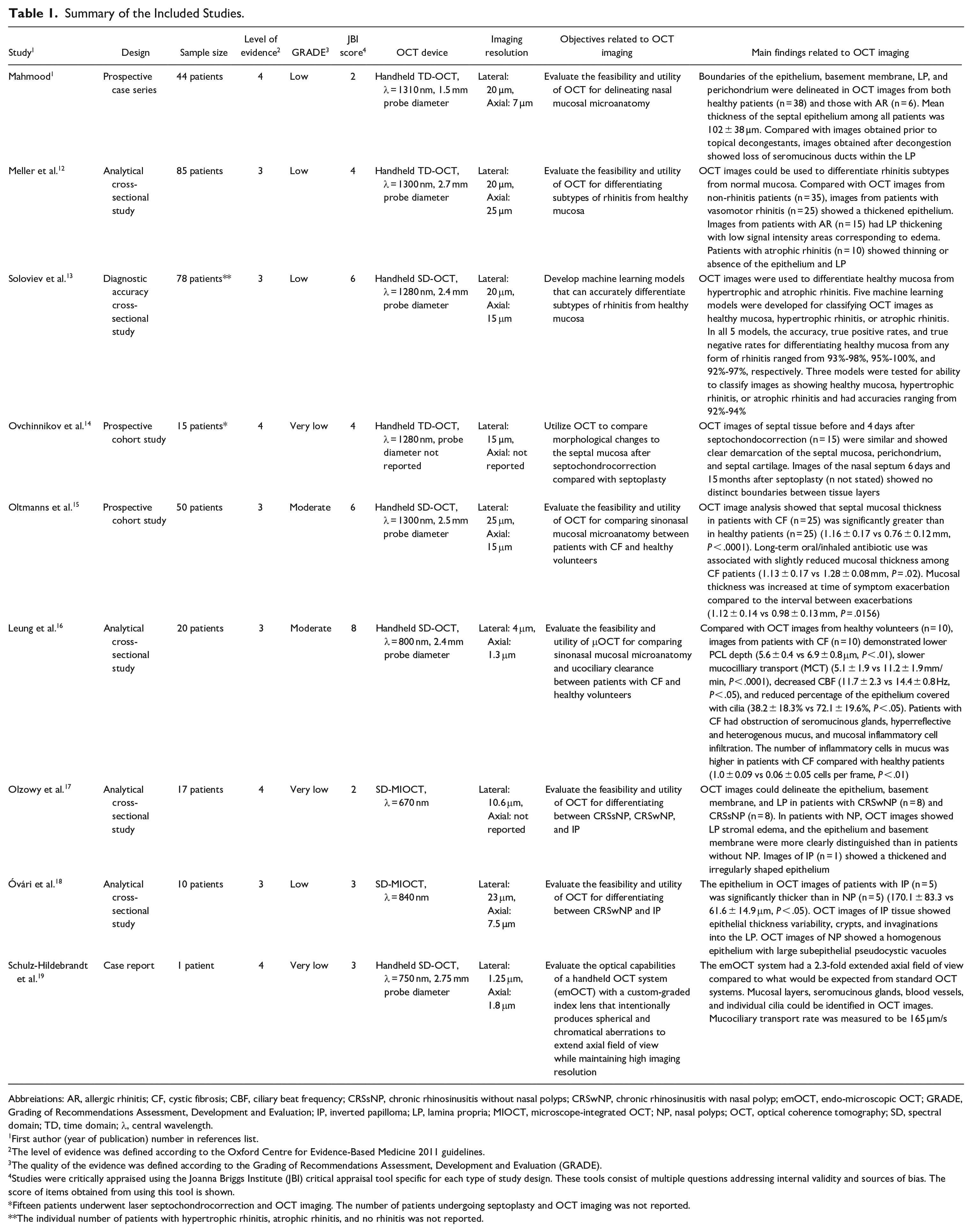
Abbreiations: AR, allergic rhinitis; CF, cystic fibrosis; CBF, ciliary beat frequency; CRSsNP, chronic rhinosinusitis without nasal polyps; CRSwNP, chronic rhinosinusitis with nasal polyp; emOCT, endo-microscopic OCT; GRADE, Grading of Recommendations Assessment, Development and Evaluation; IP, inverted papilloma; LP, lamina propria; MIOCT, microscope-integrated OCT; NP, nasal polyps; OCT, optical coherence tomography; SD, spectral domain; TD, time domain; λ, central wavelength.
First author (year of publication) number in references list.
The level of evidence was defined according to the Oxford Centre for Evidence-Based Medicine 2011 guidelines.
The quality of the evidence was defined according to the Grading of Recommendations Assessment, Development and Evaluation (GRADE).
Studies were critically appraised using the Joanna Briggs Institute (JBI) critical appraisal tool specific for each type of study design. These tools consist of multiple questions addressing internal validity and sources of bias. The score of items obtained from using this tool is shown.
Fifteen patients underwent laser septochondrocorrection and OCT imaging. The number of patients undergoing septoplasty and OCT imaging was not reported.
The individual number of patients with hypertrophic rhinitis, atrophic rhinitis, and no rhinitis was not reported.
Identifying Structural Changes in Rhinitis
A study by Mahmood et al. 1 utilized a handheld OCT probe to study the structural microanatomy of the nasal septum in 44 patients, including 6 with allergic rhinitis (AR) and 38 healthy patients. Most patients were imaged in the operating room under general anesthesia (86.4%) while the remainder were imaged in the clinic. OCT images delineated the boundaries of the epithelium, basement membrane, lamina propria (LP), and the perichondrium in healthy patients and those with AR. The mean thickness of the septal epithelium among all patients measured 102 ± 38 µm. To determine if OCT could identify medication-induced morphological changes to the septal mucosa, the authors performed intranasal OCT imaging before and immediately after administration of topical decongestants. When compared with images prior to decongestion, post-decongestant images demonstrated loss of microstructural elements within the LP, including seromucinous glands and ducts. The authors concluded that clinical use of intranasal OCT could potentially provide objective information to diagnose rhinitis and evaluate response to pharmacologic therapy.
In 2014, Meller et al. 12 conducted a study using OCT to differentiate between normal nasal mucosa and changes associated with vasomotor, allergic, and atrophic rhinitis. For this study, OCT imaging of the inferior turbinate was performed in the clinic in 15 patients with AR, 25 patients with vasomotor rhinitis, 10 patients with atrophic rhinitis, and 35 patients without rhinitis. Compared with OCT images of patients without rhinitis, imaging of patients with vasomotor rhinitis demonstrated a thickening of the epithelial layer, which the authors speculated may have been due to epithelial hyperplasia and goblet cell hypersecretion. Patients with AR had thickening of the LP with areas of low signal level, consistent with LP edema, while imaging of patients with atrophic rhinitis demonstrated thinning or absence of the epithelium and LP. These findings suggested that intranasal OCT imaging could potentially be used to differentiate rhinitis subtypes.
A study by Soloviev et al. 13 utilized machine learning models to classify rhinitis subtypes based on OCT images. The inferior turbinates of 78 patients, including healthy patients as well as those diagnosed with chronic rhinitis, were imaged. In total, 65 OCT images of normal sinonasal mucosa, 68 images of patients with hypertrophic rhinitis and 68 images from patients with atrophic rhinitis were analyzed. Compared with OCT images of healthy mucosa, images from patients with hypertrophic rhinitis demonstrated thickening of the epithelium and LP disorganization, while those from patients with atrophic rhinitis showed thinning or disappearance of the epithelium. The authors subsequently developed and trained 5 machine learning models to differentiate between healthy mucosa and different rhinitis subtypes using OCT images. All 5 models had true positive and negative rates of 92% or greater for differentiating healthy mucosa from any form of rhinitis, and 3 of the 5 models had accuracies of 92% or greater for correctly classifying images as showing healthy mucosa, hypertrophic rhinitis, or atrophic rhinitis. The results of this study provided preliminary evidence that OCT imaging could be used in combination with machine learning to noninvasively and automatically diagnose rhinitis subtypes.
Postprocedural Imaging of the Nasal Septum
Ovchinnikov et al. 14 utilized OCT to identify morphological changes to the septal mucosa after performing laser septochondrocorrection, a technique which uses a nondestructive laser to reshape the nasal septal cartilage. The study utilized a clinic-based intranasal OCT system to image the septal mucosa in 15 patients with septal deviation and nasal obstruction before and 4 days after undergoing septochondrocorrection. The authors also reported OCT findings from patients 6 days and 15 months after undergoing conventional septoplasty, although the number of patients who underwent septoplasty and OCT imaging was not reported. OCT images of septal tissue before and 4 days after septochondocorrection were similar in appearance and showed clear demarcation of the septal mucosa, perichondrium, and cartilage. By contrast, OCT images of the nasal septum obtained 6 days and 15 months after septoplasty revealed indistinguishable boundaries between these tissue layers. This study’s findings suggested that OCT could be used to evaluate morphological changes to the septal microanatomy after various procedures.
Evaluating Structural Changes and Mucociliary Clearance in Cystic Fibrosis
Oltmanns et al. 15 assessed the feasibility of intranasal OCT for measuring mucosal thickness in patients with cystic fibrosis (CF) by imaging the nasal septum in 25 patients with CF and 25 healthy patients in the clinic. The thickness of the septal mucosa in OCT images of patients with CF was significantly greater than in healthy patients (1.16 ± 0.17 vs 0.76 ± 0.12 mm, P < .0001), and long-term oral or inhaled antibiotic therapy among CF patients was associated with slightly reduced mucosal thickness compared with patients who did not receive antibiotics (1.13 ± 0.17 vs 1.28 ± 0.08 mm, P = .02). Moreover, the thickness of the nasal mucosa was significantly increased in patients at the time of symptom exacerbation compared to the stable interval between exacerbations (1.12 ± 0.14 vs 0.98 ± 0.13 mm, P = .0156). Based on these results, the researchers supported the feasibility of intranasal OCT for evaluating mucosal thickness in patients with CF as a proxy for assessing structural airway damage and monitoring response to antibiotics.
A 2019 study by Leung et al. 16 reported on the use of a high-resolution micro-OCT (μOCT) probe for evaluating sinonasal microanatomy and measurement of mucocilliary clearance (MCC) parameters, including airway surface liquid, periciliary liquid (PCL), ciliary beat frequency (CBF), and mucocilliary transport (MCT), in patients with CF. An intranasal μOCT probe was used to image the inferior turbinate and nasal floor in 10 patients with CF and 10 healthy volunteers in the clinic. Compared with healthy volunteers, patients with CF had significantly lower PCL depth (5.6 ± 0.4 vs 6.9 ± 0.8 μm, P < .01), slower MCT (5.1 ± 1.9 vs 11.2 ± 1.9 mm/min, P < .0001), decreased CBF (11.7 ± 2.3 vs 14.4 ± 0.8 Hz, P < .05), and reduced percentage of the epithelium covered with cilia (38.2 ± 18.3% vs 72.1 ± 19.6%, P < .05). OCT images also revealed that patients with CF had obstruction of seromucinous glands, hyperreflective mucous, and in-flammatory cell infiltration in the mucosa. The mean number of inflammatory cells in the sinonasal mucus was significantly higher in patients with CF compared with healthy volunteers (1.00 ± 0.09 vs 0.06 ± 0.05 cells per frame, P < .01). Overall, the study demonstrated that intranasal µOCT was capable of noninvasively evaluating MCC and morphological features of CF sinonasal disease in the clinic.
Differentiating Nasal Polyps From Inverted Papilloma Based on Tissue Morphology
Olzowy et al. 17 utilized a surgical microscope with an integrated OCT system to compare morphological differences in the sinonasal mucosa of patients with inverted papilloma (IP), chronic rhinosinusitis with nasal polyps (CRSwNP) and CRS without nasal polyps (CRSsNP) in the operating room under general anesthesia. A total of 17 patients were included in the study, including 1 patient with IP, 8 with CRSwNP, and 8 with CRSsNP. Compared with images of patients with CRSsNP, OCT images of nasal polyps (NP) demonstrated increased stromal edema of the LP, while OCT images of IP revealed a thickened epithelium with pronounced thickness variability. The study provided preliminary evidence that OCT imaging could potentially differentiate CRSsNP, CRSwNP, and IP based on mucosal morphology.
In 2018, the same group performed a second study investigating the feasibility of a microscope-integrated OCT system for differentiating IP from CRSwNP. 18 Five patients with IP and 5 with CRSwNP were imaged in the operating room under general anesthesia, and the histology slides served as the gold standard. OCT images demonstrated that the epithelium in IP was significantly thicker than in NP (170.1 ± 83.3 vs 61.6 ± 14.9 μm, P < .05). Additionally, OCT images of IP tissue could visualize epithelial thickness variability as well as the presence of crypts and invaginations into the LP. OCT imaging of NP demonstrated subepithelial pseudocystic vacuoles and minimal epithelial thickness variability. The authors concluded that in vivo OCT imaging could potentially be used to distinguish IP from CRSwNP based on differences in epithelial thickness.
Optimizing OCT Image Resolution and Field of View
Developing high-resolution intranasal OCT systems is difficult because of the tradeoff between high image resolution and reduced field of view. With a small field of view, any movement by the patient or the operator results in image displacement. As a solution to this problem, Schulz-Hildebrandt et al. 19 developed an endo-microscopic OCT (emOCT) system with a graded index lens that intentionally produces spherical and chromatical aberrations. These aberrations change the focal position of light beams traveling at different angles and wavelengths, leading to a longer field of view without a large drop-off in resolution. This emOCT system had a 2.3-fold extended field of view compared to what would be expected from standard OCT systems with the same lateral and axial resolutions. emOCT images of the middle turbinate clearly demonstrated seromucinous glands, blood vessels, and individual cilia, and MCT was measured to be 165 µm/s by tracking the lateral motion of mucus. The study’s findings suggested that the increased resolution and larger field of view of the emOCT system could be used to visualize cellular structures and measure MCT in the sinonasal mucosa.
Discussion
This is the first systematic review to summarize the reported uses of OCT for imaging the sinonasal mucosa in patients. Based on examples from the literature, OCT imaging can visualize structural and cellular features of the sinonasal mucosa unique to multiple pathologies, including rhinitis, IP, and CF, and detect changes in the microscopic features of these diseases after pharmacologic therapies and procedures. Intranasal OCT can also be used to measure parameters of MCC and provide objective evidence of ciliary dysfunction. However, most studies in this systematic review had low levels of evidence, lacked a control group, or did not report objective results that were comparable between studies. Therefore, while these studies highlight possible uses of this technology, no conclusions can be made about the benefits of OCT for improving diagnostic accuracy and guiding clinical decision-making for sinonasal pathologies.
While nasal endoscopy and computed tomography are commonly utilized to diagnose sinonasal disorders based on gross anatomic findings, these modalities cannot visualize more subtle changes to mucosal morphology. Currently, the only method to obtain this information is with histologic evaluation of excised tissue. Therefore, most studies included in this systematic review investigated the feasibility of OCT for noninvasively acquiring information about microstructural elements in the sinonasal mucosa that would be comparable to histologic evaluation for facilitating disease diagnosis and evaluating treatment response.1,12,15-19 This may be particularly advantageous for differentiating subtypes of rhinitis, since diagnosis and management decisions are typically made based on history and physical examination alone due to a lack of useful imaging modalities.1,12,13 Future applications may also include noninvasively differentiating endotypes of CRS, detecting microscopic evidence of sinonasal or nasopharyngeal carcinoma, and diagnosing invasive fungal sinusitis.
A unique application of intranasal OCT is objectively measuring MCC. 16 MCC is the primary method of pathogen removal in the sinonasal cavity, and dysfunctional MCC is thought to be a key process underlying inflammatory airway diseases, including primary ciliary dyskinesia, CRS, and CF. 20 Currently, there are a limited number of methods available for quantitatively assessing MCC dysfunction and investigating the pathophysiology of inflammatory airway disorders noninvasively. The intranasal μOCT system utilized by Leung et al. 16 to simultaneously evaluate multiple MCC parameters in patients represented the clinical translation of a benchtop high-resolution OCT system which has been extensively utilized to investigate CRS, CF, and their treatments ex vivo.16,20-27 Since dysfunctional MCC represents one of the earliest findings of these sinonasal diseases, intranasal μOCT may enable clinicians to obtain a diagnosis and intervene earlier in the disease course. Furthermore, having the ability to objectively measure changes to MCC may permit clinicians to detect early treatment response in patients who have not yet reported symptomatic improvement.
Intranasal OCT has limitations that limit its effectiveness and utility. OCT systems with handheld probes that fit in the sinonasal cavity are not yet commonly available, and high-resolution intranasal systems need to be custom designed. While high-resolution OCT systems are desirable for obtaining more accurate information about mucosal morphology and measures of MCC, the small field of view is disadvantageous when examining awake patients due to patient and operator motion. 19 Furthermore, the small field of view creates a risk of sampling bias, as imaging small areas may lead to missing relevant information in other locations and misdiagnosing patients. Developing a narrow OCT probe with a high-resolution and extended field of view was the objective of one of the studies included in this systematic review and may contribute to improved diagnostic applications of intranasal OCT in the future. 19
Conclusions
The current body of research on OCT imaging of the sinonasal mucosa in patients consists mostly of low-level evidence, including case reports, small case series, and pilot studies. While OCT imaging may be a useful supplemental modality for diagnosing sinonasal disorders, studying disease pathophysiology, and monitoring response to treatments in the future, additional high-quality studies are necessary to determine if the use of OCT to image the sinonasal mucosa in patients can improve diagnostic accuracy and impact clinical decision-making.
Footnotes
Acknowledgements
None.
Availability of Data and Materials
All referenced studies may be found in their respective publication sources.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval is not applicable for this article.
Statement of Human and Animal Rights
This article does not contain any human or animal subjects.
Statement of Informed Consent
There are no human subjects in this article and informed consent is not applicable.