
Abstract
Neurofibromatosis type 1 (NF-1), a hereditary disease caused by a mutation of a gene on chromosome 17q11.2, is associated with manifestations in several organs. Although infrequent, vascular abnormalities are a complication of NF-1, and they are the second most common cause of death in patients with NF-1. Repairing the nutrient artery and achieving hemostasis are difficult once the artery has failed, thereby resulting in poor treatment outcomes. Herein, we report a case of a patient with NF-1 who presented with an enormous cervical hematoma caused by bleeding from a branch of the external carotid artery. Vascular embolization was performed initially; however, rebleeding from the embolized site occurred. Following the removal of the hematoma, drainage tube placement was effective in preventing micro-bleeding. Thus, drainage tube placement may be an effective treatment option in patients with rebleeding.
Introduction
Neurofibromatosis type 1 (NF-1), a hereditary disease caused by germline mutations in the NF1 tumor suppressor gene, 1 is characterized by the presence of a variety of lesions in several organs, including the head and neck. Vascular involvement is a known complication of NF-1. Although infrequent, with its incidence ranging from 0.4% to 6.4%, 2 vascular complications may lead to massive hemorrhage, which may result in death. Herein, we report the case of a patient with an enormous cervical hematoma caused by bleeding from a branch of the external carotid artery treated successfully with drainage tube placement.
Case Presentation
Our institution waived the requirement of ethical approval as this was a case report. Written informed consent was obtained from the patient for the publication of this case report and accompanying images. The patient, a 72-year-old woman, had a history of drooping face since childhood; however, NF-1 remained undiagnosed since she did not seek treatment. She was transported to the hospital via an ambulance after noticing a sudden swelling in the submandibular region while showering. Her vital signs were stable at the time of admission, with no abnormalities, such as signs of anemia or abnormal coagulation, detected in the laboratory results. However, multiple neurofibromas on her trunk and face and hyperpigmented patches similar to café-au-lait spots were observed. Contrast-enhanced computed tomography (CT) revealed hemorrhage of a branch of the external carotid artery. Thus, bleeding from the tumor vessels associated with NF-1 was suspected (Figure 1). Although laryngeal edema was not observed at admission, her larynx started to swell further. Therefore, nasal intubation was performed in anticipation of possible laryngeal edema since the swelling of the submandibular region had increased rapidly. Vascular embolization was performed on the day after the visit to the hospital. Increased tortuousness of the vessels and contrast leakage from a branch of the right external carotid artery were observed (Figure 2A). The right external carotid artery was coiled peripherally, and the embolic material was injected intra-arterially on the proximal side (Figure 2B). Although further enlargement was halted, the swelling persisted. Progressive anemia was observed on the ninth day of hospitalization, and contrast-enhanced CT performed subsequently revealed rebleeding from the embolized site. Since vascular embolization could not achieve hemostasis and surgical intervention was challenging, an open wound was created in the submandibular region. Numerous blood clots were removed, and the wound was cleaned daily (Figure 3). Bleeding was observed on the day after washing, necessitating the need to consider further procedures to achieve hemostasis. Ultrasonography revealed the compression of the trachea by the tumor; therefore, a longitudinal incision was placed above it. The presence of numerous abnormal blood vessels and fragile tissue in the adipose tissue running in a web-like pattern complicated tracheostomy. Nevertheless, tracheostomy and wound closure were performed on the 19th day of hospitalization. As achieving hemostasis via normal hemostatic methods, such as ligation or cauterization, was difficult, the subcutaneous tissue and anterior cervical muscles were sutured using absorbable sutures. Consequently, hemostasis was achieved by the compression of the tissue by the muscle. In addition, a hemostatic matrix was applied on the lower surface, which aided in achieving hemostasis. Lastly, drainage tubes were placed for the management of micro-bleeding, and the surgery was terminated (Figure 4A). The duration of surgery was 1 hour and 10 minutes, and the bleeding volume was 130 mL. A biopsy of the tumor wall performed concurrently led to the diagnosis of neurofibroma (Figure 4B). No bleeding was observed subsequently, and the drainage tube was removed 2 weeks after the surgery.
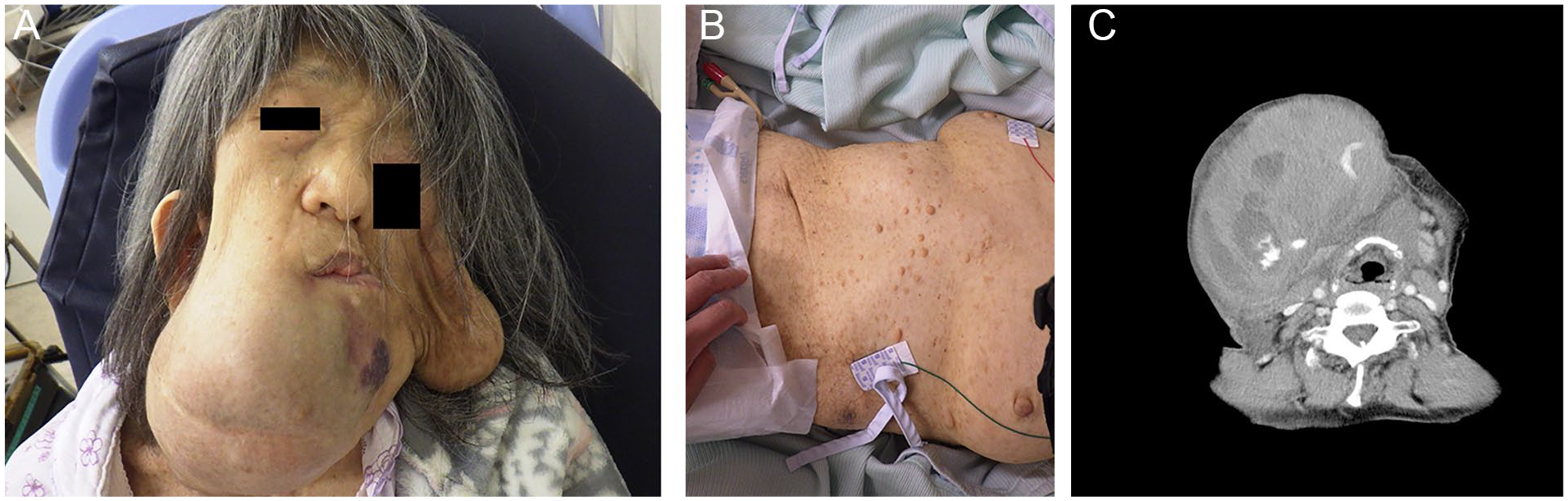
(A) The right submandibular region showed marked swelling on arrival at our hospital; however, no signs of tension were present. Drooping of the left side of the face was observed, in addition to multiple neurofibromas on the trunk and café-au-lait spots. (B) A significant increase in the submandibular swelling was observed in addition to tension after 5 hours. Pallor of the skin was also observed. (C) Contrast-enhanced computed tomography revealed hemorrhage of the branch of the external carotid artery and multiple hematomas.
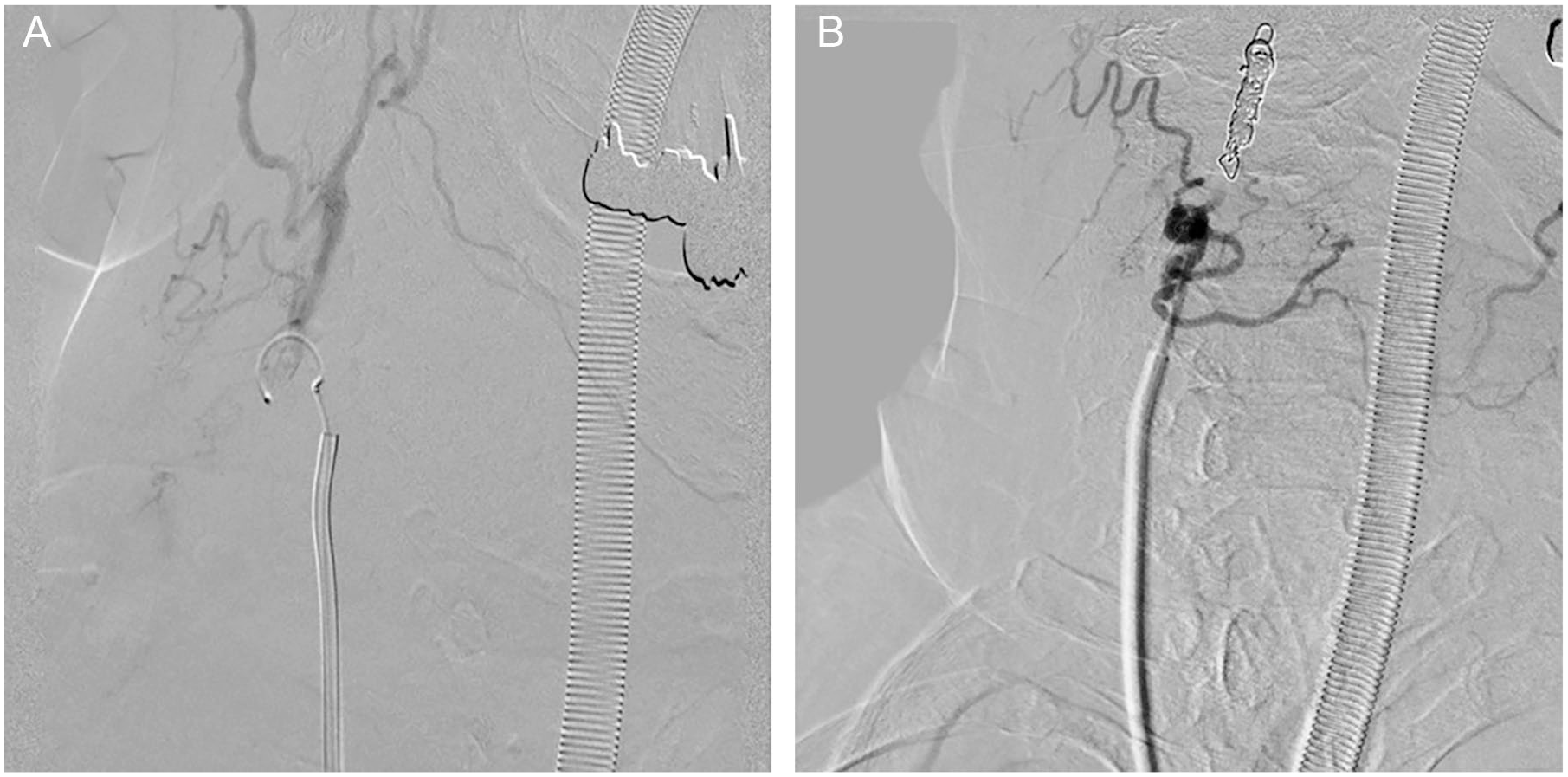
Angiography revealed the presence of tortuous vessels and contrast leakage from a branch of the right external carotid artery. (A) The right external carotid artery was coiled peripherally and (B) the embolic material was injected intra-arterially on the proximal side.
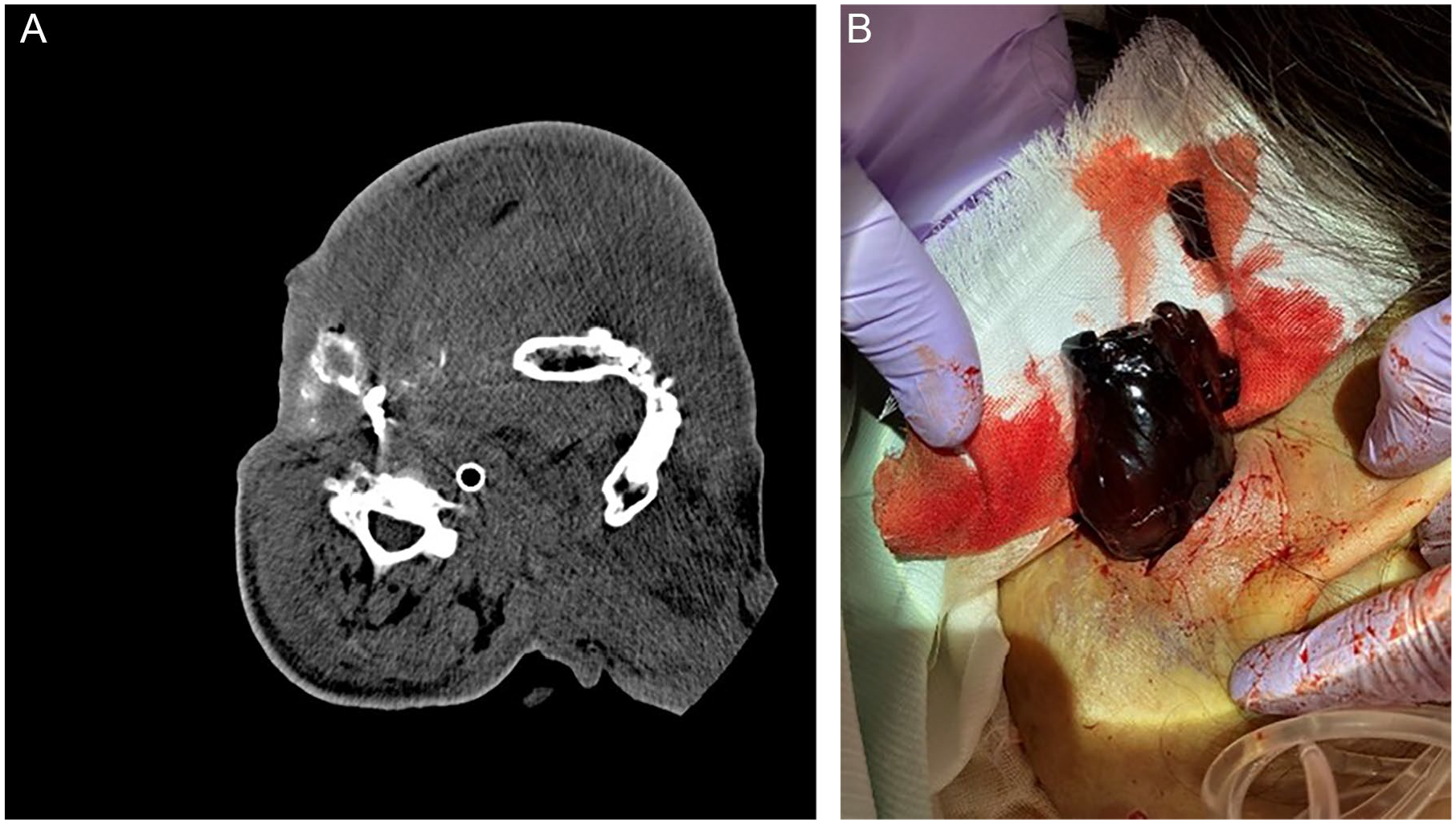
(A) Contrast-enhanced computed tomography performed on the ninth day of hospitalization revealed rebleeding from the embolized site. (B) Several blood clots were removed after reopening the wound in the submandibular region.
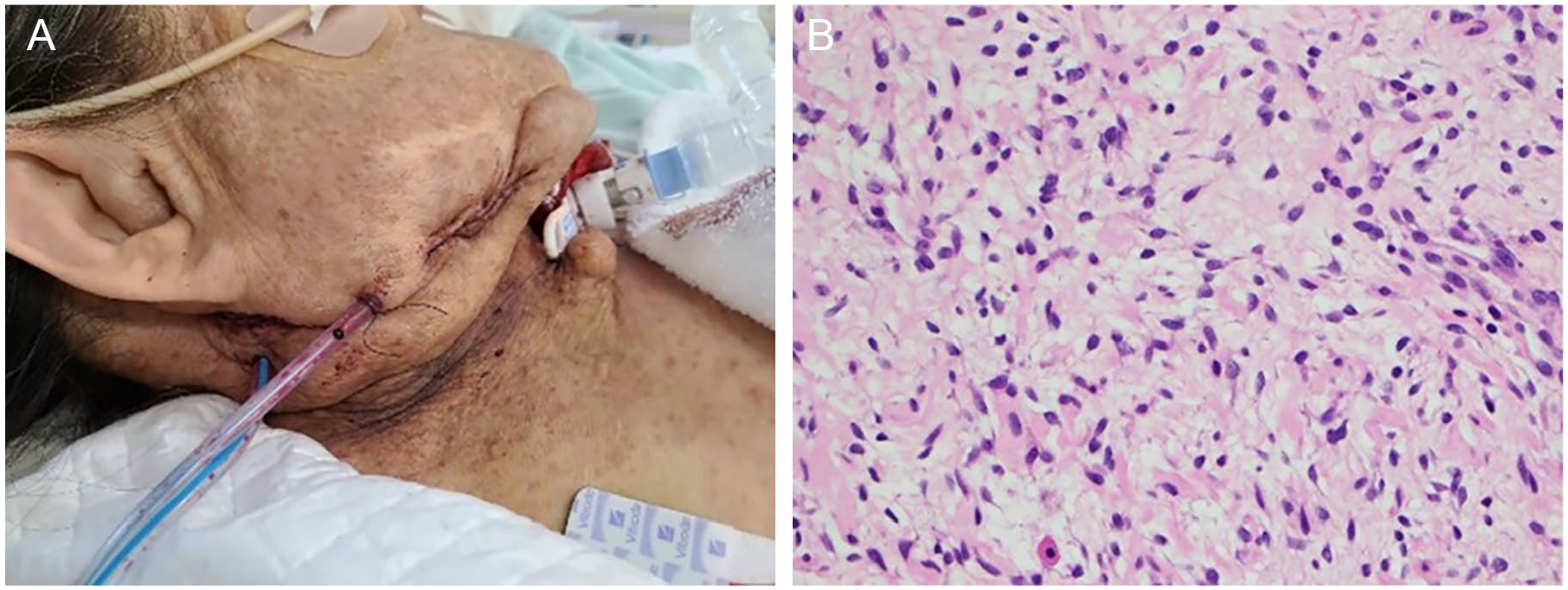
Tracheostomy was performed on the 19th day of hospitalization. The presence of several abnormal blood vessels and fragile tissue was confirmed. Subsequently, drainage tubes were placed in the submandibular and subauricular regions to reduce fluid retention (A). A biopsy of the tumor wall performed concurrently revealed the presence of cells with short spindle-shaped and wavy nuclei proliferated, leading to the diagnosis of neurofibroma (B: hematoxylin and eosin stain, high power view).
Discussion
NF-1, also known as Recklinghausen disease, was first reported in 1882. NF-1 is caused by a mutation of a gene on chromosome 17q11.2, which results in the occurrence of skin pigmentation called café-au-lait spots and cutaneous neurofibromas.1 -3 NF-1 can also affect several other organs, and neurological, endocrinal, gastrointestinal, skeletal, and vascular abnormalities have been described as uncommon complications. 4 Although the incidence of vascular abnormalities is not high, they are the second most common cause of death in patients with NF-1, following malignant peripheral nerve sheath tumors. Vascular complications are caused by direct infiltration of neurofibromas into the vascular media, ischemia of the vessel wall caused by compression of the nutrient artery, and thinning of the vascular media. Notably, repairing the artery and achieving hemostasis becomes difficult once the nutrient artery fails.2,3 The intercostal, subclavian, and internal thoracic arteries are affected most commonly; however, the vessels of the neck, such as the external carotid, vertebral, and subclavian arteries, can also be affected, accounting for approximately 30% of cases. The affected artery in the present case was a branch of the external carotid artery. NF-1 is often complicated by tortuosity and malformation of the artery, which increases the likelihood of bleeding even with mild irritation. It is unknown whether an injury occurred in this case, but the meandering of the vessels and the vascular infiltration of neurofibromas resulted in bleeding while showering.
Treatment options include surgery and vascular embolization. However, vascular embolization is often the first choice of treatment as the control of hemorrhage is challenging due to the increased fragility of the blood vessels, which makes the management of bleeding via ligation or cauterization difficult.3,5 Furthermore, abnormalities of the blood vessels hinder the ability to the anticipate the path of the blood vessels, thereby increasing blood loss. Consequently, the subcutaneous tissue and the anterior cervical muscles were sutured to ensure compression and achieve hemostasis. This approach effectively reduced bleeding from fragile blood vessels.
Sung et al reported that preoperative intravascular embolization simplifies the surgical procedure for neurofibroma, and intravascular embolization is also suitable for the management of recurrent bleeding. 3 In the present case, the preceding vascular embolization resulted in hemostasis to some extent. Therefore, vascular embolization should be the first choice of treatment in cases with hemodynamic stability. However, bleeding recurred after vascular embolization, thereby necessitating additional treatment. Direct embolization of the affected vessel was difficult as it followed a meandering path. External carotid ligation was considered; however, achieving hemostasis was difficult due to the presence of a large amount of fragile tissue.
Drainage tube was placed in this case. Although it was exceedingly effective in preventing rebleeding after vascular embolization, there have been no previous reports of drainage tube placement after vascular embolization. Drainage tubes are often used in head and neck surgery as they aid in the management of micro-bleeding, elimination of dead space, and prevention of infections. The accumulated exudate can dissociate from the flaps, thereby prolonging the period of wound healing and increasing the risk of local infection. As the dead space was enlarged by hematoma removal, drainage tube insertion was effective in the present case. In addition, drainage tube placement after vascular embolization was more effective as it led to the repositioning of the flaps, resulting in the repair of the vascular collapse. Thus, drainage tube placement is more effective in conjunction with vascular embolization. Another major advantage of drainage tube placement is the ease of management, as daily procedures are no longer necessary. In the present case, the drainage tubes were placed in the submandibular and subauricular regions. Since less than 10 mL of effluent was present after 1 week and did not increase thereafter, the drainage tubes were removed after 2 weeks. The maximum amount of effluent was 42 mL from the submandibular region the day after the surgery.
Hematoma removal is advantageous as it can be performed under local anesthesia and does not require unnecessary disruption of the blood vessels, thereby reducing adverse symptoms. However, massive bleeding may occur during the removal of a hematoma, and prompt management is required in such cases. Drainage tube placement after hematoma removal may be an effective option for the management of persistent micro-bleeding after vascular embolization.
Conclusion
Vascular involvement is a complication of NF-1, and it may lead to death due to massive hemorrhage. Vascular embolization is often the first choice of treatment as it helps achieve hemodynamic stability; however, drainage tube placement may be an effective treatment for managing micro-bleeding when rebleeding occurs.
Footnotes
Authors’ Note
Written informed consent was obtained from the patient for the publication of this case report and accompanying images.
Data Availability Statement
The authors confirm that the data supporting the findings of this study are available within the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The requirement of ethical approval was waived by our institution as it is a “Case report” and not a research study.