
Abstract
Introduction
Over the past 2 years, the coronavirus disease 2019 (COVID-19) has undergone continuous mutations, resulting in several variants, including Alpha, Beta, Gamma, Delta, and Omicron. Notably, Omicron exhibits an unusually high number of mutations, with over 30 in its key spike protein. These mutations lead to significant changes in transmissibility, transmission characteristics, and immune escape ability. 1 As of February 2023, the total number of confirmed COVID-19 cases worldwide has exceeded 750 million. Initially, during the early stages of the pandemic, the infection rate among children was less than 2%, significantly lower than that observed in adults. 2 However, since the onset of the Omicron epidemic, there has been a substantial increase in pediatric cases, accounting for 25% of weekly cases between January 27 and February 3, 2022. 3 After the relaxation of China’s zero-COVID policy in November 2022, Omicron not only caused a substantial number of infections in children but also led to changes in the clinical presentation.
Entry of SARS-CoV-2 into host cells necessitates the assistance of transmembrane protease serine 2 (TMPRSS2) or cathepsin L. TMPRSS2 is predominantly located on the cell surface and primarily involved in membrane fusion, exhibiting higher expression levels in the lower respiratory and gastrointestinal tracts compared to the upper respiratory tract. Conversely, cathepsin L plays a role in intracellular endocytosis. 4 Omicron shows limited utilization of TMPRSS2 and instead favors the cathepsin L-mediated endocytosis pathway for host cell entry. Consequently, upper respiratory symptoms become more prominent following Omicron infection, while lung involvement tends to be milder. Cases of sore throat or hoarseness have significantly increased after Omicron infection compared to the Delta variant epidemic. 5 Animal studies have also shown that Omicron-infected lungs exhibit a less inflammatory response. 6 Croup is a common upper respiratory disease characterized by the sudden onset of a barky cough accompanied by stridor (a high-pitched sound during breathing), hoarse voice, and respiratory distress. Clinical observations indicate that children under 5 years old are more susceptible to developing croup after Omicron infection. This susceptibility may be attributed to the fact that Omicron affects the narrower upper respiratory tract of young children, which is more prone to collapse. 7 In this study, we present the clinical features and outcomes of Omicron-associated croup in children during the Omicron surge (December 16 to December 31, 2022) in Shanghai, China.
Patients and Methods
Patients
A total of 105 children with COVID-19 and cough were admitted to the fever clinic and ENT department between December 16, 2022, and December 31, 2022. The median age of these children was 11 months (range: 3-60 months). Prior to admission, some children received a diagnosis of COVID-19 through Rapid Antigen Tests or Polymerase Chain Reaction (PCR) tests, while others performed self-testing at home. However, upon arrival at the hospital, all children underwent PCR retesting, confirming their COVID-19 status. Croup was diagnosed when the patient presented with a barky cough and stridor. The classification of laryngeal obstruction was as follows: (a) I° (mild): no symptoms at rest, but slight inspiratory dyspnea and stridor may occur during crying or exertion; (b) II° (moderate): slight inspiratory dyspnea during quiet respiration, exaggeration on exertion, sleeping, and eating is nearly normal, with no evidence of hypoxia; (c) III° (severe): marked inspiratory dyspnea, loud stridor, depression of suprasternal and supraclavicular fossae and intercostal spaces, cyanosis, restlessness, and struggles for air hunger, accompanied by rapid pulse, high blood pressure, and refusal to eat; and (d) IV° (extremely severe): extremely dyspneic, restless, sweating, and cyanotic. Pulse is rapid, irregular, weak, and thready. Blood pressure drops. Ultimately, circulatory collapse may occur, leading to asphyxia or cardiac failure. This study was approved by the ethics committee of the Children’s Hospital of Fudan University.
Data Collection and Follow-Up
The clinical characteristics, symptoms, laboratory results, chest X-ray or laryngoscope findings, treatments, and outcomes of children with COVID-19 and croup were reviewed. All children were followed up for 8 months by telephone.
Results
General Information and Clinical Symptoms
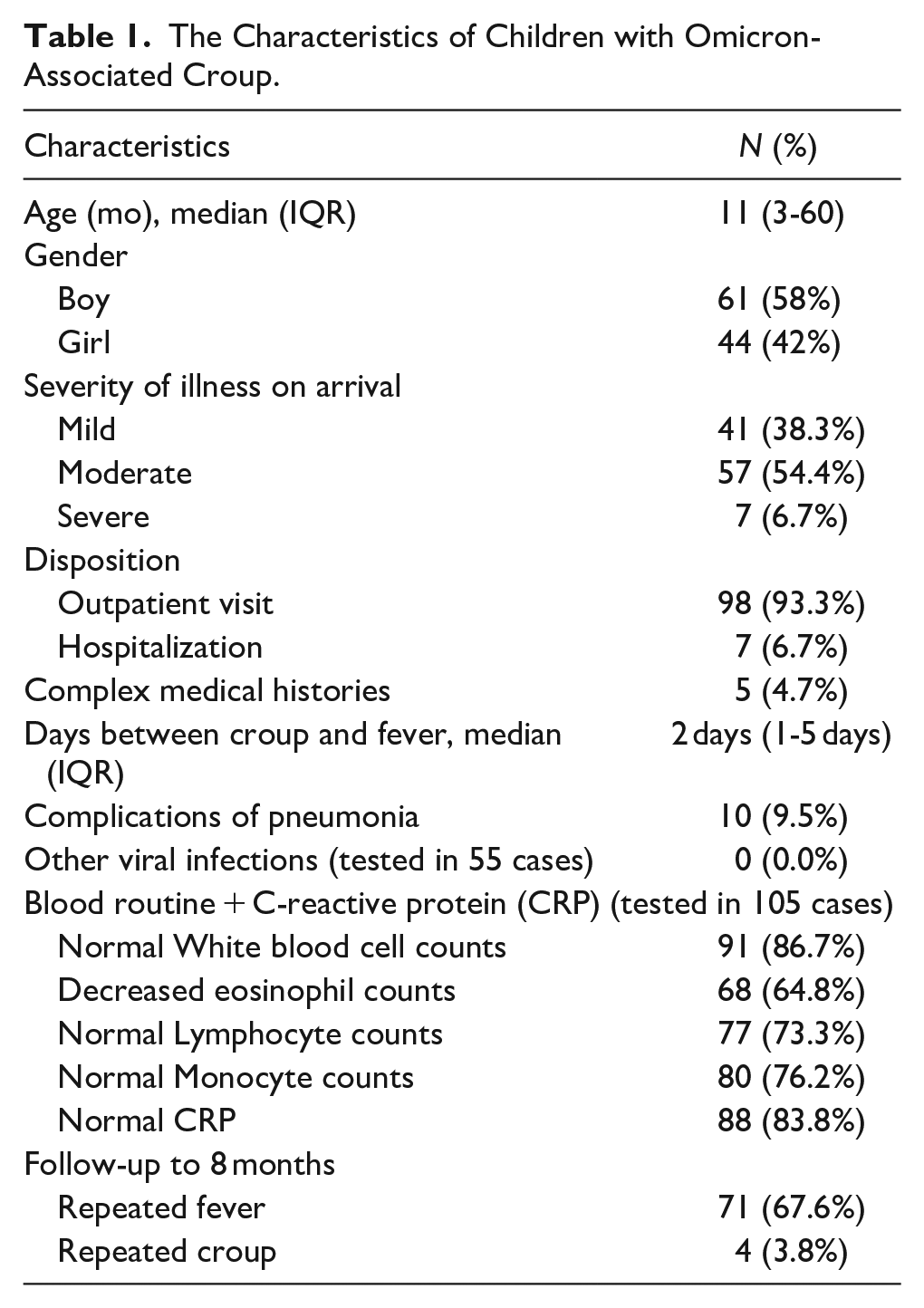
As shown in Table 1, a total of 105 children with COVID-19 and croup were included in this study. The median age of the children was 11 months (range: 3-60 months), with 61 boys and 44 girls. The severity of croup was assessed using the classification of laryngeal obstruction: 41 cases (38.3%) were classified as mild, 57 cases (54.4%) as moderate, and 7 cases (6.7%) as severe, indicating that the majority of cases were not severe. Among the cases with complex medical histories, 5 had underlying conditions, including 2 cases of immune deficiency, 1 case of hydrocephalus, 1 case of bronchostenosis, and 1 case of heart disease. All 5 of these cases had moderate laryngeal obstruction. Most children with croup presented with fever, barky cough, and stridor, along with other upper respiratory symptoms such as rhinorrhea, sputum accumulation, and nasal stuffiness. Croup typically developed 1 to 5 days (median 2 days) after the onset of fever, rather than on the first day.
The Characteristics of Children with Omicron-Associated Croup.
X-Ray of the Chest and Laboratory Results
A total of 51 cases underwent chest X-rays, and only 10 children were diagnosed with pneumonia, indicating that the majority of COVID-19 children with croup did not have complications of pneumonia. Among the 55 cases that had respiratory virus antibody tests (anti-chlamydia pneumoniae, anti-respiratory syncytial virus, anti-adenovirus, anti-coxsackie virus, and mycoplasma pneumoniae), all of them tested negative. Additionally, blood routine + C-reactive protein (CRP) examinations were conducted on 105 cases in the early stage of the disease. White Blood cell (WBC) counts were found to be normal in 91 cases (86.7%). Eosinophil counts were severely reduced in 68 cases (64.8%). Lymphocyte counts were reduced in 28 cases (26.7%). Monocyte counts were increased in 25 cases (23.8%). CRP levels were increased in 17 cases (16.2%). Out of the 11 cases that had serum amyloid A tests, 8 showed increased levels (72.7%).
In summary, the majority of COVID-19 children with croup did not have complications of pneumonia. Most of these children exhibited decreased eosinophil counts and increased serum amyloid A levels. Moreover, other blood routine indicators were mostly within the normal range.
Treatments and Outcomes
Among the cases included in our study, 7 were admitted to the emergency ward due to Grade III laryngeal obstruction. These cases received treatment with prednisone/dimethylamine + atomization + oxygen inhalation, but none required endotracheal intubation. Sixty cases (60/105, 57.1%) were treated with atomization for 3 to 7 days, while the remaining 38 cases received methylprednisone/dexamethasone/oral prednisone + atomization. Seven cases (7/105, 6.7%) were admitted to the hospital due to severe laryngeal obstruction, while the rest of the cases were treated in the outpatient clinic. All of the cases recovered from croup.
During the 8 months of follow-up, 2 cases developed granulocytopenia; however, they eventually recovered. Seventy-one cases experienced repeated fever due to various infections, such as repeated SARS-CoV-2, respiratory syncytial virus, mycoplasma pneumoniae, A/H1N1 influenza, and others. However, only 4 cases (4/105, 3.8%) had repeated croup. In summary, the outcomes for the 105 cases were good.
Discussion
Pediatric acute croup is an acute inflammation of the larynx’s mucosa, commonly seen in various viral infections. In approximately 80% of cases, one or more viruses are detected. The most common virus is parainfluenza virus, particularly parainfluenza virus type 1, accounting for around 25% to 33% of all croup cases. Parainfluenza virus type 3 is the second most common, accounting for about 6% to 10%. Other viruses also have a correlation with croup in children. For example, influenza viruses account for 1% to 10% of children with croup, depending on the year and circulating strain. Additionally, rhinoviruses, enteroviruses, adenoviruses, and bocavirus are detected in approximately 9% to 13% of children with croup. Moreover, the NL63 strain of human coronavirus (hCoV) has a propensity to cause croup and has been recognized as the second most commonly isolated virus among children with croup in Seoul, South Korea. 8 Bacterial croup is less common and may be caused by mycoplasma pneumoniae and Corynebacterium diphtheriae. However, the type of infectious agent does not affect outcomes or initial management. 9
While it has been believed that SARS-CoV-2 infection rarely causes croup, recent studies have observed a spike in pediatric croup during the Omicron epidemic. Based on this fact, it can be inferred that Omicron is more susceptible to upper respiratory tract infections.10-14 For instance, a Korean study in 2019 revealed that 12.4% (21/569) of children with COVID-19 developed croup during the Omicron epidemic, compared to 1.2% during the Delta epidemic. 15 Similarly, a Japanese case report in 2022 reported an increase in croup cases during the Omicron epidemic. 16 A study conducted at Seattle Children’s Hospital in the USA observed a higher prevalence of SARS-CoV-2 in children with croup during the Omicron period (48.0% of 107 children with croup) compared to the Delta period (2.8% of 407 children with croup). 17 Consistent with this, another study conducted at Children’s Healthcare of Atlanta in the USA also demonstrated that during a 2-month Delta period and a 3-week Omicron period, 20 (0.9%) of 2115 COVID-19 visits and 222 (12.0%) of 1851 COVID-19 visits were diagnosed as croup, respectively. 18 These findings suggest that Omicron infection is a risk factor for croup, which aligns with our own findings.
However, in our study, no children with croup older than 6 years were found. It is generally believed that croup predominantly affects children aged 6 months to 3 years. However, a study conducted in New York in 2023 with a total of 57 children diagnosed with croup during the Omicron epidemic found that 12 (19.0%) were older than 6 years. Most of these children had been vaccinated and had never experienced croup before. Fortunately, the condition of these children older than 6 years was not serious. 19 Based on these findings, it can be inferred that older children infected with the Omicron variant may also develop symptoms of croup, and a lack of awareness among healthcare practitioners could lead to missed or delayed diagnoses.
Another interesting finding is that Omicron-associated croup rarely coexists with other viral infections. In our study, a total of 55 cases underwent respiratory virus antibody tests (anti-chlamydia pneumoniae, anti-respiratory syncytial virus, anti-adenovirus, anti-coxsackie virus, and mycoplasma pneumoniae), and all of them tested negative. This phenomenon was also observed in Jessica Hayes’ study, 20 which included 76 children with Omicron-associated croup. Among the 24 patients who had a full respiratory pathogen panel obtained in addition to COVID-19 PCR testing, only 3 patients tested positive for one or more additional viruses (human metapneumovirus, rhinovirus/enterovirus, and coronavirus 229E). None of the children with coinfections required hospitalization. Similarly, Brewster RC’s study 7 found that out of 75 children tested for other viral infections, all were negative except for 1 with rhinovirus. These 3 studies suggest that there is no need for further testing of other viruses in Omicron-associated croup, which helps to reduce healthcare expenses.
These children had few abnormal results in their early-stage blood routine examinations, with normal levels of WBC and CRP. However, most of them had reduced eosinophil counts. A previous study has suggested that these features might indicate an early sign of COVID-19. 21 Eosinophils are derived from pluripotent hematopoietic stem cells in the bone marrow. They play a role in secreting cytokines, releasing toxic proteins (ECP, EPO, and EDN), producing oxygen free radicals (superoxide anion), and mediating inflammatory diseases, allergic diseases, and parasitic infections. Massive infiltration of eosinophils in tumor tissues could improve the patient’s prognosis. 22 Studies have found that eosinophils were significantly reduced in some patients after experiencing acute infectious diseases, major surgery, and burns. Most severe acute respiratory syndrome patients had a similar result, possibly due to increased secretion of adrenal cortex hormones in the stress state.23,24 However, the condition would return to normal later.
Secondly, we observed that lymphopenia and monocytopenia were infrequent and affected about 20% of children. A prior study has reported that these abnormalities can occur during COVID-19. Nevertheless, our study did not observe them, perhaps because most children were not severely ill, and few had complications such as pneumonia, allowing for quick recovery.
A USA study of 79,592 children under 5 years of age with first-time COVID-19 infection found that children infected with the Omicron variant had a 29.0% reduction in emergency room visits, a 67.0% reduction in hospitalizations, a 68.0% reduction in ICU occupancy, and a 71.0% reduction in mechanical ventilation compared to the Delta. 25 This suggests that the Omicron variant is less toxic. A similar phenomenon was observed in our study, where only 10 children (9.5%) developed pneumonia, which co-occurred with or followed croup. Moreover, out of the 105 cases in our study, 41 (38.3%), 57 (54.4%), and 7 (6.7%) were diagnosed with mild, moderate, and severe laryngeal obstruction, respectively. Two other studies also reported similar findings. In Lim CC’s study, 26 59 (72.8%), 13 (16.0%), and 9 (11.0%) had mild, moderate, and severe laryngeal obstruction, respectively. Choi YY’s study found that 5 (23.8%), 14 (66.7%), and 2 (9.5%) had mild, moderate, and severe laryngeal obstruction, respectively. In summary, the toxicity of the Omicron variant was reduced, and most cases of Omicron-associated croup 15 presented with mild to moderate laryngeal obstruction.
However, compared to croup associated with infections caused by other viruses, most studies suggest that Omicron-associated croup is more severe. This conclusion is mainly based on reported hospitalization rates. For example, in Hayes J’s study, 20 19 children (23.5%) required hospitalization, with 3 of them having complex medical histories and being admitted to the ICU. A study conducted in South Korea 15 found that 23% of children with Omicron-associated croup were hospitalized. Lim CC 26 reported a case of COVID-19-induced croup in an 18-month-old child that progressed into multisystem inflammatory syndrome. Venn AMR 10 observed 3 cases of COVID-19-associated croup (11 months, 2 years, and 9 years old) presenting significant pathology and delayed resolution of their stridor at rest (12, 19, and 21 hours, respectively). Brewster RC’s study 7 identified 75 children diagnosed with COVID-19-associated croup, and the hospitalization rate (11.5%, 7/61) and redosing of croup-directed therapies may indicate a more severe phenotype compared to other viral causes. However, for croup associated with other viral infections, previous studies have reported that approximately 85% of cases are classified as mild, less than 1% meet criteria for severe croup, less than 5% of all croup cases are hospitalized, and only 1% to 3% require intubation. 9 In summary, current studies suggest that Omicron-associated croup is more severe compared to croup associated with other viral infections. However, whether Omicron-associated croup requires such a high hospitalization rate (about 20%) is disputed.
In our study, the hospitalization rate was only 6.7%, and only cases with Grade III obstruction were admitted to the hospital. The low hospitalization rate can be attributed to 2 reasons: (a) during the Omicron outbreak, there was a large number of patients and limited medical resources in Shanghai, so only severe cases could be admitted to the hospital ward and (b) the enrolled cases in our study were generally healthy without underlying diseases, and only 5 cases had complex medical histories. These cases received nebulization therapy and/or intravenous steroid treatment in the early stages of their illness, resulting in relief of laryngeal obstruction symptoms, and none of the cases required intubation. A follow-up period of up to 8 months was conducted for these cases, and no residual effects were found. Two cases showed a temporary decrease in granulocyte count after infection, but by the 8-month follow-up, their counts had returned to normal. Out of the 71 cases that had repeated fever due to various infections, only 4 of them had repeated croup. Hayes J’s study 20 also noted that among the hospitalized cases, only 50% required further interventions such as epinephrine solution, dexamethasone, or closer monitoring, such as long-term steroid use and/or remdesivir for patients requiring continuous oxygen supplementation. Therefore, the authors considered that 50% of the hospitalizations were unnecessary. Re-gardless of the reasons for the low hospitalization rate, our study suggests that even though Omicron-associated croup leads to more severe symptoms compared to croup associated with other viruses, the majority of cases still experience mild to moderate symptoms. If children do not have severe laryngeal obstruction, unnecessary hospitalization can be avoided, and outpatient treatment can be pursued to reduce healthcare expenses.
Conclusions
In conclusion, young children should be vigilant for croup during the Omicron epidemic. Routine blood tests may reveal reduced eosinophil counts, while WBC and CRP levels remain normal in the early stages. Omicron-associated croup rarely coexists with other viral infections. Most cases present with mild to moderate laryngeal obstruction, and a small number are complicated by pneumonia. Prompt nebulization therapy and/or intravenous steroid treatment have shown favorable outcomes. Although Omicron-associated croup can be more severe than croup associated with other viral infections, unnecessary hospitalizations could be avoided, thereby reducing healthcare expenses.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.