
Abstract
Fibromatosis or desmoid tumors are rare benign fibroblastic lesions that are rarely present in the head and neck regions. When they do occur in these regions, however, they tend to be aggressive toward the surrounding tissue and be associated with heavy morbidity and mortality. We report the case of a 26-year-old Tunisian female who presented with acute obstructive dyspnea and a 3-week history of cervical swelling. The swelling was initially only located in the left submandibular area, it then gradually extended to all the anterior cervical supra- and infrahyoid regions causing a clinical presentation resembling that of obstructive dyspnea, the patient was admitted, and an emergency tracheotomy was performed. Tissue samples were taken, pathological analysis revealed an aggressive case of fibromatosis. The patient was treated with corticosteroids and antihormonal therapy, the fibrous mass shrunk considerably allowing the removal of the tracheotomy cannula, no tumor recurrence was noted during the observation period. Due to the rarity of this disease, especially in the cervical region, there are no therapeutic guidelines available.
Introduction
Desmoid tumors (DT), or fibromatosis, are a form of fibrous proliferation that tends to be locally invasive. It is a rare and benign tumor accounting for almost 0.03% of all neoplasms. 1 Its pathogenesis is still unclear; however, it is considered a multifactorial disease. 2 The risk of fibromatosis onset and growth has been linked to trauma, history of surgery, pregnancy, and the use of oral contraceptives. 3
DT can develop anywhere in the body. The head and neck locations represent 10%-15% of cases. 3 Management of the aggressive form of the disease in this region is particularly challenging, due to its complex anatomy and close association with vital neurovascular structures. This article presents the second recorded case of aggressive cervical fibromatosis causing airway obstruction in English Medical literature.
Case Presentation
A 26-year-old otherwise healthy Tunisian woman was referred to our department with a 3-week history of cervical swelling.
She had a medical history of well-controlled asthma and a tonsillectomy in early childhood done for recurring tonsillitis. There was no history of facial trauma or dental care.
The swelling started in the left submandibular area for which the patient was prescribed an ambulatory antibiotic by her family doctor, no improvement was noted.
On physical examination, there was a firm mass in the left submandibular region and swelling in the mouth floor along with dental cavities in the left first molar, there was no associated lymphadenopathy, with no other notable abnormalities.
The patient was admitted to our department. Initial cervical computed tomography showed swelling and infiltration of the left submandibular area. Diagnosis of dental-origin cellulitis was initially retained, and the patient received an antibiotic treatment. However, the swelling gradually increased in size extending to all the anterior cervical supra- and infrahyoid regions causing obstructive dyspnea (Figure 1).

(a) Clinical view of an extensive cervical mass; (b) intraoperative view during tracheotomy.
An emergency tracheotomy was performed under general anesthesia and a tissue biopsy was taken at the same time (Figure 1).
Pathological analysis of the biopsy specimen showed a soft tissue tumor with variable cellularity made up of spindled cells with myofibroblast morphology embedded between striated muscle fibers (Figure 3). Im-munohistochemical (IHC) staining showed positive im-munostaining for Acute Myeloid Leukemia (AML) and beta-catenin, and was negative for desmin (Figure 2) which is compatible with fibromatosis.
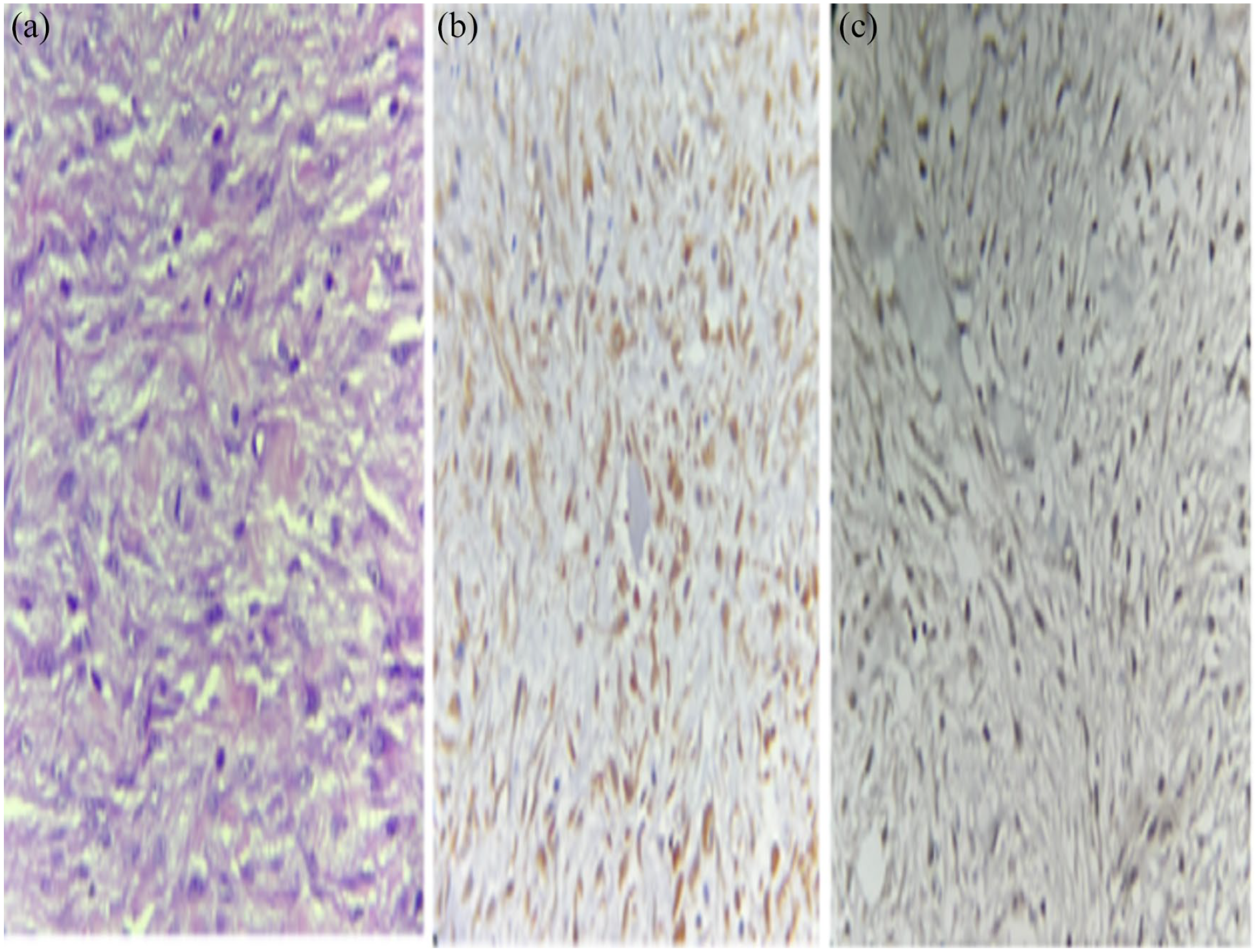
Histopathology: soft tissue tumor composed of variable cellularity made of spindled cells with myofibroblast morphology that dissociates the striated muscle fibers (a). Immunohistochemical staining shows positive immunostaining for B-catenin (b) and AML (c).
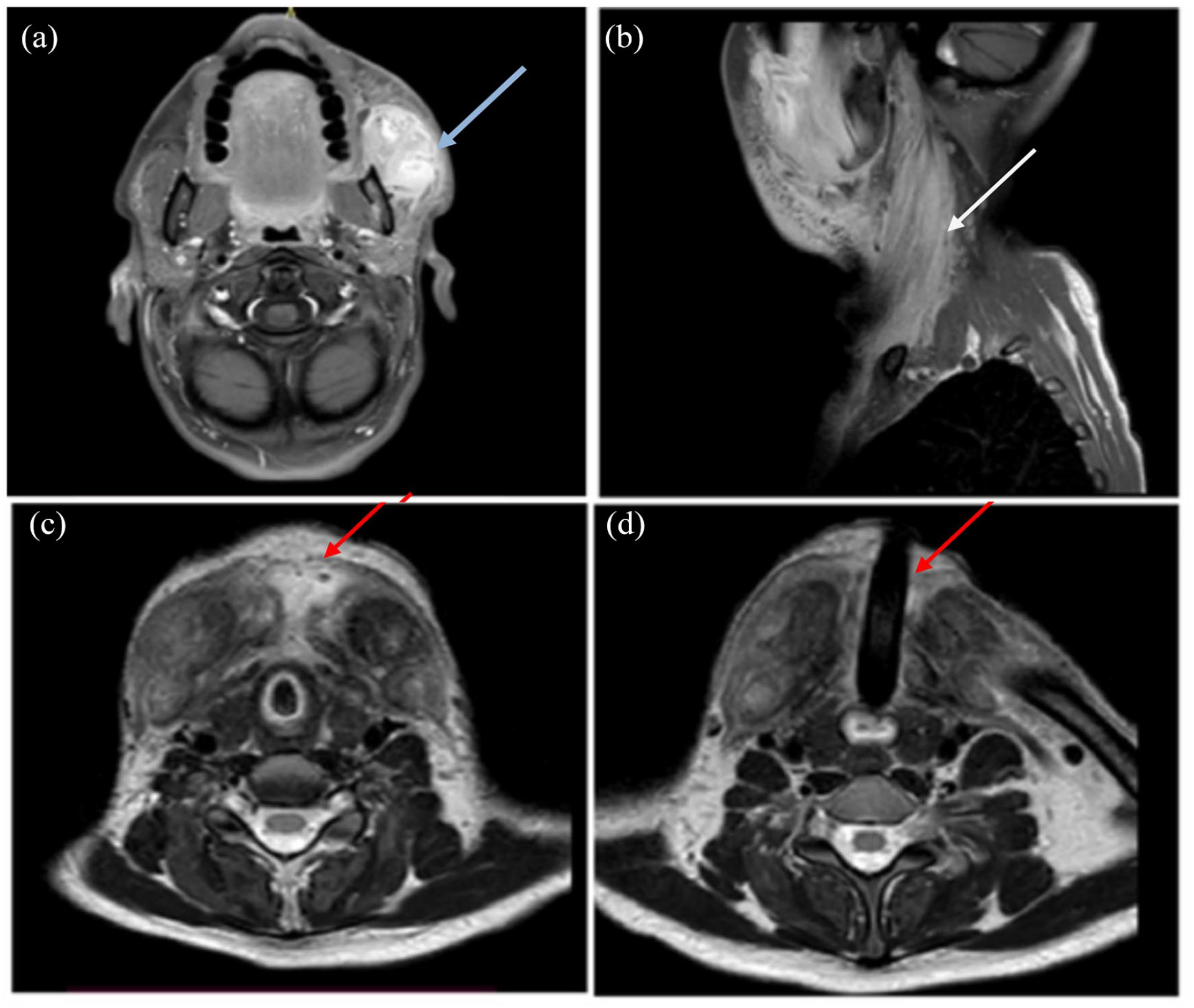
Axial and sagittal T1 post-contrast magnetic images of the neck (a and b): heterogeneous contrast-enhancing mass, hypointense on T1 and hyperintense on T2, affecting Sternocleidomastoid muscles (white arrow), suprahyoid muscles, and left masseter muscle (blue arrow). Axial T2-weighted turbo spin-echo (T2 TSE) magnetic resonance imaging showing inflammatory tissue process invading neck muscles and soft subcutaneous tissue without and with a tracheostomy tube in situ (c and d) (red arrow).
A body scan was conducted, no extra cervical lesions were found.
Cervical magnetic resonance imaging (MRI) showed a large heterogeneous contrasted mass, hypointense in T1 sequences and hyperintense in T2 sequences, affecting the Sternocleidomastoid muscles, suprahyoid muscles, and the left masseter muscle (Figure 3).
Due to the extensive local expansion of the tumor, we sought to avoid surgical excision as it came with significant risks. After promptly informing the patient, we opted for medical treatment: prednisone 60 mg/day for 10 days associated with antihormonal treatment (tamoxifen) for 4 months. By the 4 months mark the fibrous mass had shrunk considerably and the tracheotomy cannula was removed (Figure 4). No tumor recurrence was noted after 12 months of follow-up.

Posttreatment view of the patient after 12 months of follow-up.
Discussion
Fibromatosis is a rare disease; it represents less than 0.03% of all tumors, with an incidence of 4 new cases per 100,000 people per year. 1 It is categorized under soft tissue tumors, thought to arise from connective tissue, facial sheaths, and other mesenchymal structures of the body. 4 They can occur at any age, in both sexes, but especially in young women aged between 20 and 40 years. 4 It clinically presents as a progressively developing deep-seated, fixed, painless mass. Depending on its location, it may be associated with trismus, dysphagia, and proptosis. Upper airway obstruction can occur, as was reported in our case. It is a potentially fatal clinical presentation that requires urgent medical attention.
Computer tomography scan and especially MRI are the imaging techniques of choice. They provide important information on the extension and the degree of invasiveness of the tumor which is crucial in treatment planning especially in sensitive areas such as the head and neck. 3
Pathological examination confirms the diagnosis and can distinguish between the various forms of the disease, it also excludes differential diagnoses (such as a desmoplastic fibroma or neurofibroma). 5
The tumor is typically composed of mature fibroblasts arranged in spindle form with a tendency to clump in scattered foci with variable cellularity. 3
In IHC staining, tumor cells were reported to be negative for S-100 and CD 34 and frequently positive for desmin, vimentin, and B-catenin. 6
The main treatment modality for fibromatosis is complete surgical resection with wide margins, 5 but this may not be easily achieved in sensitive and compact areas such as the head and neck and can prove to be mutilating with potential functional and cosmetic damage, 1 as is the case of our patient.
Fibromatosis is histologically benign but locally ag-gressive and has a high recurrence rate (20%-70%). 7
Recurrence is more commonly reported in the first year, but there are reports of lesion recurrence even 5 years after treatment. 7 In cases such as ours, nonsurgical treatments such as radiation therapy, chemotherapy, hormonal therapy, and nonsteroidal anti-inflammatory drugs (NSAIDs) have been used to treat DT to maintain vital organ function and avoid mutilation. 1
Radiotherapy has been proposed as a second option for patients who cannot undergo surgery or an as adjunct treatment for the latter. Studies have shown that post-operative radiation therapy can reduce relapse rate from 59% to 25%. 8 However, radiation therapy carries radiation side effect risk and even risks of secondary neoplasm development, and resort to this therapeutic modality should therefore be carefully decided on a case-by-case basis. 8 In cases where radiation therapy and surgery are risky, administration of NSAIDs (like celecoxib or indomethacin) and antiestrogen treatment (tamoxifen or toremifene) can prove to be a viable alternative and be an effective therapeutic modality with low toxicity. 3 Another study, 9 has shown that antiestrogen and anthracycline-containing regimens were associated with a higher radiological response rate against DT. In the case of asymptomatic desmoids tumor with no signs of progression; experts recommend the wait-and-see strategy. 10
In a study that included 83 patients placed under active surveillance, progression-free survival at 5 years was 50% and the median progression time was 14 months. 10
Finally, Management of DT should be multidisciplinary, due to the diversity of clinical presentations and therapeutic options.
Conclusions
Desmoid fibromatosis is a rare and benign soft tissue tumor. the head and neck presentations of this disease are particularly difficult to manage due to proximity to vital structures. There are currently no guidelines available on treatment modality. This study, despite its very limited patient count, may provide an overview of the different treatment modalities and an example of successful management of this rare entity.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent for the publication of data and images was obtained from the patient. Data availability statements and all data generated or analyzed during this study are included in this article. Further inquiries can be directed to the corresponding author.