
Abstract

Samuel Gross was a renowned surgeon of the 19th century. Born on a farm in Easton, PA in 1805, he graduated from the Jefferson Medical College in 1828.
1
He had academic appointments at Cincinnati and Louisville before returning to Jefferson to serve as the Chairman of Surgery.
1
Throughout his medical career, he was a prolific writer, penning multiple influential works including the two-volume “System of Surgery,”
2
one of the earliest, comprehensive overviews on surgery. While covering all surgeries (including orthopedics, ophthalmology, and urology), this textbook included a fine section on the removal of aerodigestive tract foreign bodies of all kinds. Much of this chapter was based on his earlier work, “A Practical Treatise on Foreign Bodies in the Air-Passages,”
3
detailing the clinical course and management of over 200 cases of foreign body aspiration. In it, Gross muses: How many persons have perished, perhaps in an instant, and in the midst of a hearty laugh, the recital of an amusing anecdote, or the utterance of a funny joke, from the interception at the glottis of a piece of meat, a crumb of bread, a morsel of cheese, or a bit of potato, without a suspicion, on the part of those around, of the real nature of the case!
Gross categorizes airway foreign bodies to include those of vegetables (seeds, corn, and nuts), animals (bits of meat or bone), and mineral matter (pebbles, nails, and coins) (Figure 1). He points out that foreign body aspiration may cause morbid suffocation from enlodgement within the glottis. In other cases, the foreign body can remain in the trachea or lodged in either bronchus, causing local irritation, inflammation, ulceration, and later pneumonia or abscess formation. He noted that once the body entered the airway, “instantly, the most violent distress is excited,” followed by “frequent paroxysms of coughing.” Other symptoms included dysphonia, ranging from a “croup, or hoarse, and low” quality to a voice that is “reduced to a mere whisper. Hematemesis, noisy breathing, sound[s] of a stone shaken violently in an earthen jar.” Expectoration, dyspnea, and pain were also expected as normal sequelae.

Foreign bodies removed from the airway by Samuel Gross. 4
The nature of these symptoms, coupled with physical exam findings, can localize the foreign body within the airway. Gross had described that if situated in the larynx, the foreign body would cause some degree of hoarseness or even aphonia, coupled with discomfort in the region of the larynx. If impacted in one of the bronchi, the “respiratory murmur. . .may be very diminished, or wholly absent, according to the amount of the pulmonary obstruction.” If within the trachea itself, the patient experiences a “peculiar sensation which the substance produces as it passes up and down the windpipe.” That is not to say that the foreign body cannot move in position once it enters the airway. Gross notes that “the extraneous substance may change its place in consequence of the impulse which it receives during coughing, during violent expulsive efforts of the lungs, or even during the various movements of the body.”
Early medical management focused on aiding in the natural expulsion of the foreign body by use of emetics, sternutatories (causing sneezing), and expectorants. Gross notes that “the expectations thus raised have never been realized,” alluding to the lack of consistent efficacy of these medications. Also, Gross notes the dangers of these medications as the violent coughing, vomiting, sneezing, and expulsive efforts of the lungs may in fact cause the foreign body to be lodged in the glottic inlet and cause suffocation. Gross briefly touches upon the inversion of a patient as a means to expel a foreign body, although with similar criticism for the risk of displacing the foreign body into the glottis and leading to suffocation.
The first practical bronchoscopes were not developed until the 1890s by Kirstein, Killian, and Jackson, 3 so for Gross, foreign body removal was truly surgical. A “bronchotomy,” as Gross called any artificial opening into the airway, set the stage for definitive management of airway foreign bodies. As Gross stated, “the only real safety of a person, laboring under a foreign body in the air-passages, consists in bronchotomy.” Gross described three approaches to the airway: laryngotomy, division at the cricothyroid membrane, tracheotomy (Figure 2), division of the trachea at a point between the cricoid and sternum, usually incising through multiple tracheal rings, and laryngo-tracheotomy when a laryngotomy is initially performed and then the incision is extended to the trachea if the initial laryngotomy did not suffice. Each was advised depending on the location of the foreign body, with spontaneous removal thereafter or manual extraction with the choice of the instrument by the treating physician (Figures 3 and 4). 4
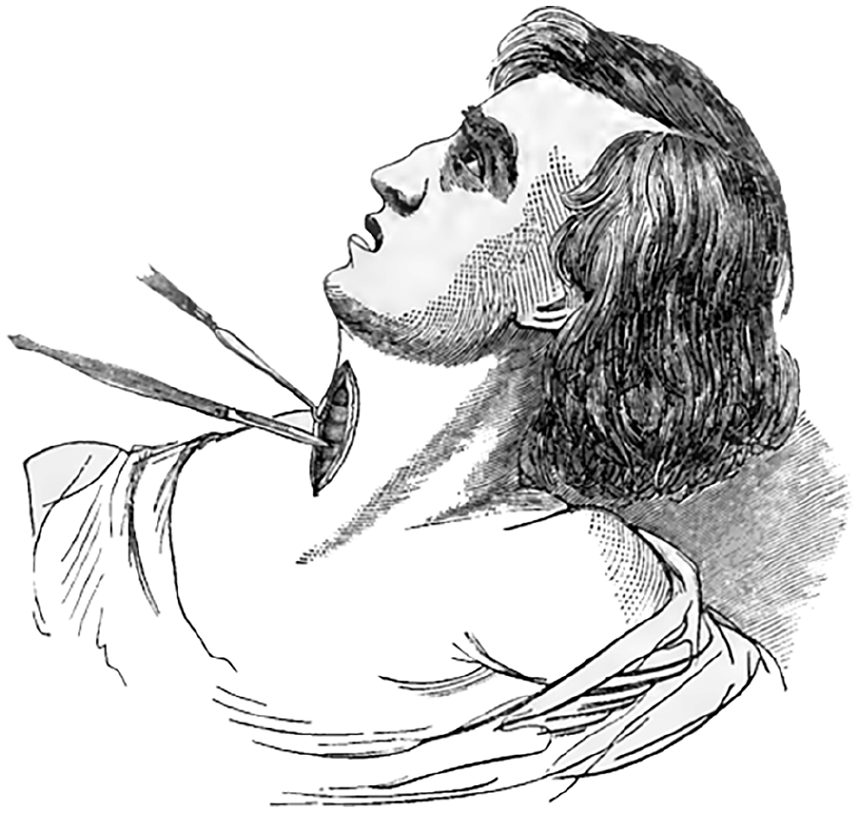
Tracheotomy. 3

Grasping forceps used by Samuel Gross. 3

Extraction instruments circa 1872. 4
Footnotes
Data Availability Statement
Note applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical/Consent Statement
Informed consent was not required.
Grant Number
Not applicable.