
Abstract
Introduction
Branchial cleft deformities are the second most common congenital lesions of the head and neck in children, accounting for approximately 30% of congenital neck diseases.1,2 These deformities can manifest as sinus tracts, fistulas, cysts, or cartilaginous remnants. The currently accepted theory is that branchial cleft deformities are caused by incomplete occlusion of the branchial sac and branchial cleft during embryonic development. During the 6th week of embryo development, the second arch envelopes the third and fourth arches, subsequently uniting with the inferior precardiac mass, leading to the appearance of the cervical sinus, replacing the second to fourth grooves. Concurrently, the parathyroid glands and thymus are derived from the third to fifth pouches. Normally, the cervical sinus is completely resorbed at birth. The branchial fistula is in fact persistence of the exterior opening of the cervical sinus. 3 The second branchial cleft fistula is the most common, accounting for about 95% of all branchial cleft fistulas. In 1928, Bailey described 4 types of branchial cysts based on their relations to their surrounding structures. 4 According to his classification criteria, the second branchial cleft sinuses are classified into 4 types: the blind end of the fistula of type I is as deep as the sternocleidomastoid muscle fascia; type II reaches the surface of the carotid artery; type III passes between the internal and external carotid and extents to the lateral wall of the pharynx; and type IV, also known as complete branchial fistula, opens in the tonsillar Fossa.
This article retrospectively analyzes 76 cases of second branchial fistula, to provide the experience of diagnosis and treatment.
Materials and Methods
Study Design and Patients
In this retrospective study, we enrolled children with second branchial cleft fistulas who underwent surgical treatment at our department from January 2016 to December 2020. All patients underwent cervical ultrasonography before the operation, and the branchial cleft fistula was confirmed by postoperative pathological examination. All cases were initial cases. This study was approved by the medical ethics committee of Beijing Children’s Hospital.
Surgical Technique
All patients underwent cervical ultrasonography. In 8 cases, magnetic resonance imaging (MRI) was performed further to visualize the fistulas. These imaging results were used for the selection of the surgical incision. All patients underwent surgery under general anesthesia with tracheal intubation. Those with external orifices were injected with methylene blue to trace the tract before operation. Methylene blue staining was observed in the tonsillar fossa in 4 cases during the operation, and type IV branchial cleft fistulas were subsequently diagnosed. For type I cases, a small fusiform incision of approximately 5 mm in length was made along the periphery of the fistula, and the fistula was dissected until its bottom for resection. For type II cases, a fusiform incision of approximately 1 cm in length was made along the fistula, and the fistula was dissected to the root for complete excision.
For patients diagnosed with type III branchial cleft fistula on preoperative ultrasonography, a trapezoidal incision was made in 2 cases, and a fusiform incision of approximately 2.5 cm in length was made around the fistula. After dissection, the fistula was separated upward along its periphery, and another transverse incision was made at the level of the hyoid bone, about 1.5 cm in length. The fistula was then pulled out from the upper incision, separated upward until it reached the constrictor muscle of the pharynx, and cut off after ligating. In 2 cases, a single horizontal incision was made, about 3.5 cm in length. The fistula was dissected deep into the submandibular gland and resected after ligation.
In 4 cases of type III and 4 cases of type IV branchial fistula, a single incision, about 2 cm in length (Figure 1) was made for subsequent dissection of the fistulas under endoscopic assistance. The fistula was separated to the deep side of the submandibular gland, and endoscopes were applied to expose the operative cavity. A circular cavity was formed around the fistula, and fistulas were subsequently found to cross the hypoglossal nerve and glossopharyngeal nerve (Figure 2) and to be ligated at the pharyngeal constrictor level. It is difficult to ligate the fistula through the small incision. Therefore, we used right-angle pliers to hold the end of the fistula, subsequently applying a loose knot over the pliers. A thread pusher was then used to push the knot to the upper end of the fistula, and the knot was tightened (Figure 3). This method is simple to conduct and can greatly reduce the operative time.

The single small incision is about 2 cm in length.
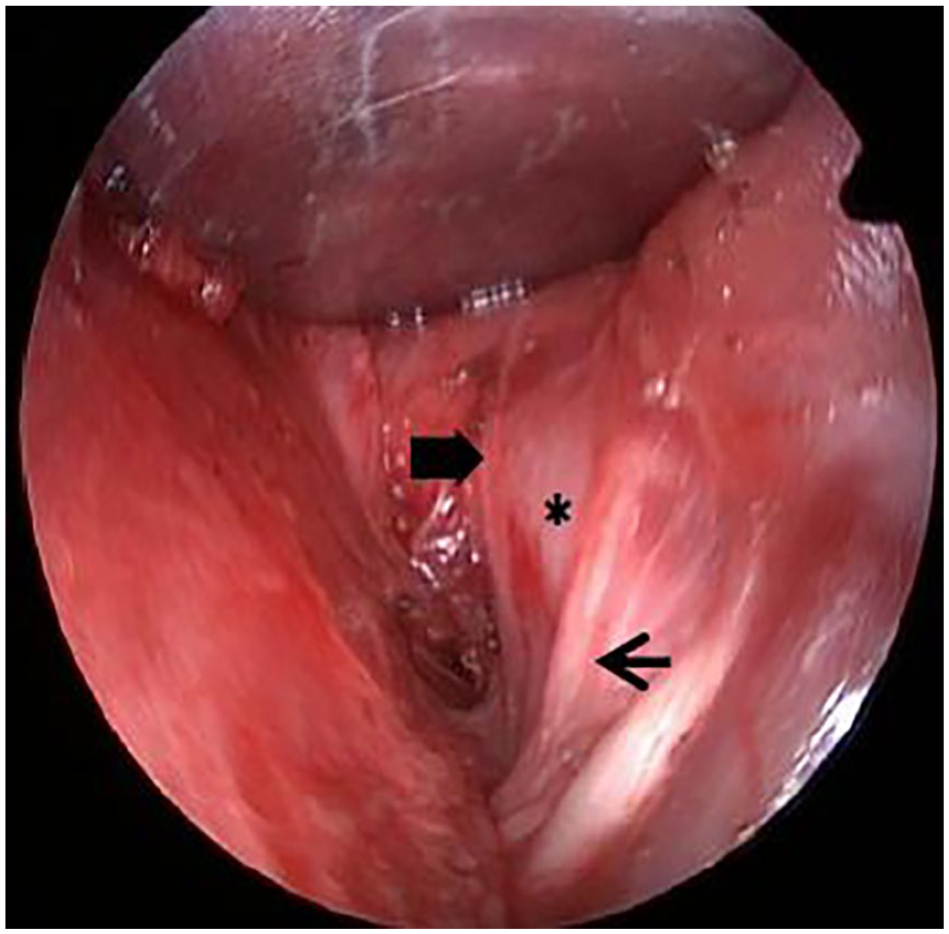
The hypoglossal nerve (the thin arrow), glossopharyngeal nerve (the thick arrow), and carotid artery (the asterisk) are located deep within the fistula.
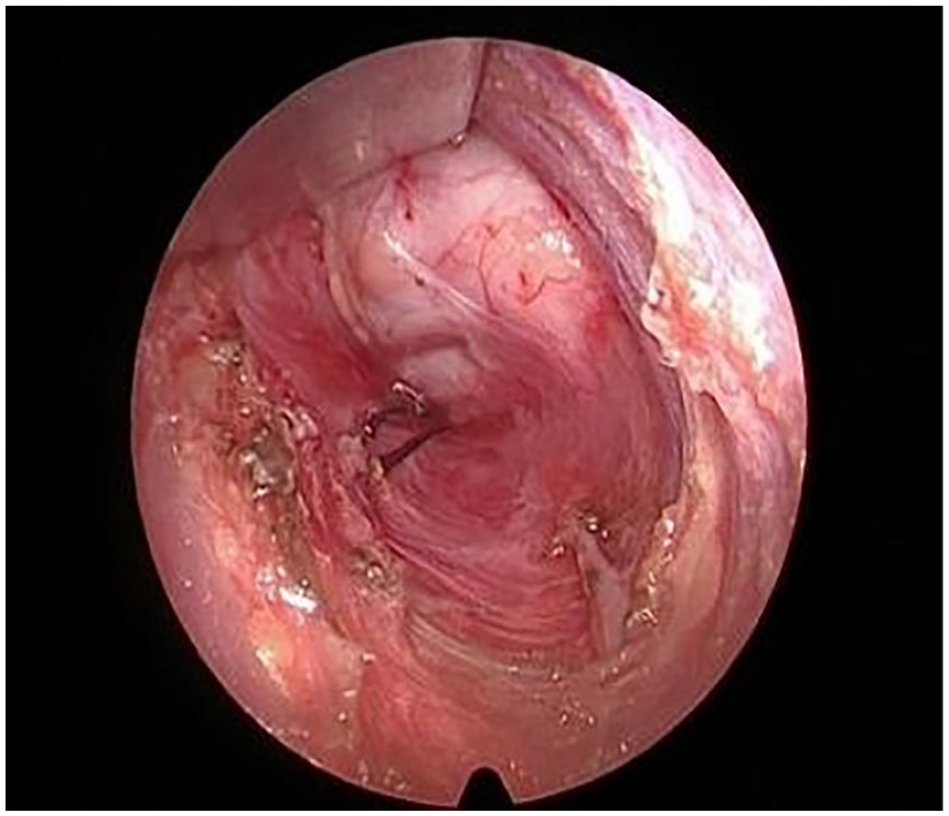
The fistula is ligated on the outside of the tonsillar capsule.
Types II, III, and IV second branchial cleft fistulas were noted to have larger diameters during the operation and were easy to recognize, meaning they could be identified using ultrasonography. These fistulas were usually surrounded by muscle bundles, forming a loose cavity with surrounding tissues, and were easy to separate.
Postoperative antibiotics were applied as appropriate, and incisional sutures were removed 7 days after the surgery. All children were followed up regularly after the operation.
Results
A total of 76 patients were enrolled, including 33 boys and 43 girls, with ages ranging from 1 to 13.5 years (average age, 5.8 years). In all, 43 patients had lesions on the right side, 20 on the left side, and 13 were bilateral, yielding a total of 89 lesions. There were 49 type I lesions, 28 type II lesions, 8 type III lesions, and 4 type IV lesions. These cases included 46 cervical fistulas which were visible immediately after birth and 18 fistulas which discharged fluid later in life, of which 23 lesions presented recurrent infection. Fistulas were found in 4 lesions after infection, whereas 10 lesions manifested without fistulas following repeated cervical infections. Small orifices with caseous discharge were noted on 2 lesions, whereas cervical nodules were observed in 9 cases. In total, 8 lesions had a history of drainage of cervical abscesses.
The diameter of the fistulas measured by ultrasonography for type III and type IV second branchial cleft is 0.25 to 1 cm. The trapezoidal incision was used in 2 type III branchial cleft fistula, whereas a single horizontal long incision was applied in 2 type III fistula. Furthermore, single incision-assisted endoscopic resection of the fistula was used in 4 type III and 4 type IV branchial cleft fistula.
All the children were pathologically confirmed to have branchial cleft fistula after surgery. Three patients experienced postoperative infection, all of whom recovered after anti-inflammatory treatment. No complications occurred in the remaining cases. The patients were followed up for 6 to 60 months. There were no cases of recurrence after the operation. The 4 type IV lesions were followed up from 26 months to 41 months, and no recurrence was observed.
Discussion
With the advancement of embryological research, Wenglowski first proposed the theory of branchial cleft cyst origin in 1912. 5 At present, the pathogenesis of branchial cleft malformation is not completely determined. The explanation theories regarding its development include branchial apparatus theory, cervical sinus theory, thymopharyngeal theory, and inclusion theory. Among these, the most widely accepted theory is that incomplete involution of the branchial apparatus causes branchial abnormalities. 6 Branchial cleft cysts and branchial cleft fistulas are common in children but can also appear in adults.6,7 Kalra et al. 6 showed in their study of second branchial cleft fistulas that the average age of onset was 5.56 years and the average age of fistula emergence was 5.79 years. Karabulut et al. 8 reported an average age of 5.30 years. Sinus or fistulas are often diagnosed earlier than cysts, as cysts may take longer to appear clinically. 6 In a study of 52 patients with second branchial fistulas with an average age of 5 years (range, 1-13 years) and a male-to-female ratio of 2.7:1, Rattan et al. 9 identified 41 patients with unilateral branchial cleft fistulas, including 29 cases on the right side and 12 cases on the left. Simpson 10 reported a male-to-female ratio of 3:1. However, Chandle et al. 11 reported a slight female predominance in the second branchial cleft fistula cases. In this study, the average age of onset was 4.8 years, and the ratio of male to female was 1:1.5, indicating a slight female predominance. According to previous reports, fistulas and sinuses were more common on the right side,4,12 with bilateral branchial cleft fistulas accounting for 2% to 3%. 13 In this study, right lesions were more common than left lesions, which is consistent with the results of previous reports. Nine children had bilateral branchial cleft fistulas, indicating it was not uncommon. According to literature reports, complete second branchial cleft fistulas are extremely rare. 14 In this study, type I was the most common type, whereas type IV was only diagnosed in 4 lesions, accounting for 4.5% of the cases; these findings are consistent with those in the previous literature.
The external orifices of branchial cleft fistulas are usually visible at birth. Choi et al. 15 reported that the most common symptoms were discharge from the cervical fistula, cervical mass, and recurrent infections. However, this abnormality can easily be overlooked for several years if no infection occurs. The clinical manifestations are often confused with other common head and neck diseases, such as lymphadenitis and localized infection. In our study, a large proportion of cervical fistulas did not present until several years after birth or, in some cases, until cervical fistula infections occurred. Therefore, branchial cleft fistulas should be considered in children with a history of recurrent cervical infections. In addition, the second branchial cleft fistula is often confused with the work type II first branchial cleft fistula 16 since the external orifices of both can be seen underneath the mandible. Work type II first branchial cleft fistula generally originates from the inferior wall of the external auditory canal, runs through the parenchyma of the parotid gland or the superficial surface of the masseter fascia, and passes through and ends in Pochet’s triangle on the ipsilateral hyoid bone. The lesion can travel on the superficial surface of the facial nerve, or be located on the deep surface or branches of the facial nerve. 17 This type of branchial cleft fistula is often closely related to the parotid gland. The second branchial cleft fistula, however, is often located deeply or medially in the submandibular gland and extends to the bifurcation of the carotid arteries. Therefore, we believe that these 2 types of fistulas can be differentiated according to the relationship between the fistula and the parotid or submandibular gland. In addition, it should be differentiated from thyroglossal fistula and pyriform sinus fistula. 18
Imaging examinations are important for the evaluation of the fistula tract. The route of the second branchial fistula is relatively regular. Ultrasonography is sufficient for most cases and is advantageous as it avoids the radiation involved with computed tomography (CT), as well as the costs added by MRI use. 19 CT and MRI examinations are only used for fistulas with unclear or atypical ultrasound imaging. Type I and type II second branchial cleft fistulas can be easily diagnosed by ultrasound. Preoperative ultrasound cannot accurately distinguish type III and type IV second branchial fistula, making it necessary to inject methylene blue to trace fistulas during operation.
Currently, exposure to the fistula is difficult due to the long tract of the fistula for type III and type IV second branchial cleft fistulas. Various surgical modalities have been reported in the literature for second branchial cleft fistulas. Some scholars have proposed an excision approach using a large hockey stick incision to fully expose the cervical structure. 20 Stepwise excision is currently mostly used because it allows good exposure to the fistula.2,9 In this technique, which was first proposed by Bailey in 1933, 21 dissection of the parapharyngeal segment is performed through the mouth, after which tonsillectomy is performed, and the fistula is removed through the mouth postoperatively. Since the late 1990s, endoscopic techniques have been used more and more frequently in head and neck surgeries. Chen et al. reported their experience with endoscopy-assisted resection of 13 cases of branchial cleft cysts, 12 reporting that a post-auricular incision of approximately 4 cm in length was required in all patients. They reported that endoscopy-assisted techniques, with small, esthetic incisions, had advantages in reaching upper cysts. Süslü et al. 20 described an endoscopy-assisted technique to reach upper cervical lesions through a 1-cm incision in the lower neck. Minimally invasive endoscopy-assisted surgery was proposed to help track the fistula and to directly magnify the internal orifice of the fistula, thus avoiding the need for a second incision. The carotid sheath, hypoglossal nerve, glossopharyngeal nerve, and other tissues are clearly visible and can be effectively dissected. Another advantage of endoscopic surgery is the minimal postoperative scarring compared with traditional surgical methods.
This study retrospectively analyzed the surgical treatment of the second branchial cleft fistulas in our department in recent years. The diameter of the fistula varied from 0.25 to 1 cm, which is wide and easy to identify after injection of methylene blue. In the early stage, we used either a trapezoidal incision or a single long incision for type III and type IV branchial cleft fistulas. These 2 methods can expose the root of the fistula, allowing the fistula to be easily cut off following ligation. None of the patients treated with this technique have experienced recurrence so far. However, this surgical method leaves a large scar, which not only affects the children’s appearance but also has psychological effects. In the later stage, we tried to adopt the single small incision combined with endoscopy-assisted fistula resection in 8 cases. During the operation for the 8 cases, the diameter of the fistula was noticeably large, and a strip-shaped muscle bundle was seen around the fistula. Separation was fairly easy around the muscle bundles, and a circular cavity was formed around the fistula in the deep regions of the submandibular gland. The fistula crossed the hypoglossal nerve and glossopharyngeal nerve, meaning that considerable care had to be taken to avoid damaging the blood vessels and nerves. This kind of small incision under endoscopic surgery leaves only small scars and, therefore, achieves a good esthetic effect. Furthermore, none of the patients have experienced recurrence. Therefore, this minimally invasive surgical method is aesthetically pleasing, effective, and safe.
It is necessary to perform tonsillectomy at the same time as the branchial cleft fistula is removed in the traditional surgical method of complete second branchial cleft fistula. 22 However, some scholars have proposed that the removal of tonsils does not affect the recurrence rate.23-25 In our study, the type IV second branchial cleft fistula was dissected to the level of the pharyngeal constrictor and then cut off following ligation. The tonsils were not removed. The patients were followed up from 26 months to 41 months, and no recurrence was found after surgery. However, there were only a few cases of type IV second branchial cleft fistula in this study. Whether it is necessary to remove the tonsils needs further support from case studies.
Conclusion
Our study has a large number of cases. The second branchial fistula is mainly characterized by external orifices and infection. Different incision design is chosen according to ultrasonography and classification. For type III and type IV second branchial cleft fistula, mini-incision with endoscopy-assisted fistula high ligation and resection ensures a clear operative field, achieving an ideal cosmetic effect and a high rate of cure.
Footnotes
Author Contributions
Y.L. designed and wrote the manuscript. S.W. and J.Z. drafted and revised the manuscript. N.S. acquired the data. Q.L., Z.L., and X.Z. analyzed the data of patients. X.N. designed the surgical procedure and approved the final version of the article. All authors contributed to the final manuscript. All authors read and approved the final manuscript.
Consent Statement
All the authors listed have read through the manuscript, approved for publication, and declared no conflict of interest.
Data Availability
The data used to support the findings of this study are available from the corresponding author upon request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Beijing Science and Technology Commission Capital Clinical Treatment Technology Research and Translation Application Project by (Z201100005520077), Capital Health Development Scientific Research Project (2022-1-2092).