
Abstract
Branchial cleft anomalies are embryonic remnants of the branchial arches and are described as the second most common congenital neck mass. Depending on their extent, these anomalies are classified as a cyst, sinus, or fistula with branchial cysts being the most common. Branchial cysts deriving from the second branchial arch are by far the most common, accounting for approximately 95% of all cases. Complete second branch arch fistulas with both an internal and external opening are a rare variant of this anomaly, and even less have been well-documented on computed tomography (CT) imaging in the literature. We present here a case of a 20-year-old female with CT findings consistent with a complete second branchial arch fistula extending from the tonsillar fossa to the external lateral neck.
Introduction
Branchial cleft anomalies are embryonic remnants of the branchial arches which in utero form the face and neck precursors. If these structures are not obliterated during fetal development, they may persist to varying degrees along the associated branchial arch developmental tract. They are well described throughout the literature and are described as the second most common congenital neck mass, behind thyroglossal duct cysts. 1 Traditionally, branchial cleft anomalies are subcategorized based off their arch derivative with second branchial arch anomalies accounting for nearly 95% of all cases. 2 The anomalies derived from this arch can occur anywhere along the second arch tract from the skin overlying the supraclavicular fossa to entering the pharynx at the level of the tonsil. 3 In addition, anomalies are classified as cysts, sinuses, or a fistula with the latter being the least common. While second branchial arch fistulas have been noted to occur in clinical medicine, a complete fistula formation with both an internal and external opening that is well characterized on computed tomography (CT) is extremely rare. Here, we present a case of a complete branchial cleft fistula in an otherwise healthy adolescent female.
Case Report
Patient is a 20-year-old female who presented for evaluation of lifelong punctate area in the right lateral cutaneous neck that has intermittently been infected and treated with antibiotics. She has experienced multiple prior episodes of tonsillitis in addition to 2 to 3 episodes of streptococcus pharyngitis within the past year. These episodes were treated with amoxicillin, Augmentin, Bactrim, and/or Medrol. She noted that during times of tonsillar enlargement and infection, there has been drainage from the site on her neck. On examination, tonsils were 2+ bilaterally, and there was a small opening at the right cutaneous lower neck with no active drainage and fluid was unable to be expressed. Neck CT with contrast was ordered and showed what appeared to be a second arch derivative, complete branchial cleft fistula extending from the cutaneous skin opening superiorly to an opening in the right tonsil (Figures 1 and 2). Decision was made to proceed with elective surgical excision and tonsillectomy.
In the operating room, following standard endotracheal intubation, a lacrimal probe was used to slightly dilate and define the fistulous tract from the skin opening. The tract was dissected superiorly in a plane deep to the digastric muscle and traced over the hypoglossal nerve and superiorly until it communicated with the pharynx. A right tonsillectomy was then performed in the standard fashion and elevated from the pharyngeal constrictor muscle, removing with it the fistulous tract via the oral cavity in its entirety. The gross specimen measured approximately 12 cm in length (Figure 3).

Computed tomography of the neck—sagittal view.
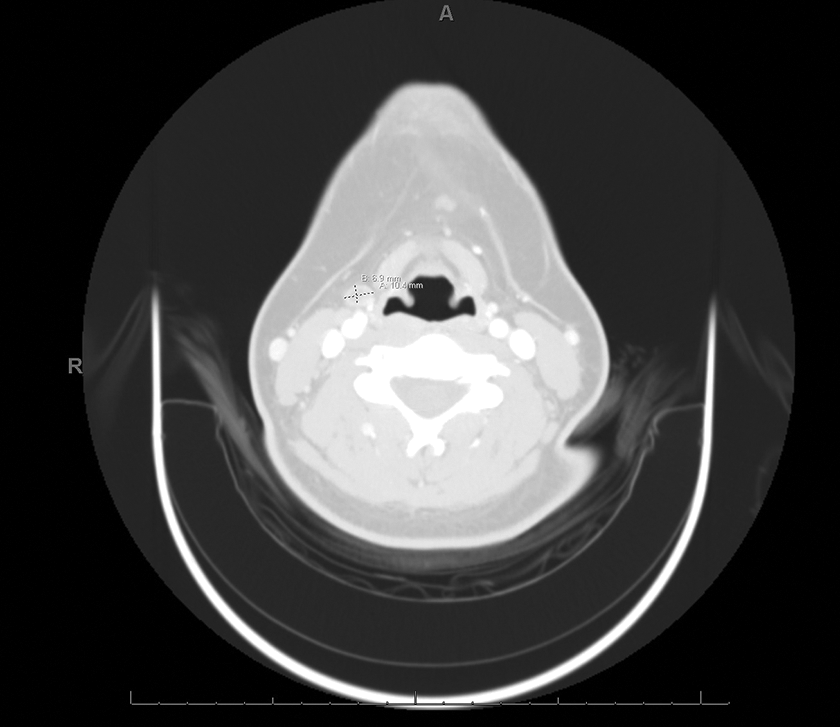
Computed tomography of the neck—axial view.

Intraoperative gross specimen following surgical resection.
Discussion
The branchial apparatus develops in utero at approximately 4 weeks gestation and derives muscular, nerve, and skeletal components. The pharyngeal arches are masses of mesoderm from the branchial apparatus, covered by ectoderm and lined internally by endoderm. Each branchial arch is separated both externally and internally by small grooves called clefts and pouches, respectively. These clefts and pouches will migrate toward each other to form a membrane, while the mesoderm or arch will grow and obliterate the cleft and pouch. Failure of this process can result in a collection of fluid in the form of a cyst, sinus, or fistula depending on the severity of the remnant.
Each pharyngeal arch ultimately develops into important anatomical features of the head and neck. The second branchial arch in particular contains Reichart’s cartilage which is the precursor to the stapes, stylohyoid ligament, styloid process, and upper body and lesser horn of the hyoid. In addition, cranial nerve VII, and the stapedial artery are derived from this branchial arch. Lack of obliteration along the second branchial arch pathway often results in a fluid filled cyst, sinus, or fistula extending along the anterior border of the sternocleidomastoid muscle superiorly toward the oral cavity and ipsilateral tonsillar fossa. Therefore, these tracts are closely associated with major neurovascular structures of the neck making a sound understanding of the pertinent anatomy important for the surgical resection.
Although a few case reports of complete branchial cleft fistulas have been described previously in the literature,4,5 characterization of the entire fistula on CT imaging is less documented. Visualization of the entire fistula tract via this approach is helpful for both the diagnosis and surgical planning of the resection as it correlates with the surrounding anatomy, specifically the neurovascular structures of the head and neck. In addition, the presented images in this study can serve as an educational for the learner of the branchial apparatus.
Conclusion
Complete branchial cleft fistula with both an internal and external opening is a rare variant of an otherwise common congenital neck defect. Although difficult to see completely on imaging, we present here a very well-characterized complete fistula on CT of the neck extending from the tonsillar fossa to the cutaneous neck.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.