
Abstract
Pleomorphic adenoma (PA) is the most prevalent benign tumor of the salivary glands, characterized by both epithelial and mesenchymal differentiation. It primarily originates within the parotid and submandibular glands, with only rare occurrences in the minor salivary glands. PA in the sinonasal area is extremely rare. Herein, we present a case of a 61-year-old female with a large soft tissue mass in the paranasal sinus and nasal cavity, as evidenced by computed tomography imaging. The patient suffered from repeated nasal congestion for more than 6 months. Eventually, the mass was completely resected using an endoscopic endonasal prelacrimal approach under general anesthesia. Postoperative pathological examination revealed the presence of PA in the nasal sinus.
Introduction
Among all the pleomorphic adenoma (PA) originating from the salivary glands, 75% occur in the parotid gland, 15% in the submandibular gland, and the remaining 10% arise from the minor salivary glands. 1 Given that the minor salivary glands are distributed throughout upper aerodigestive tract, PA of the minor salivary glands can occur in the trachea, lacrimal gland, larynx, pharynx, soft palate, hard palate, floor of the mouth, and nasal cavity.1 -3 PA occurring in the nasal cavity is rarely reported, with only around 120 documented cases, 4 while PA of the maxillary sinus is even more uncommon. According to Kuan et al., PA originating from the maxillary sinus accounts for only 7 of the 39 cases of all PAs in the skull base and nasal cavity. 5
PA typically manifests with unilateral or bilateral nasal obstruction and epistaxis as primary symptoms. The diagnosis of PA can be challenging due to the nonspecific nature of these symptoms and the findings of radiological examinations. Computed tomography (CT) scans often reveal a well-defined, lobulated expansile growth mass, with some cases demonstrating calcifications within the tumor and adjacent bone changes. 6 The osteolysis phenomena of carcinoma ex-PA (an infiltrative carcinoma arising from a primary or recurrent benign pleomorphic adenoma) and PA are 71.4% and 10%, respectively, 7 so osteolysis phenomena may indicate malignancy of the tumor. In contrast, the magnetic resonance imaging (MRI) findings of PA often reveal a T1-weighted low- to medium-intensity signal and a T2-weighted medium- to high-intensity signal.
Although PA is a benign tumor, it can recur. According to reports, the recurrence rate of PA in the nasal cavity is between 5.1% and 10%.3,8,9 The reason for recurrence may be that the tumor-negative margins were not reached or that there is microscopic recurrence from residual pseudopodia resulting from incomplete excision.7,10 The primary approach for addressing PA involves the complete removal of the tumor with clear margins. A review of scientific literature via the PubMed and Web of Science databases revealed a notable scarcity of English articles pertaining to maxillary sinus PA cases. Moreover, only a few instances of sinonasal PA in Chinese patients have been reported in English articles, but no case reports regarding maxillary sinus PA in Chinese patients were identified.
Herein, we describe a case of PA found in the right sinonasal tract, detailing its the main clinical and pathological features. Furthermore, we conducted a comprehensive review of the limited literature on sinonasal PA.
Case Report
A 61-year-old female presented to the outpatient clinic at Wuhan Union Hospital in January 2023 with a history of persistent nasal congestion lasting over 6 months. She complained of right-sided nasal congestion of unknown origin, accompanied by sensations of head fullness. Of note, the patient had previously undergone anti-infective treatment at a local clinic, but her symptoms showed no improvement. A paranasal sinus CT examination revealed the presence of an intrasinus mass located in both the right maxillary sinus and ethmoid sinus (Figure 1A and E). Subsequent MRI imaging revealed an oval-shaped lesion characterized by a T1-weighted low-intensity signal intermixed with a T2-weighted high-intensity signal, measuring 40 mm × 27 mm × 41 mm in size (Figure 1B-D, F-H). Interestingly, upon administration of contrast, the enhancement of the lesion appeared markedly uneven. Besides, the demarcation between the mass and the right-side middle and inferior turbinate was indistinct, and partial obscurity of the lesion’s boundary was observed in relation to the ethmoid sinus.
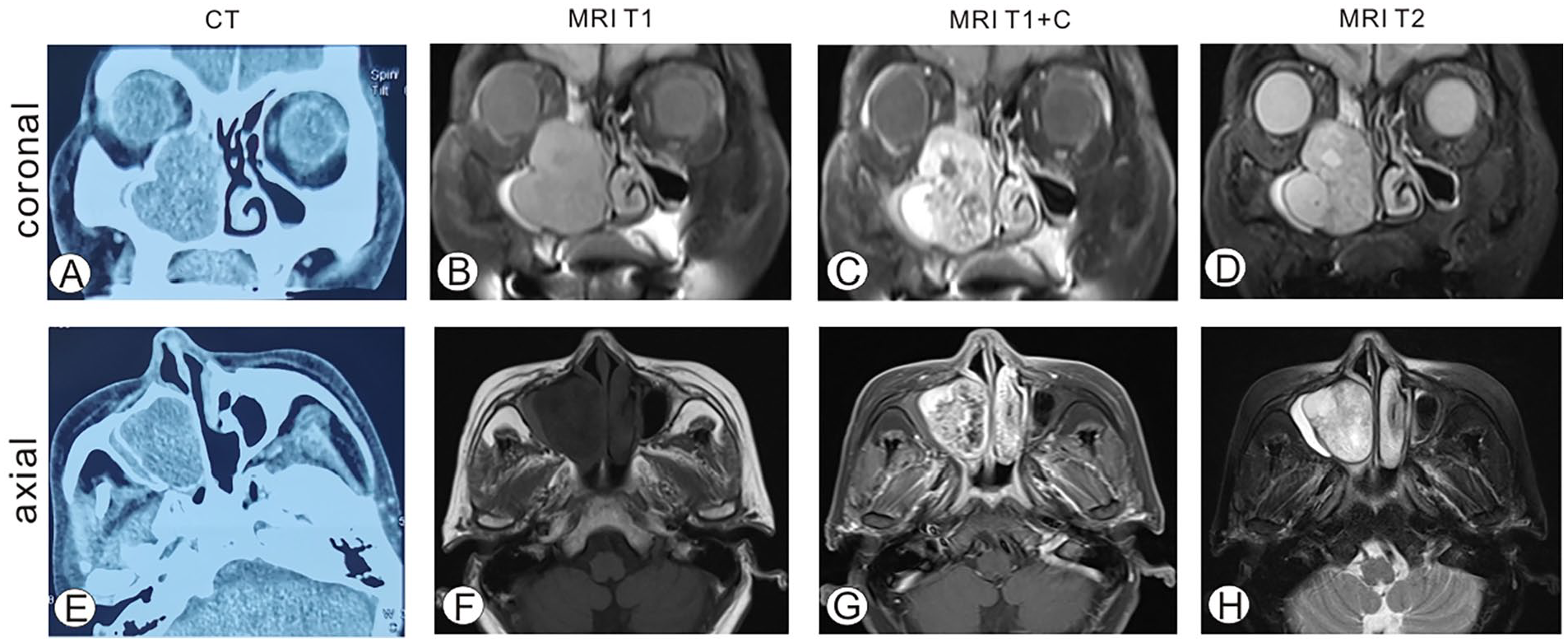
Radiological examinations of the paranasal sinus. (A) Coronal CT scan reveals a soft tissue density shadow in the right nasal cavity and maxillary sinus, measuring 40 mm × 27 mm × 41 mm in size. (B,D) Coronal MRI scans showing an oval-shaped T1-weighted low-intensity signal mixed with T2-weighted high-intensity signal shadow in the right nasal cavity and right maxillary sinus. The enhancement was obviously uneven upon contrast administration (C). The boundary between the mass and the right-side middle and inferior turbinates was unclear, and the boundary with the ethmoid sinus is partially indistinct. T2 high-intensity signals were seen in both maxillary sinuses, ethmoid sinuses, and right frontal sinuses, with thickened and enhanced mucosa, and the right ethmoid sinus was significantly affected (D). (E) Axial CT scan shows a soft tissue density shadow in the right nasal cavity and maxillary sinus. (F,H) Axial MRI imaging shows uneven enhancement upon contrast administration (G).
Subsequently, the patient underwent resection of the lesion using the endoscopic endonasal Prelacrimal approach (PLA) under general anesthesia. During the intervention, we observed that the right nasal cavity was constricted, and a pathogenic growth was visible in the right maxillary sinus. The boundary was still clear, and the content was gelatinous in nature. Notably, the tumor invaded the lamina papyracea. The excised tissue was promptly sent to the pathology department for further examination.
Postoperative histopathological examination indicated the presence of a salivary gland-type tumor (Figure 2A), consistent with PA. Immunohistochemical staining (Figure 2B-I) revealed the following: PCK(+), CK7, EMA, SMA, p63, CK5/6, SOX10 showed biphasic differentiation, and Ki67 (LI: <5%). The presence of epithelial components (PCK, CK7, EMA, CK5/6) and mesenchymal components (SMA, SOX10) exhibited the mixed characteristics of the tumor. Following resection, the patient did not report any specific sinonasal symptoms such as nasal obstruction or discharge, or loss of smell.
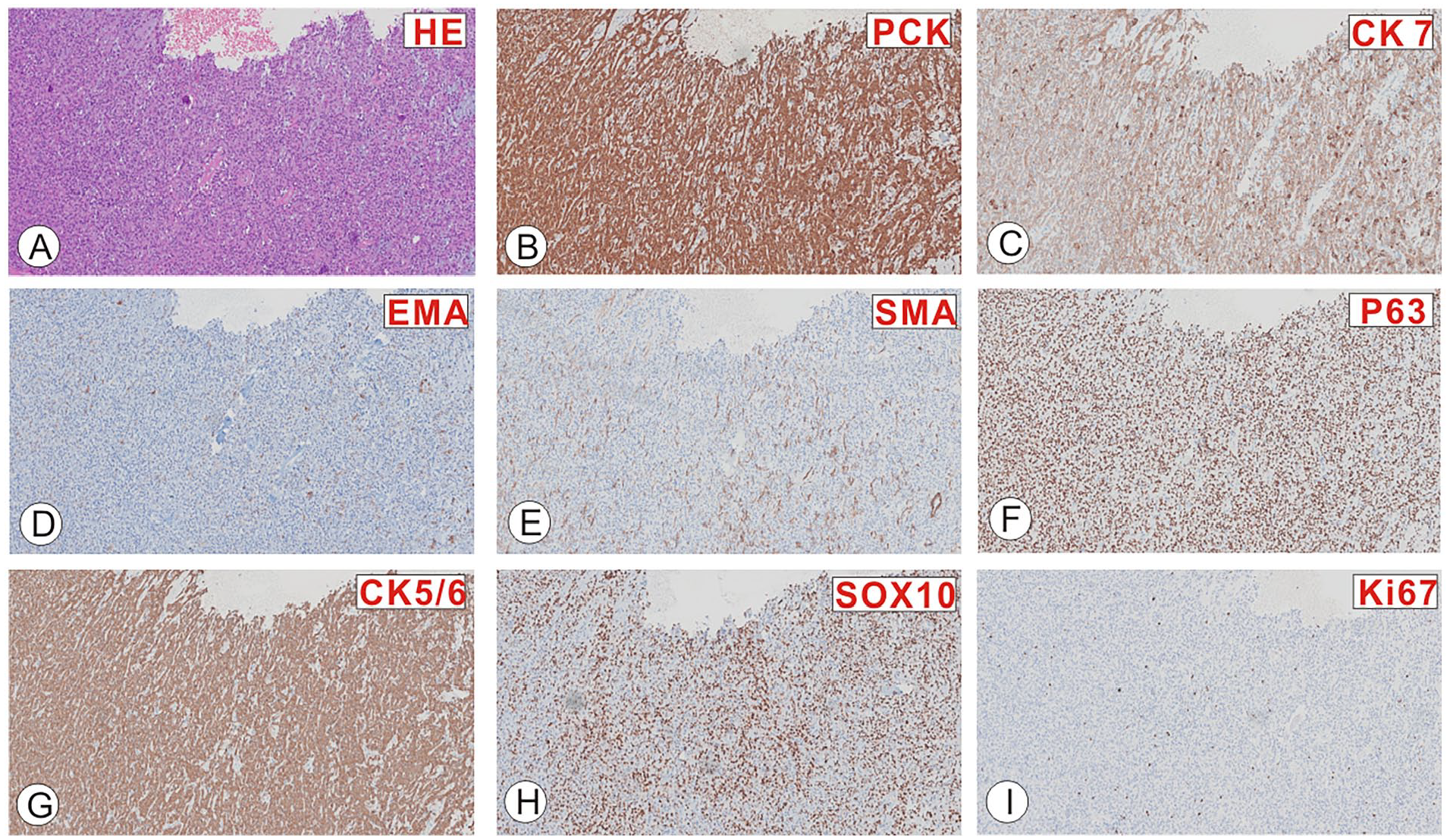
Histologic analysis of specimens. (A) Microscopic examination of the HE-stained specimen revealed pathological features of a salivary gland-type tumor, consistent with pleomorphic adenoma. (B) Immunohistochemical staining confirmed the presence of tumor cells positive for PCK. (C-H) The tumor cells showed biphasic differentiation for CK7 (C), EMA (D), SMA (E), p63 (F), CK5/6 (G), and SOX10 (H). (I) The tumor cells were positive for Ki67 (LI: <5%) staining.
Discussion
PA primarily manifests in the parotid gland and submandibular glands, with less frequent occurrences in the minor salivary glands. Its occurrence in the sinonasal region is particularly rarer. Nevertheless, sinonasal PA is a crucial condition that demands careful consideration as a differential diagnosis, as it shares symptoms and features with other diseases.
The average age of onset of nasal PA is 44 years old, with around 80% of reported cases affecting female patients.11,12 A study conducted in Korea, encompassing 101 patients with sinonasal PA, reported an average age of 45.4 years and found that 59.4% of the patients were female. Furthermore, 57.4% of cases exhibited PA in the septum, 15.8% in the lateral nasal wall, and 7.9% in the inferior turbinate. Paranasal sinus involvement is very rare, with only 5.9% of PA occurring in the maxillary sinus and 1% of PA occurring in the frontal sinus. 4
The most common symptom of PA is unilateral or bilateral nasal obstruction and epistaxis. 13 Patients may also present with symptoms such as a nasal mass, cheek swelling, mucopurulent rhinorrhea, epiphora, and hearing loss. 4 Sinonasal PA usually appears as a well-defined, homogeneous soft tissue mass on CT imaging. 13 Differentiating between benign and malignant PA often hinges on identifying changes in the surrounding bone, with the presence of osteolysis indicative of malignancy. On MRI imaging, PA exhibits low to medium signal intensity on T1-weighted imaging and medium to high signal intensity on T2-weighted imaging. Nevertheless, due to the nonspecific nature of the symptoms and examination findings associated with sinonasal PA, the definitive diagnosis of PA relies on histopathological examination, 14 and P63 and KI67 proliferation index can be used to reflect the possible malignant areas in the tumor. 15
While PA is generally considered a benign tumor, it can exhibit recurrence or even undergo malignant transformation. Rha et al. previously reported that 8 out of 101 patients with sinonasal PA experienced recurrence, with a rate of 7.9%. 4 According to Wanpeng Li et al., the recurrence rate of benign PA patients was 10% during an average follow-up period of 2.2 years (range from 0.5 to 5.3 years). 7 Meanwhile, Vento et al.’s 6-month follow-up study revealed that none of the 10 patients experienced recurrence 11 . Approximately 6% of all existing benign PAs are prone to malignant transformation, and this risk tends to increase over time.16,17 The recurrence of sinonasal PA does not appear to be significantly correlated with tumor size but is related to the site of origin. 4 Notably, the occurrence of PA in the paranasal sinuses is significantly linked to a high recurrence rate, 4 which may be attributed to the anatomical challenges associated with achieving en bloc resection with clear margins.
The primary treatment for PA involves complete surgical removal of the tumor with clear margins. 10 En bloc resection is of particular importance in preventing PA recurrence. The recurrence rate in patients who underwent en bloc resection was only 4.8% (1/21), while 20% of cases undergoing piecemeal resection experienced tumor recurrence (1/5). 4 The endoscopic endonasal approach is particularly advantageous in achieving excellent visualization of the tumor margin, facilitating en bloc resection with clear margins, and contributing to successful PA management.
PA has demonstrated limited sensitivity to radiotherapy, and there is ongoing debate regarding the necessity of adjuvant radiotherapy following surgery. The focus of controversy is that radiotherapy may cause malignant transformation of the tumor. 18 In addition, radiotherapy can lead to an increased complication incidence. In cases involving intraoperative tumor spillage, residual tumors, or recurrence, the utilization of radiotherapy for PA is a subject of consideration but continues to be a matter of controversy. 18 Adjuvant radiotherapy postoperatively has proven effective in reducing the recurrence rate of pleomorphic adenomas with positive incisal margins or multiple nodules. It can also be beneficial in patients at a high risk of developing recurrent PA after surgery, as it helps control subclinical disease. 19
Due to the potential for recurrence, long-term follow-up and monitoring of patients is essential. Recurrence typically occurs with an average time frame of 7 years after surgery, although it can manifest anywhere between 9 months and 20 years post-surgery. As a recommended practice, patients should undergo follow-up examinations monthly within the first 6 months after surgery, followed by subsequent follow-ups every 3 to 6 months. Lifelong follow-up is also strongly recommended to ensure timely detection of any recurrence or complications. 5 In situations where the primary site cannot be directly observed through nasal endoscopy, regular MRI or CT examinations become necessary. In this specific case, a follow-up was conducted 6 months after surgery, with no evidence of recurrence.
In conclusion, sinonasal PA is a very rare benign tumor and represents a crucial differential diagnostic entity. Its symptoms and imaging findings are nonspecific, necessitating histopathological examination for definitive diagnosis. The primary treatment for PA entails complete surgical excision of the tumor with clear margins. Given the propensity for recurrence in sinonasal PA, diligent postoperative follow-up is imperative. Herein, we present a case of sinonasal PA originating from the maxillary sinus, which was successfully managed through endoscopic sinonasal tumor resection via a PLA. Importantly, no evidence of tumor recurrence was observed during the six-month postoperative follow-up period.
Footnotes
Authors’ Contributions
TZ, J-X Shen, YT, and G-J Chen designed and supervised the work. Z-H Zhang drafted the article. HC and M-Z Zhou conceived and designed the report; HC, J-X Yue, Q-L Zhou, Y-J Wu, and TZ diagnosed, treated, and followed the patients; and participated in the collection of clinical data. All authors have read and approved the final version of this article.
Data Availability Statements
All data generated or analyzed during this research are included in this published article. Data supporting the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was financially supported by the National Natural Science Foundation of China (82201301, CH), Natural Science Foundation of Hubei Province (2022CFB087, ZT), the Research Grant of Union Hospital, Tongji Medical College, HUST (F016.02004.21003.126, ZT), and Open Project of Key Laboratory of Molecular Imaging (2022fzyx015, TZ).
Ethical/Consent Statement
Not applicable.