
Abstract
Anaplastic thyroid carcinoma is a rare and aggressive form of thyroid cancer that has a poor prognosis and a high mortality rate. It is characterized by rapid growth and invasion of nearby tissues. It typically presents as a rapidly growing goiter or nodule that is firm to the touch and firmly attached to the underlying structures. Case reports of unusual presentations of anaplastic thyroid carcinoma have been reported. The presentation of anaplastic thyroid carcinoma mimicking cervical tuberculosis is very unusual. We reported a case of a 65-year-old patient who had a left cervical swelling that had been evolving for 4 months, causing dysphagia. Initial imaging showed a necrotic mass in the left lobe of the thyroid, communicating with a second necrotic mass in the subcutaneous tissue that was fistulized to the skin and suggesting cervical tuberculosis. The mass was incised with pus and whitish material resembling caseous tuberculosis was discharged. Acid-fast bacilli (AFB) Polymerase chain reaction (PCR) was negative and biopsy revealed a nonspecific granulomatous lesion. Due to the growth of the mass and the presence of a permeation nodule, a second biopsy was performed, revealing anaplastic thyroid carcinoma. The patient was referred for radiochemotherapy due to tumor inoperability.
Key Clinical Message
Anaplastic thyroid carcinoma, a highly aggressive type of thyroid cancer, can exhibit unusual clinical symptoms. We presented a rare case of anaplastic thyroid carcinoma resembling cervical tuberculosis. Despite their uncommon presentation, it is crucial not to postpone the diagnosis and treatment of these aggressive cancers due to their dismal prognosis.
Introduction
Cancer and tuberculosis are 2 common diseases that affect health worldwide. They affect various organs and typically present with different clinical manifestations. However, these 2 diseases can sometimes present with unusual but similar clinical manifestations, leading to misdiagnosis of cancer and tuberculosis. 1 The thyroid gland is not spared from this risk of diagnostic error. It is more common for thyroid tuberculosis to be misdiagnosed as thyroid cancer than the opposite.2,3 In fact, thyroid tuberculosis is a great mimic and diagnostic chameleon and is prone to be diagnosed as thyroid carcinoma.2,3 However, thyroid cancer is very rare to present as cervical tuberculosis. To our knowledge, only 3 cases of thyroid carcinoma, initially manifesting as a neck abscess, have been reported.4 -6 In this report, we describe a very rare case of an adult who presented symptoms similar to cervical tuberculosis and pathological results that ultimately revealed anaplastic thyroid carcinoma.
Case Report
A 65-year-old patient presented to our service with a left-sided basi-cervical swelling that had been evolving for 4 months. The swelling had increased progressively over the last 2 months, causing dysphagia. The swelling was 8 cm in diameter, with indistinct margins, was immobile during swallowing, and had indurated and soft areas. It was fistulized on the skin.
The blood count showed hyperleukocytosis of 13,600 cells/mm3 (85% neutrophils, lymphopenia: 8.5% lymphocytes, i.e., 1,200/mm3), normocytic normochromic anemia with hemoglobin level of 9.3 g/dL, and platelets of 307,000/mm3. CRP was high at 69 mg/L.
Cervical computed tomography showed a necrotic mass in the left lobe of the thyroid compressing the airway, communicating with a second necrotic mass in the subcutaneous tissue of the anterolateral cervical region, and extending to the left sternocleidomastoid muscle. This mass was fistulized on the skin and initially suggested cervical tuberculosis (Figure 1).
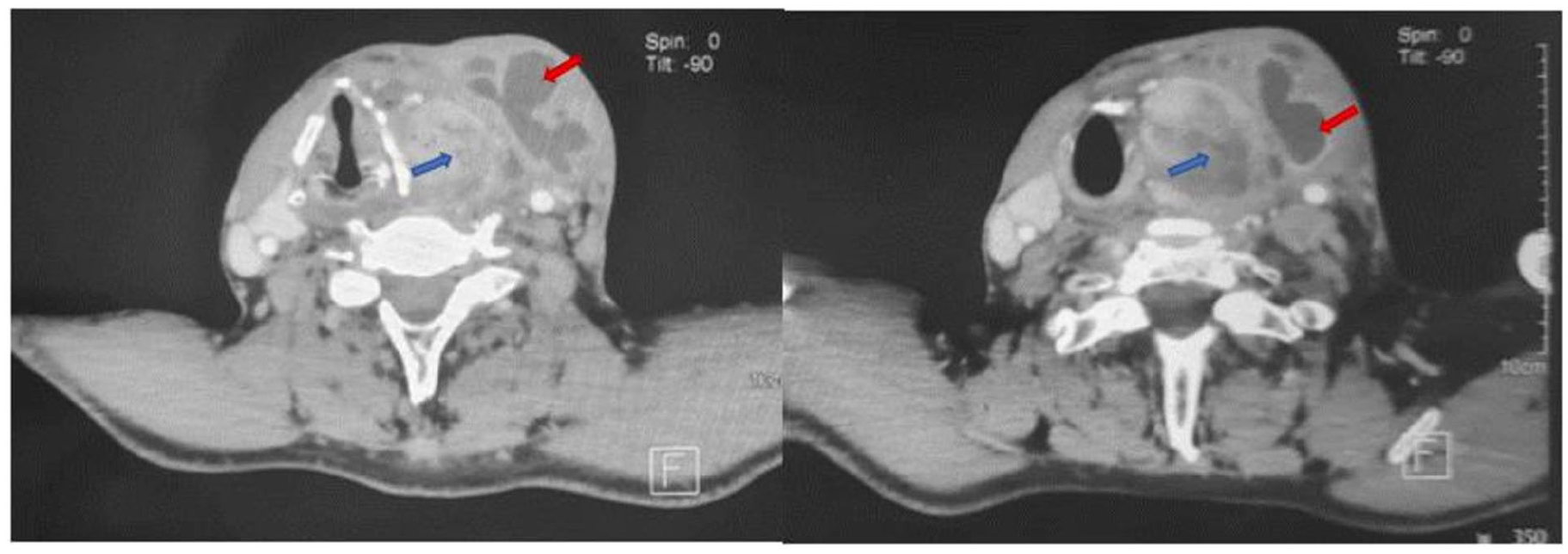
Axial cervical CT with contrast injection: Left-sided cervical mass (blue arrow) in contact with the eroded thyroid cartilage, displacing the airway to the contralateral side. It is associated with a homolateral necrotic subcutaneous mass (red arrow), communicating with the first mass at some points and extending to the left sternocleidomastoid muscle.
When the subcutaneous mass was punctured and incised, pus and whitish material that resemble caseous tuberculosis were discovered. Biopsies of the fistula margins and the abscess wall concluded a nonspecific granulomatous lesion. Acid-fast bacilli (AFB) PCR was negative.
For 15 days, the patient received antibiotics intravenously. A regression of local inflammatory signs and biological inflammatory syndrome was noted. However, the mass increased in size, softened, and a friable tumor tissue appeared in the permeation orifice.
A second biopsy of this tissue revealed an anaplastic thyroid carcinoma. Immunohistochemical analysis showed tumor cells that express keratin, Epithelial membrane antigen (EMA), and Paired-box gene 8 (PAX8) diffusely and intensely. Tumor cells were focally positive for Thyroid Transcription Factor-1 (TTF1) (Figure 2).
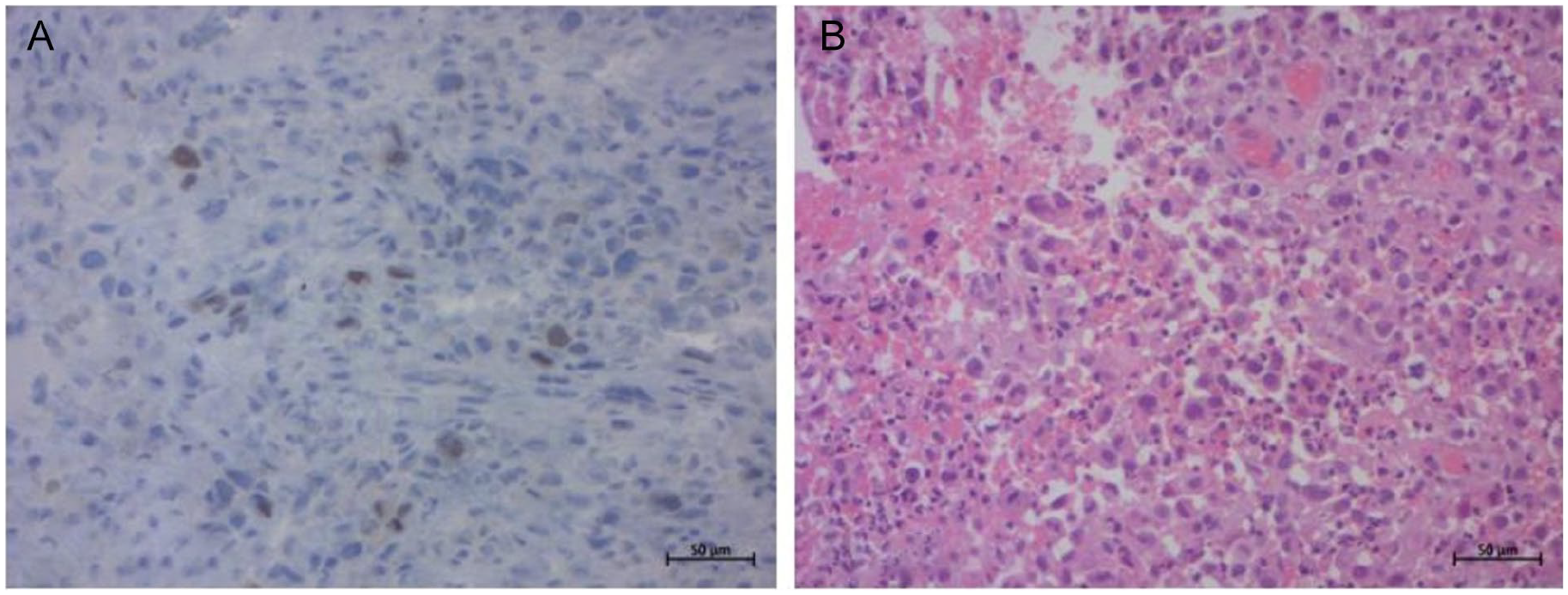
Histological findings. (A) Diffuse proliferation of dyscohesive atypical tumor cells admixed with inflammatory cells. The tumor cells have basophilic cytoplasm and irregularly enlarged nuclei, often with a prominent nucleolus. The mitoses are numerous. (HE ×200). (B) Tumor cells showed focal positivity for TTF1 (×200).
A second computed tomography showed tumor growth in the left thyroid mass that invades the esophageal wall, the prevertebral plane, and covers more than half the circumference of the left internal carotid artery. Suspect bilateral jugulo-carotid lymph nodes had also appeared (Figure 3).
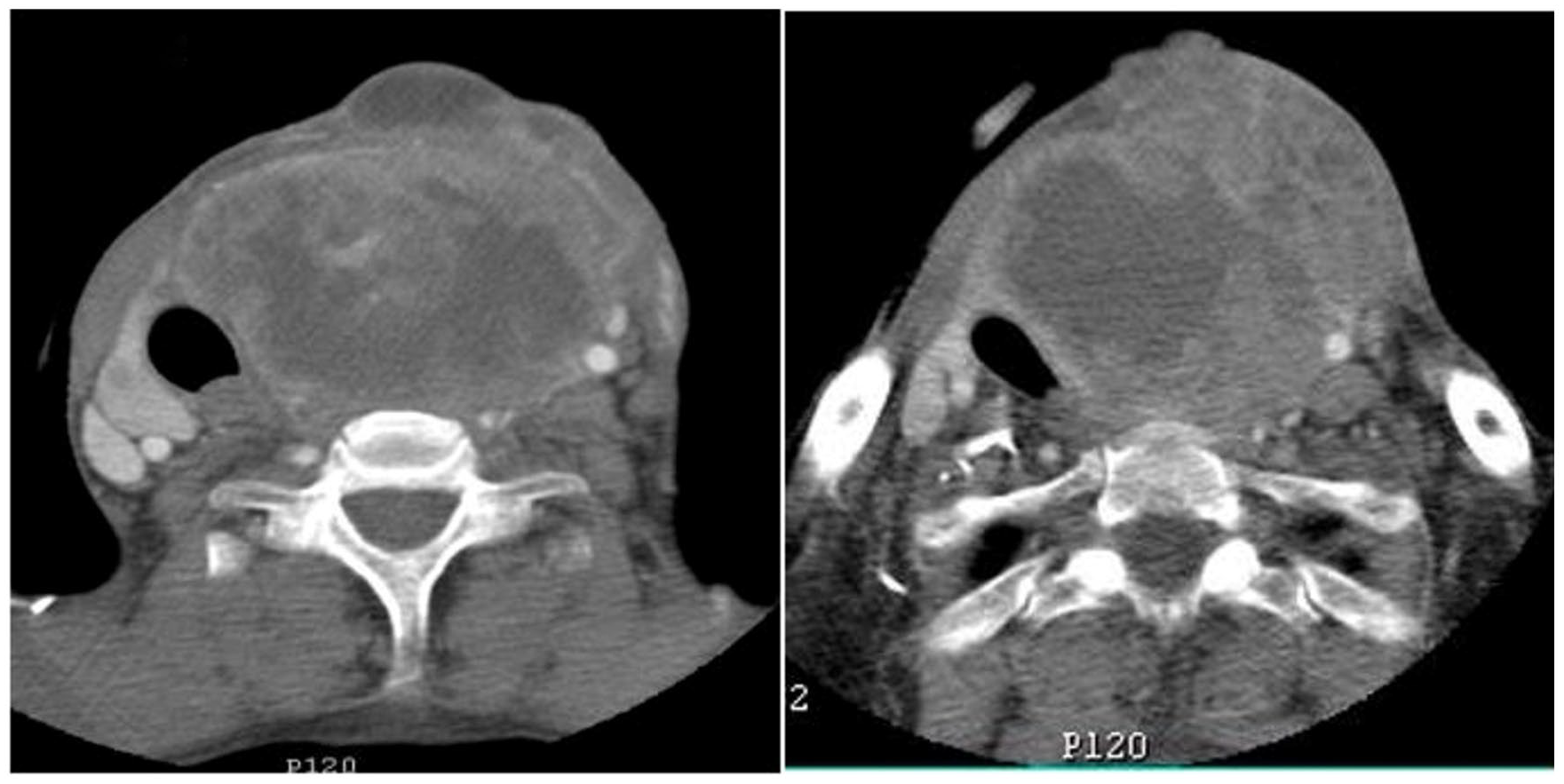
Axial cervical CT with contrast injection: Important increase in the size of the left thyroid mass, with areas of necrosis, displacing and compressing the trachea and esophagus with signs of involvement of the subcutaneous tissue and prevertebral plane. Encasement of the left common carotid artery over more than half of its circumference and compression of the left jugular vein.
Both a Positron Emission Tomography (PET) scan and a computed tomography of the thoracoabdominopelvic region did not reveal any distant hypermetabolic foci. Following a multidisciplinary consultation meeting, the patient was referred for radiochemotherapy due to the inoperability of the tumor.
The patient underwent the initial course of chemotherapy treatment. Progression was characterized by an increase in tumor size, worsening dysphagia, and a decrease in overall health. Unfortunately, the patient died after 1 month of starting chemotherapy due to deteriorating general condition.
Discussion
Although tuberculosis and cancer are 2 completely different diseases, they can present with unusual but similar symptoms that can overlap and mimic each other. In fact, misdiagnosis of cancer and tuberculosis has been reported in various organs, such as the lungs, liver, breast, bones, and even the thyroid gland. 1 It is more common for thyroid tuberculosis to be misdiagnosed as thyroid cancer than the opposite.2,3 Many cases of thyroid tuberculosis incorrectly diagnosed as thyroid cancer have been associated with pressure symptoms such as dysphagia, 7 dyspnea, and recurrent laryngeal nerve palsy, 8 raising suspicion of malignancy. However, it is very unusual for thyroid cancer to present as cervical tuberculosis. In our case, tuberculosis was suspected due to the insidious progression of cervical swelling, the appearance of a skin fistula with the discharge of pus and a whitish material reminiscent of the tuberculous caseum, as well as the central necrosis of the mass on CT while taking into account the high prevalence of tuberculosis in the country.
Anaplastic thyroid carcinoma represents approximately 2% of all thyroid cancers. 9 It is a particularly dreaded form of cancer due to its extreme aggressiveness and poor prognosis. It is most frequently in the elderly, with a mean age distribution between 60 and 79 years and is slightly more common among women (1.5:2 ratio). 9
Anaplastic carcinoma is believed to arise from a terminal dedifferentiation of preexisting carcinomas of the thyroid follicular cell. This association has long been suggested by the consistent observation of coexisting follicular or papillary thyroid carcinomas with anaplastic carcinoma. 10 The classic presentation of anaplastic thyroid carcinoma is a rapidly growing large goiter or nodule that is firm to the touch and attached to the underlying structures. Signs of local–regional invasion are common, including inspiratory dyspnea, dysphonia due to recurrent laryngeal nerve paralysis, dysphagia, and cervical pain. More than 80% of patients have cervical lymph node metastases at presentation and 20% to 50% have systemic metastases. 11
Case reports of unusual presentations of anaplastic thyroid carcinoma include possible bradycardia due to compression of the vagus nerve, 12 superior vena cava syndrome, 13 thyrotoxicosis, 14 acute Horner’s syndrome, 15 leukocytosis due to granulocyte colony-stimulating factor secretion, and ball valve-type respiratory obstruction. 16 The presentation of anaplastic thyroid carcinoma mimicking cervical tuberculosis is very unusual and may be the first case reported in the literature.
Even rare similar cases reported in the literature were thyroid carcinomas mimicking the presentation of cervical abscess rather than tuberculosis.4 -6 In fact, Loh TL et al. 4 reported a rare case of anaplastic thyroid carcinoma that mimicked a thyroid abscess in a 52-year-old patient in 2018. Fine needle aspiration cytology was negative for malignancy. An incision and drainage were performed, and the histopathological result of a biopsy of an isolated proximal enlarged lymph node revealed metastatic carcinoma. The thyroid biopsy confirmed anaplastic thyroid carcinoma. Mahattanapreut et al. 5 reported a 67-year-old patient with a case presented with a large abscess affecting the retropharyngeal space, the orohypopharynx, the larynx, and the left lobe of the thyroid gland with multiple lymphadenopathies and cystic necrosis in 2021. Incision and drainage of the abscess were performed on the patient, and necrotic tissue samples were sent for histopathology. Papillary thyroid carcinoma was found in the pathology of necrotic tissue with lymph node metastasis. Lin et al. 6 conducted a study on the incidence of head and neck cancers that initially appeared as deep neck infections. Among the 81 patients with deep neck infections, 4 were found to have underlying cancers, including papillary thyroid carcinoma, nasopharyngeal carcinoma, hypopharyngeal carcinoma, and Hodgkin lymphoma.
To distinguish between the infectious process and the malignancy, a fine needle aspiration cytology should be performed. 17 However, cytological examination of cystic lesions of malignancy might yield a false negative result due to the dilutional effect of cystic fluid. In our case, even the biopsy of the abscess wall was initially negative. This can be attributed to the abundance of inflammatory cells, as the presence of a few atypical clusters of cells may go unnoticed. 17
The literature supporting specific guidelines for the treatment of anaplastic thyroid cancer is limited. Therapeutic options include surgery, radiation, and systemic therapy. 18 Similarly, incision and drainage of the cervical abscess underlying the tumor is part of treatment, although it can seed the tumor in soft tissues of the neck and skin as the loci break down, and encourage the dissemination of carcinoma cells. 17
Surgical removal of this rapidly progressing cancer is often not possible due to either extensive local disease or synchronous metastatic disease. Total thyroidectomy has been reported to increase survival rates in highly selected cases; however, cervical and mediastinal disease must be minimal. 19
The most critical aspect of therapy is controlling the local spread of the disease and its associated symptoms. Although anaplastic thyroid cancer has been considered radioresistant compared to other malignancies, several studies have shown that radiation therapy can effectively control local disease and alleviate symptoms in some cases. 20 Lastly, systemic therapy can be used to reduce the overall burden of the disease, although current chemotherapy regimens have not been shown to affect overall survival. Anaplastic thyroid carcinoma is known for its poor prognosis. The 5-year survival rate is less than 10%, and the average survival is 6 to 8 months regardless of treatment. 18
Conclusions
In conclusion, anaplastic thyroid carcinoma is an extremely aggressive form of thyroid cancer that can present with atypical clinical manifestations, leading to misdiagnosis. In this case report, we highlight a rare case of anaplastic thyroid carcinoma mimicking cervical tuberculosis, which underscores the importance of considering uncommon etiologies in the differential diagnosis of necrotic neck masses. Given the poor prognosis of these tumors, such an atypical presentation should not delay the diagnostic and, especially, therapeutic management of such aggressive cancers.
Footnotes
Acknowledgements
All authors approved the final version and have agreed to be accountable for all aspects of the work, including ensuring that questions related to accuracy.
Data Availability Statement
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent
Obtained from the patient in writing.
Informed Consent
A written informed consent was also obtained from the patient to publish this report in accordance with the journal’s patient consent policy.