
Abstract
The tracheoesophageal fistula (TEF) is an abnormal flow between the esophagus and the trachea. Most patients with TEF experience severe symptoms. Asymptomatic TEF is rare. In this case report, a 47-year-old woman planned to undergo orthopedic surgery under general anesthesia. She had no symptoms related to TEF, and the preoperative chest computed tomography was also normal. However, there was significant airway resistance after induction. Using a fiber bronchoscope, a TEF was discovered. The TEF found after anesthesia due to high airway pressure is unusual, and the outcome and treatment of these patients need to be further discussed.
Introduction
Tracheoesophageal fistula (TEF) is the abnormal flow between the esophagus and the trachea. It can be congenital or acquired. Congenital TEF is more common in infants and acquired TEF is mainly in adults. It is challenging because of its complicated origins, difficult diagnosis and therapy, and high death rate. Most patients with TEF experience the following symptoms: severe choking when drinking or eating, pain behind the chest wall, repeated attacks of suppurative bronchitis or pneumonia, repeated aspiration, and so on. Asymptomatic TEF is rare, especially in adults. A case of TEF found during general anesthesia was reported to improve the understanding and diagnosis of this disease.
Case Report
Written informed consent was obtained from the patient to publish this case report. The ethics committee waived informed consent for the study.
A 47-year-old female patient was admitted to our hospital after experiencing a left leg fracture caused by trauma. She was in good health before the accident. All preoperative examination including chest computed tomography (CT) was normal.
The patient was intended to undergo the reduction operation under general anesthesia combined with a sciatic nerve block. Vital signs were routinely monitored after entry. Her pulse oxygen saturation was 97%, blood pressure was 139/86 mmHg, heart rate was 79 bpm, and respiratory rate was 18 bpm. Routine induction was performed; at this time, the airway pressure was about 25 cm H2O. After implantation of the No. 4 laryngeal mask, the ventilation resistance was obvious and the respiratory sounds could hardly be heard. Endotracheal intubation guided by a visual laryngoscope was performed immediately, the intubation was successful, and the position of the tube was correct, but the resistance of the airway was still high. Meanwhile, the abdomen was gradually swollen and the end-tidal carbon dioxide did not show a waveform. Although the possibility of the silent lung could not be ruled out, treatment including bronchodilators had no effect. In summary, considering the abnormal anatomy of the trachea, a fiber bronchoscopy was performed immediately, and it was found that there was a fistula approximately 0.5 cm away from the carina beside the opening of the left main bronchus, so the TEF was diagnosed (Figure 1). Fortunately, there was no regurgitation of the digestive fluid in the trachea. After approximately 1 hr, the patient gradually returned to consciousness and had good spontaneous breathing. The tracheal tube was pulled out. She returned to the ward safely. At follow-up, the patient had no complications and confirmed that there were no symptoms and signs related to TEF previously.
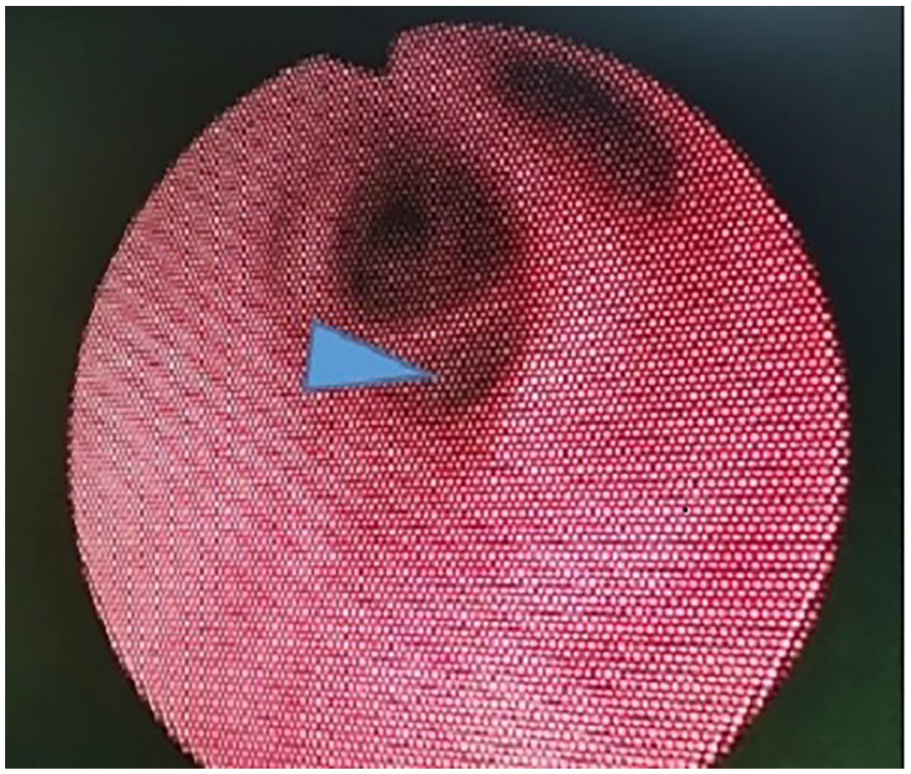
There was a fistula about 0.5 cm away from the carina beside the opening of the left main bronchus with fiber bronchoscopy.
Discussion
TEF is a connection between the trachea and the esophagus caused by abnormal development or disease of the esophagus and/or trachea. It can be caused by congenital malformations, advanced esophageal cancer, trachea tube cuff injuries, chest trauma, and so on. 1 Patients with TEF may have different clinical manifestations, depending on the speed of its formation, size, location, comorbidities, and immune status. Asymptomatic TEF is rare. The patient in our case has no symptoms, which may be related to the following reasons: (a) the esophageal fistula is low, the tracheal fistula is high, and the fistula can be closed by muscle contraction; (b) The mucosa at the orifice fistula forms folds, which produce a one-way valve when swallowing, and food is not easy to stray into the trachea. (c) The upward fistula prevents food from flowing into the lung under the action of gravity. It was proved via bronchoscopy that the fistula was congenitally formed since the mucosa around it was smooth and free of hyperplasia and scarring. During ventilation, gas entered the trachea, esophagus, and stomach through TEF, which caused high airway pressure and ineffective ventilation.
Previous reports have mostly diagnosed asymptomatic TEF through gastric distension during intraoperative positive pressure ventilation or air leakage after implantation of the correct type of tracheal tube. 2 In this case, gastric distension during ventilation was also observed, meanwhile, airway pressure increased obviously. The TEF was diagnosed by bronchoscopy after excluding esophageal intubation and the silent lung. In this situation, restoring the patient’s spontaneous breathing is prioritized. This is the first case report of an asymptomatic TEF in adults diagnosed based on high airway pressure during surgery.
Anesthesia management of patients with TEF includes awake endotracheal intubation, avoidance of muscle relaxants and positive pressure ventilation, and total intravenous anesthesia but no inhalation anesthesia, which has the risk of leakage. 3 Visualization of the fistula and cuff location by bronchoscopy can increase the success rate of ventilation. The use of single-lung ventilation is also one of the ventilation strategies for anesthesia management of patients with TEF. 4 In patients with esophageal cancer complicated by TEF, high-frequency jet ventilation can be used to reduce air leakage through the fistula, thus achieving a good ventilation effect. 5 The main treatment for TEF is endoscopic stent placement or surgical repair.
Asymptomatic congenital TEF is rare. However, for high airway pressure after induction, the possibility of airway anatomic abnormalities like TEF should be considered after excluding common factors such as anesthetic machine and respiratory circuit malfunction, catheter discounting, secretion blockage, severe bronchial spasm, and so on.
In addition, the sensitivity, specificity, and negative or positive predictive value of chest CT scanning for TEF are unclear. In chest CT, it is difficult to find the existence of a tiny fistula. When the fistula contains air, it can be found on chest CT, but the esophageal muscle is closed most of the time, which limits the finding of TEF during preoperative evaluation. Just like this case, the patient’s preoperative chest CT could not find TEF (Figure 2). An opposite situation existed. The presence of TEF was observed on imaging images, but no fistula was found under endoscopy. 6 Therefore, imaging and endoscopy are complementary in the diagnosis of TEF.
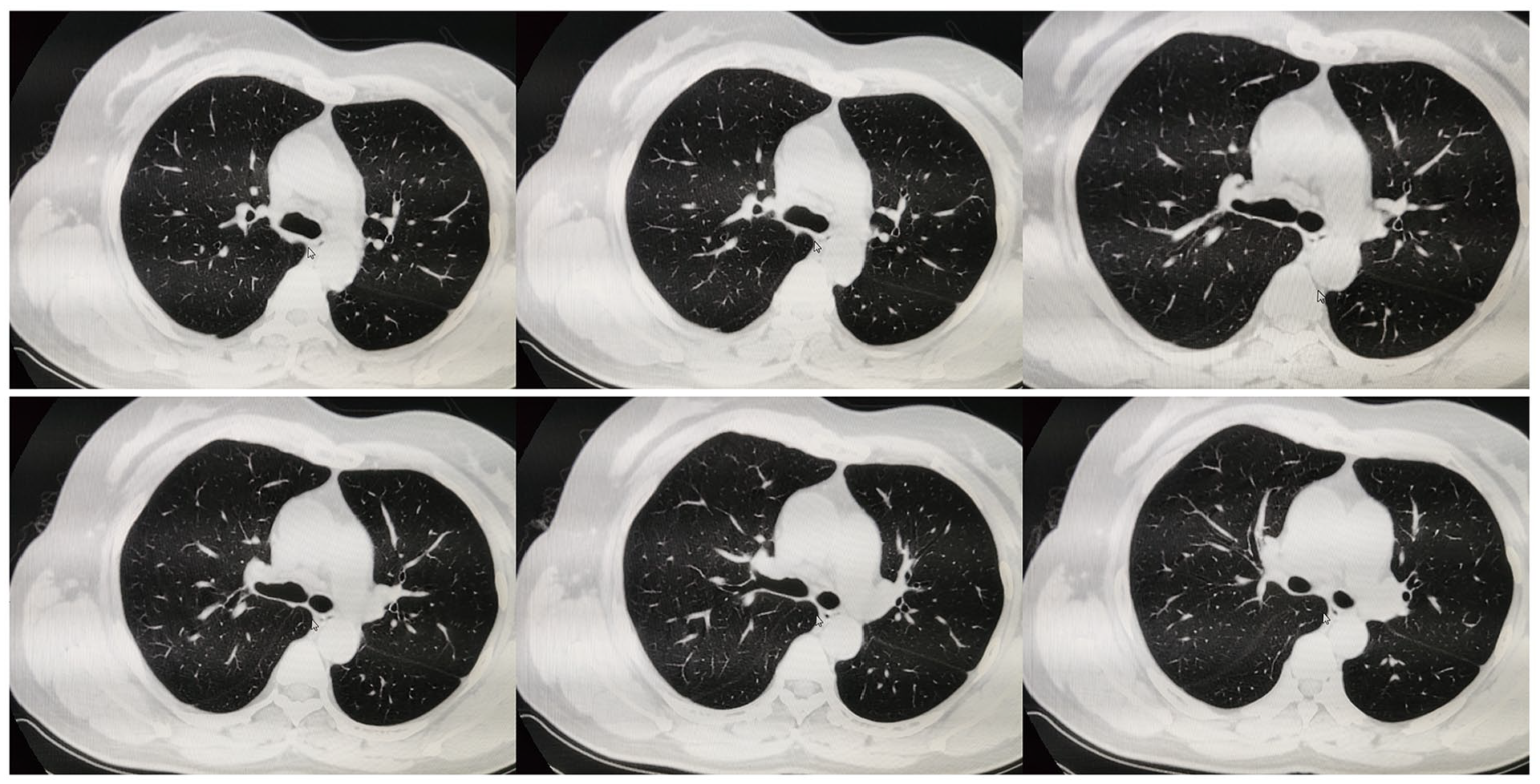
No tracheoesophageal fistula was observed from the main trachea to the left and right bronchus bifurcation on the patient’s preoperative chest CT.
We advised the patient to follow up with the Department of Thoracic Surgery, or ENT. Because asymptomatic tracheoesophageal fistula is so rare in adults, despite previous reports of surgical treatment in adult patients with asymptomatic TEF to prevent future complications,6,7 there is no clear data on whether, when, and how intervention is needed. The supplement of these data needs to be further explored in subsequent clinical practice.
Conclusion
To sum up, we present a rare case of asymptomatic TEF that was diagnosed by bronchoscopy during orthopedic surgery due to high airway pressure after anesthesia induction. The follow-up treatment and outcome of such patients remain to be further discussed.
Footnotes
Acknowledgements
Thanks to Tiancai Yang for providing the case, and thanks to Peng Liang and Xiaoqian Deng for their suggestions on the revision of this article.
Data Availability Statement
This case report does not involve data collection, processing, or analysis. Instead, it emphasizes the uniqueness and practicality of the case, rather than relying on data-driven analysis or statistics. Therefore, there is no need to provide information on data sources, acquisition processes, or data availability.
Author Contributions
Y.F. and T.Y. wrote the first draft of the article.
T.Y. was directly involved with patient care.
P.L. and X.D. made strict revisions to the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.