
Abstract
Metastatic papillary thyroid carcinoma in the lymph nodes without a primary tumor in the thyroid gland is rarely reported. We report the case of a 63-year-old male who had a left neck level II palpable mass. A left cervical mass had previously undergone 2 central needle biopsies, but only atypical cells had been identified. His prior medical history included surgical treatment for prostate cancer 11 years ago. There was no suspicious primary tumor in the endoscopic examination. After the excisional biopsy, the pathologic finding was metastatic papillary carcinoma from the thyroid, and there were no aberrant findings in the thyroid sonography. The patient underwent a complete thyroidectomy, bilateral central neck dissection (CND), and left level IV dissection, along with postoperative radioactive iodine (RAI) therapy. No thyroid lesion and no more positive lymph nodes were found in the final pathology report. Three months later, a radioiodine nuclear scan was performed, although it revealed no abnormal iodine uptake.
Introduction
The most common and treatable form of thyroid cancer is papillary thyroid carcinoma. 1 It typically presents as a palpable neck mass, and incidental ultrasound discovery of thyroid nodules is not uncommon. 2
When we detect enlarged cervical lymph nodes, we perform radiologic and cytopathologic evaluations on the lymph nodes to determine whether they are malignant. In addition, a comprehensive endoscopic evaluation of the head and neck area is performed to evaluate the primary site. However, if the primary head and neck cannot be identified, and a less invasive cytopathologic test fails to diagnose cancer, a surgical excisional biopsy of the lymph node is carried out. 3
The papillary thyroid carcinoma with lymph node metastasis but without a primary thyroid lesion is a rare phenomenon and presents a diagnostic challenge.4 -7 This article describes a case where metastatic papillary thyroid carcinoma was found in the cervical lymph nodes without a primary tumor in the thyroid gland.
Case Presentation
A 63-year-old man visited with a palpable mass in his left neck. He underwent a neck ultrasound examination, including the thyroid gland. The ultrasound examination showed multiple enlarged lymph nodes at level 2 on the left side. The lymph node measured 30.2 mm × 12.0 mm and had a predominantly solid component, an oval shape with a smooth margin, and no visible hilum. No abnormalities were found in the remaining parts, including the thyroid gland. A core needle biopsy was performed twice on the largest lymph node, which reported only atypical cells (Figure 1). These lymph nodes showed hypermetabolic uptake on F-18 fluoro-deoxy-glucose positron emission tomography, and no other pathological uptake was observed (Figure 2).
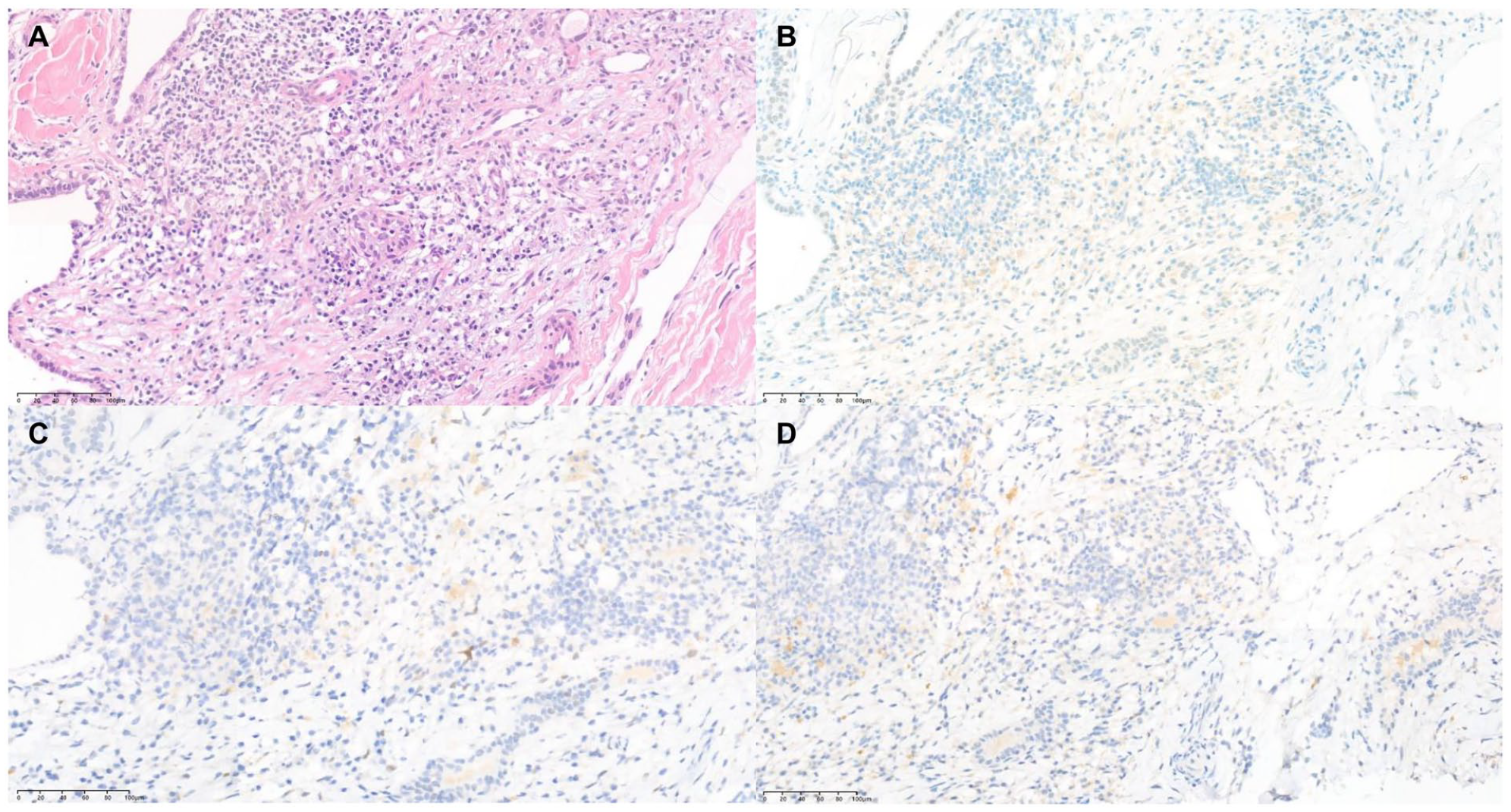
Histologic features of the left neck level III lymph node from core needle biopsy. Histopathology showed atypical cells suggestive of malignancy (A—hematoxylin-eosin, original magnification ×100). Immunohistochemical stain showed that negative to prostate specific antigen (B—hematoxylin-eosin, original magnification ×100), negative to androgen receptor (C—hematoxylin-eosin, original magnification ×100), negative to NXK3.1 (D—hematoxylin-eosin, original magnification ×100), and confirmed that it is not metastasis of prostate cancer.
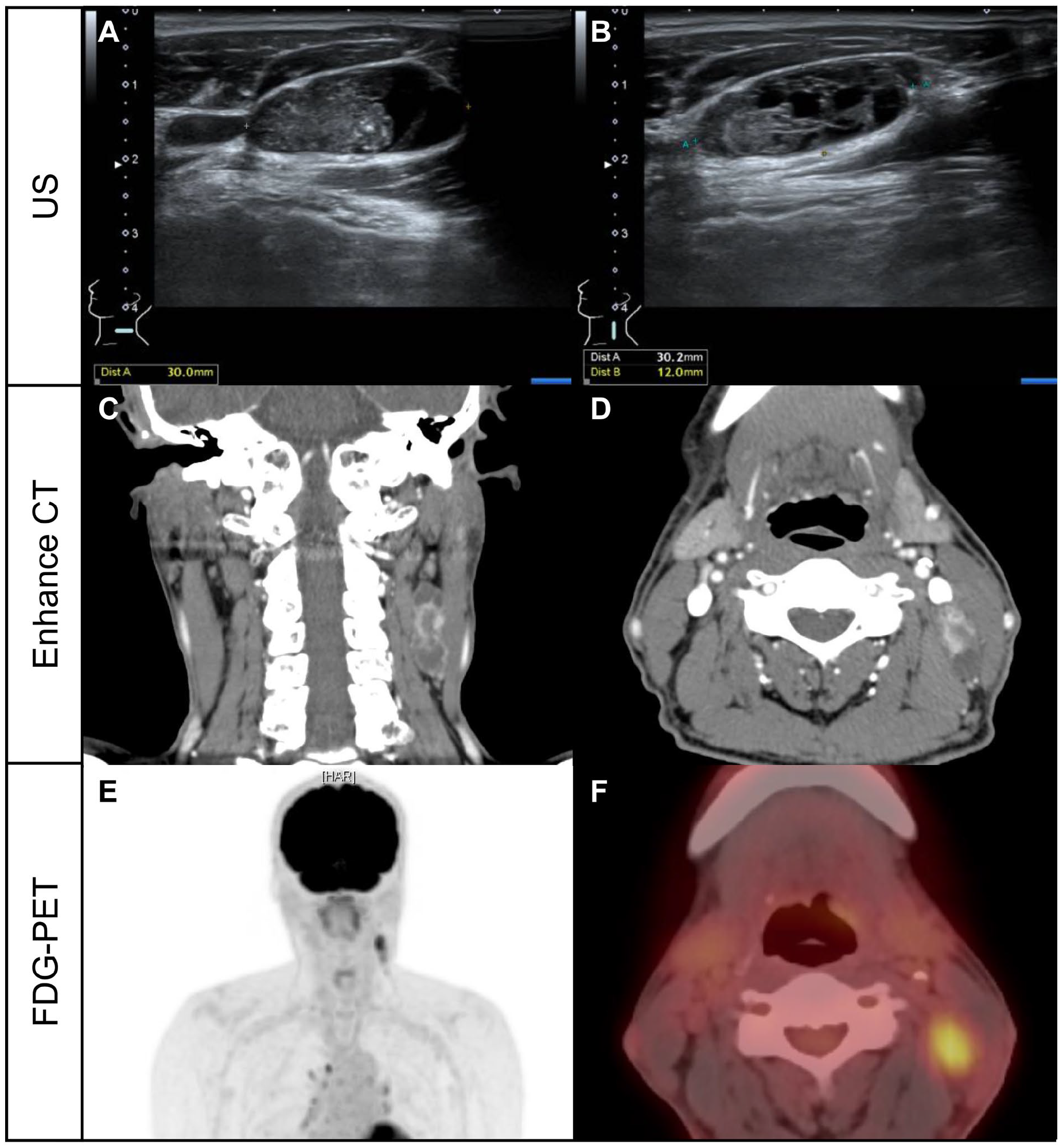
Initial imaging evaluation of left level II and III neck masses. The ultrasound examination showed multiple enlarged lymph nodes at levels II and III on the left side. The largest lymph node measured 30.2 mm × 12.0 mm and had a predominantly solid component, an oval shape with smooth margin, and no visible hilum (A and B). Enhanced CT scan revealed multiple rim-enhancing, enlarged cystic lymph nodes with irregular margins in the left neck at levels II and III (C—coronal view, D—axial view). Hypermetabolic uptake was observed in the lesions previously identified on enhance CT scan in FDG-PET, but there were no findings suggestive of lymph node metastasis or distant metastasis in other areas (E and F).
The patient had no specific symptoms such as fever, weight loss, or night sweats, and no abnormal findings were found on physical examination except for the palpable mass in the left neck (Figure 3). In his medical history, he underwent radical prostatectomy for prostate cancer 11 years ago and received salvage radiation treatment for operative bed recurrence 5 years ago. Routine blood tests, thyroid function tests, and thyroglobulin tests were normal before the surgery.
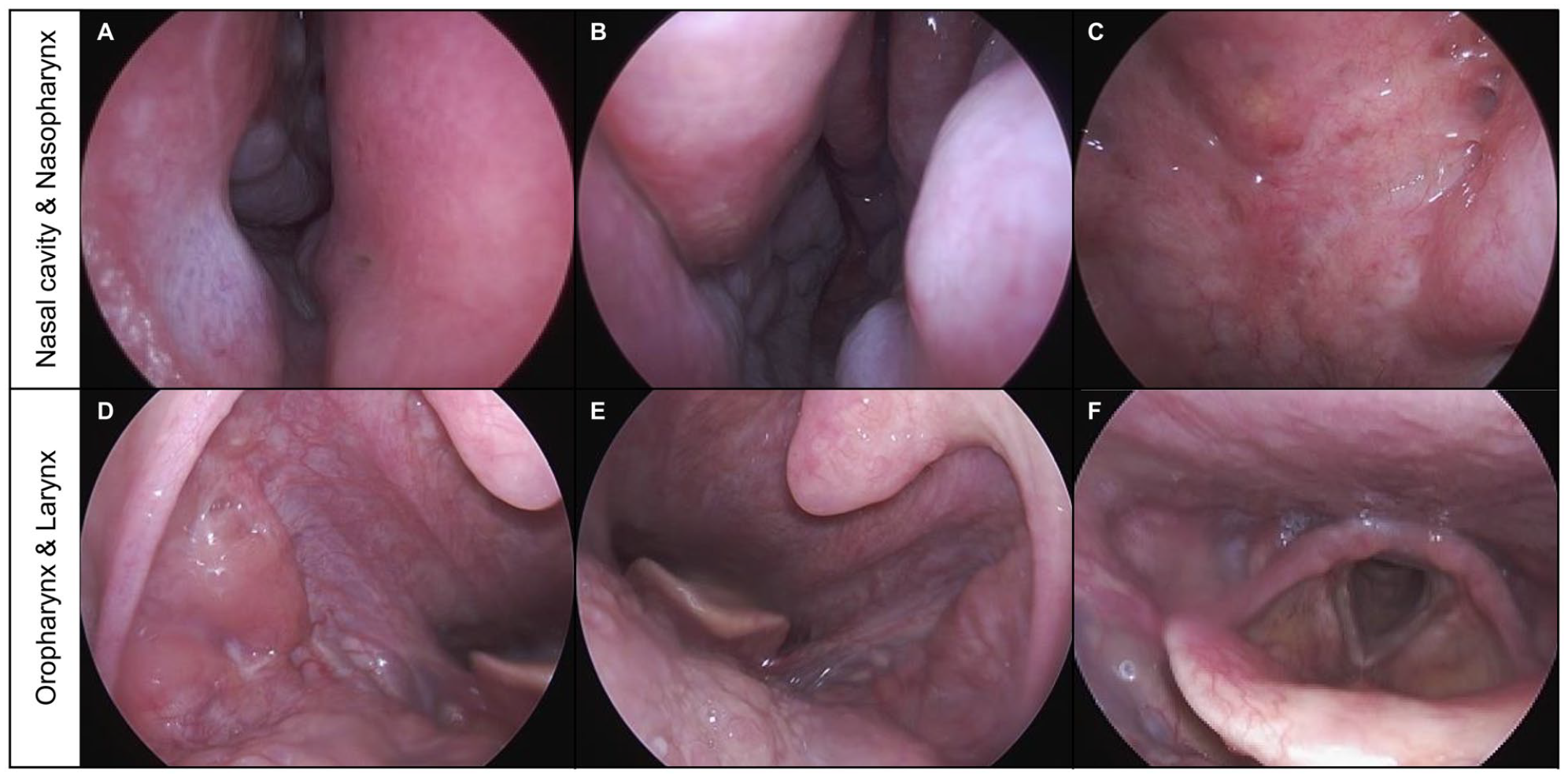
Preoperative pan endoscopic evaluation. The endoscopic examination showed no abnormal mucosal lesions in the nasal cavity and the nasopharynx (A—right nasal cavity, B—left nasal cavity, C—nasopharynx). Similarly, no mass or abnormal mucosal lesions were observed in the oropharynx, including the tonsillar area, and no significant findings were observed in the larynx (D—right oropharynx, E—left oropharynx, F—larynx).
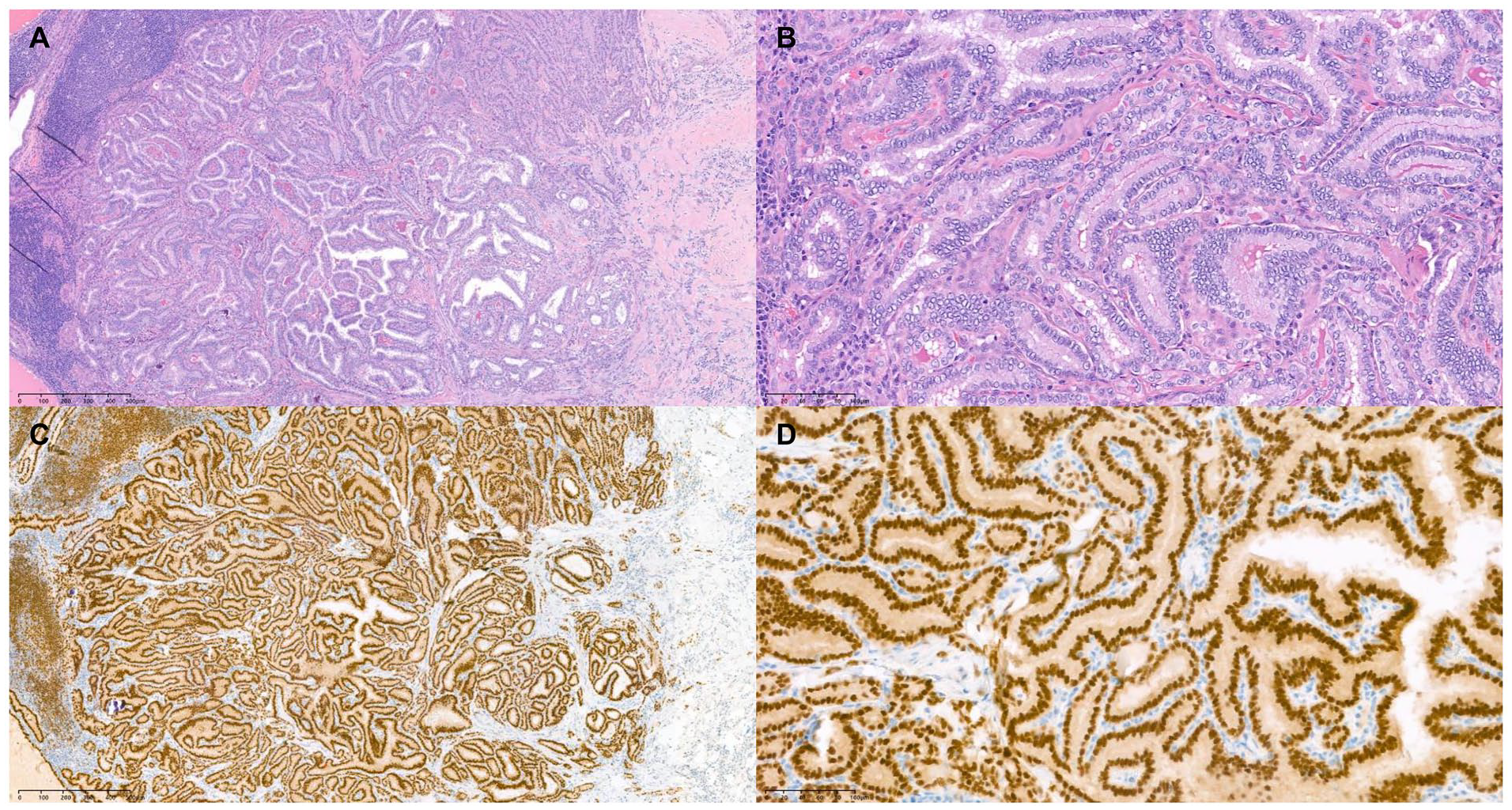
An excisional biopsy was performed on the left level II neck lymph node, and the final pathological diagnosis confirmed metastatic papillary carcinoma from the thyroid. Among the total of 12 lymph nodes, 3 had pathological findings, and the largest lymph node had a size of 2.2 cm with extranodal extension (Figure 4). The patient underwent a repeat thyroid ultrasound examination, which did not show any significant findings, including nodules. Surgical treatment, including total thyroidectomy, bilateral central neck dissection, and left level IV selective neck dissection, was recommended as additional therapy, and the patient agreed to undergo surgery. He recovered well without any complications after surgery, such as recurrent laryngeal nerve injury and hypocalcemia. Even though 2 pathologists thoroughly examined the tissue, no malignant tumor was found in the thyroid gland. Only nodular hyperplasia with a size of 0.2 cm × 0.1 cm × 0.1cm was found in the left lower lobe, and all 16 lymph nodes were reactive lymph nodes without any pathological lymph nodes (Figure 5).
Histologic features of the left lymph nodes from excisional biopsy. Histopathology confirmed metastatic papillary carcinoma from the thyroid, and the largest one measured 2.2 cm with extranodal extension (A—hematoxylin-eosin, original magnification ×25, B—hematoxylin-eosin, original magnification ×100). Immunohistochemical staining showed that it was positive for PAX 8 (C—hematoxylin-eosin, original magnification ×25, D—hematoxylin-eosin, original magnification ×100).
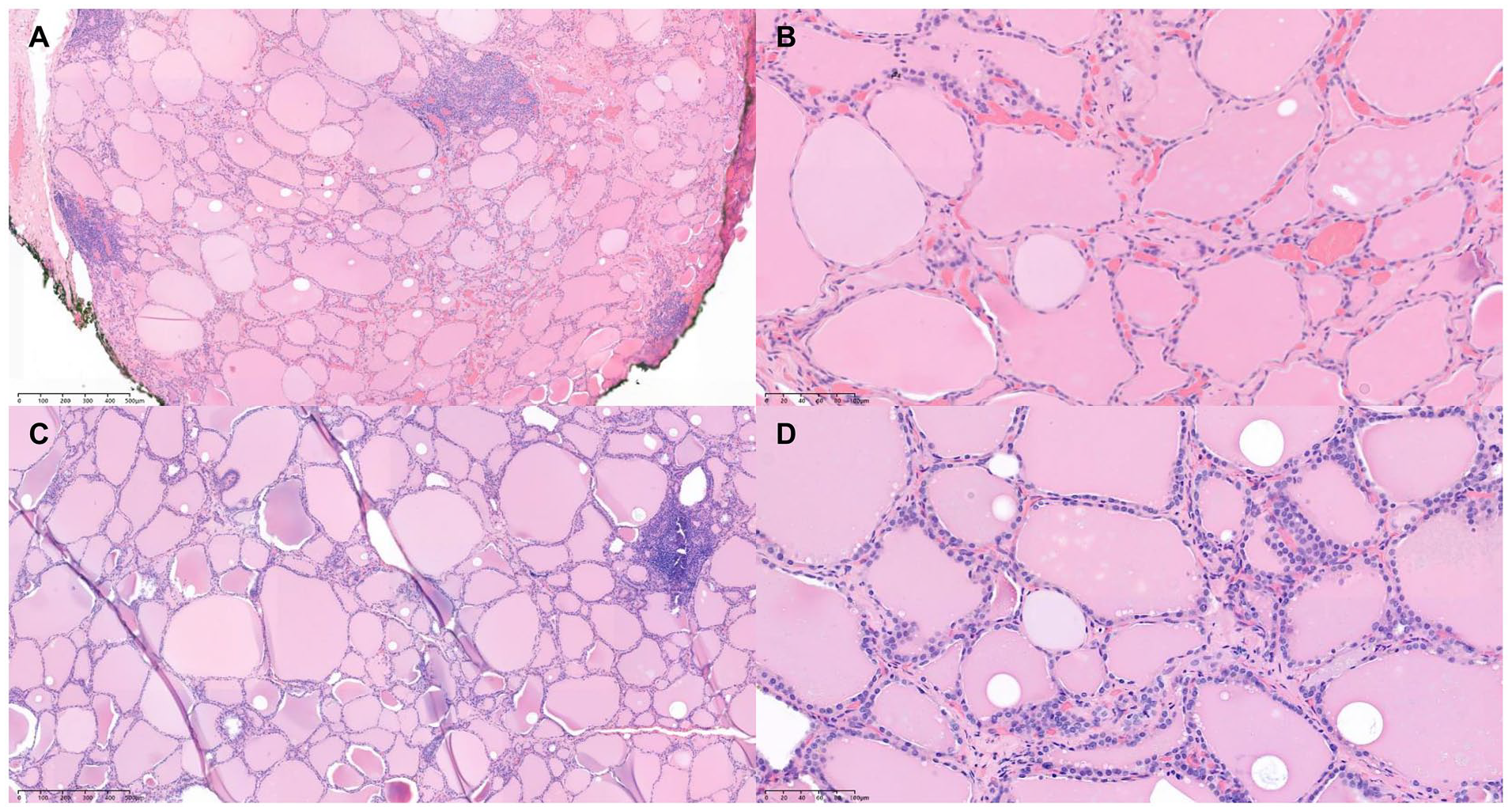
Histologic features of the thyroid. Histopathology showed 0.2 cm × 0.1 cm × 0.1 cm nodular hyperplasia with focal chronic lymphocytic thyroiditis in the left lower lobe (A—hematoxylin-eosin, original magnification ×25, B—hematoxylin-eosin, original magnification ×100). Only normal thyroid tissue was found in the rest of the thyroid gland (C—hematoxylin-eosin, original magnification ×25, D—hematoxylin-eosin, original magnification ×100).
According to the tumor, node, and metastasis staging system of the American Joint Committee on Cancer, the patient’s thyroid cancer stage was T × N1bM0. Additional treatment was discussed at a multidisciplinary meeting, and postoperative radioactive iodine therapy was recommended. A whole-body I-131 scan was performed 3 months after surgery, and no abnormalities were found, including ectopic thyroid tissue. The patient received radioactive iodine treatment and is currently undergoing follow-up observation through computed tomography (CT), ultrasound, and blood tests, including thyroglobulin. No signs of recurrence were found until 1 year after surgery.
Discussion
A thyroid cancer that is impalpable and often has a diameter of less than 1.0 cm was previously referred to as occult thyroid carcinoma (OTC). 8 OTC is classified as an incidental disease by the World Health Organization disease classification system and is referred to as occult since it is typically found during secondary surgery or at autopsy. 9 OTC was divided into 4 categories by Boucek et al. 10 Patients with benign thyroid illnesses who were incidentally diagnosed with thyroid cancer after a total thyroidectomy, or an autopsy belong in the first category. Patients belonging to the second category have thyroid papillary microcarcinomas that are unintentionally discovered during imaging procedures like ultrasounds. Patients with clinically metastatic thyroid cancer belong under the third category; in these cases, the initial tumor is not visible prior to surgery but is later discovered in histologic specimens. Patients with thyroid cancer that has spread to ectopic thyroid tissue belong under the fourth category. The fifth category of OTC was introduced by Liu et al., 11 in which a thyroid gland lesion is determined to be benign by pathologic and imaging examinations, but thyroid carcinoma metastases are found in either local lymph nodes or distant organs. Two more groups were made for the patients in this fifth category. In the first, metastatic thyroid carcinoma was found within localized lymph nodes. The second type involves the detection of metastatic thyroid cancer in the cervical lymph node or distant organ. The patient of this report belongs to the second group of the fifth category.
There are several ideas that could explain why a papillary thyroid cancer would metastasize in the absence of a primary thyroid gland tumor. The pathologist might not have meticulously examined all of the thyroid tissue samples layer by layer, following the regulations, which could have resulted in the concealment of tumor tissue. This represents the first possible explanation for the missed diagnosis. It is worth noting that lesions smaller than 3 mm could potentially escape detection. 12
Regression of the tumor is another hypothesis. In the clinical development of papillary thyroid cancer, the immune system is essential as well. It has been reported that the phagocytosis of tumor cells by macrophages is related to a higher risk of lymph node metastasis, extra-thyroid infiltration, and distant metastasis. 13 In thyroid cancer, fibrosis may therefore be a symptom of partial or total tumor regression. In a case of primary occult papillary thyroid cancer with bone metastasis, Nishikawa et al. 14 reported that the thyroid gland only showed diffuse thick fibrosis and lymphocytic infiltration; no main thyroid lesion was discovered. It has been proposed that immunity or other host resistance mechanisms may cause some cases of primary undetected papillary thyroid cancer to decrease or fade away following distant metastasis.
Additionally, ectopic thyroid tissue may develop papillary thyroid cancer. A congenital abnormality of development is an ectopic thyroid. From the foramen cecum to the anterior mediastinum, it can be found along the thyroid gland’s embryonic migration path. 15 While the thyroid itself stays normal, cancer may form in the ectopic thyroid tissue and spread to nearby lymph nodes or distant organs.
Papillary thyroid cancer presenting as isolated cervical lymphadenopathy is a rare occurrence. Despite the clinically and radiologically normal appearing thyroid gland, the appropriate next best step is total thyroidectomy once these lymph nodes are proven to be metastatic in nature. When it is followed up by a postoperative radionuclide scan and lifelong suppressive thyroxine, the outcome is usually favorable. 4
Footnotes
Acknowledgements
This work was supported by the National research Foundation Korea (NRF) grant funded by the Korea government (MSIT) (No. 2022R1F1A1071634).
Author Contributions
Conceptualization: S.H.J. and N.C. Data curation: S.H.J., J.H.P., J.K., and N.C. Writing – original draft: S.H.J. and N.C. Writing – review & editing: N.C.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Written informed consent for publication of this article was obtained from Samsung Medical Center. Written informed consent was obtained from the patient.