
Abstract
Background
The oblique brachiocephalic trunk and right common carotid artery constitute the right carotid sheath space (RCSS). The aim of this study was to detect the clinicopathologic factors associated with RCSS lymph node metastasis.
Methods
In total, 232 papillary thyroid carcinoma (PTC) patients with preoperative contrast-enhanced computed tomography scans were analyzed for associations between RCSS lymph node metastasis and clinicopathological factors.
Results
Among the 232 cases, 18 (7.76%) had suspicious RCSS lymph nodes, which was correlated with the presence of >5 metastatic lymph nodes, a larger thoracic inlet, and primary tumor size >2.15 cm. All pathologically confirmed metastatic lymph nodes were >1 cm in diameter.
Conclusions
The concept of “RCSS lymph node metastasis” was first introduced by this study. For PTC patients, a larger thoracic inlet, increased number of metastatic lymph nodes, and larger primary tumor size were related to RCSS lymph nodes, and more attention should be paid to patients who have lymph nodes >1 cm. A future prospective study will be designed to identify the potential risk factors for RCSS lymph node metastasis.
Keywords
Background
Papillary thyroid carcinoma (PTC) is the most common thyroid malignancy, accounting for 85% of all thyroid carcinomas. 1 The 10-year overall survival for most PTC patients is excellent, exceeding 90%.1,2Lymph node dissection is critical to treating PTC, as PTC patients have a high incidence of cervical lymph node metastasis (20% to 90%).1,3
The common carotid artery is the lateral border of the central-compartment lymph node dissection (CLND), and the jugular vein is the medial border of the lateral-compartment lymph node dissection (LLND). Generally, the carotid artery and jugular vein are juxtaposed; however, the space between them becomes obvious, especially on the right side, because of the oblique right brachiocephalic trunk (BCT) and common carotid artery.
The BCT is the first of the three main branches of the aortic arch. After arising from the aortic arch in the midline, it courses upward to the right, crossing the trachea, and then bifurcates posterior to the sternoclavicular joint into the right subclavian and right common carotid arteries. The oblique BCT and right common carotid artery constitute the right carotid sheath space (RCSS). In this study, we defined RCSS as the space surrounded by the sternothyroid muscle anteriorly, the lung apex and esophagus posteriorly, the intersection of the right common carotid artery and jugular vein superiorly, the suprasternal fossa and clavicle inferiorly, and the right common carotid artery and jugular vein medially and laterally, respectively (see Figure 1).
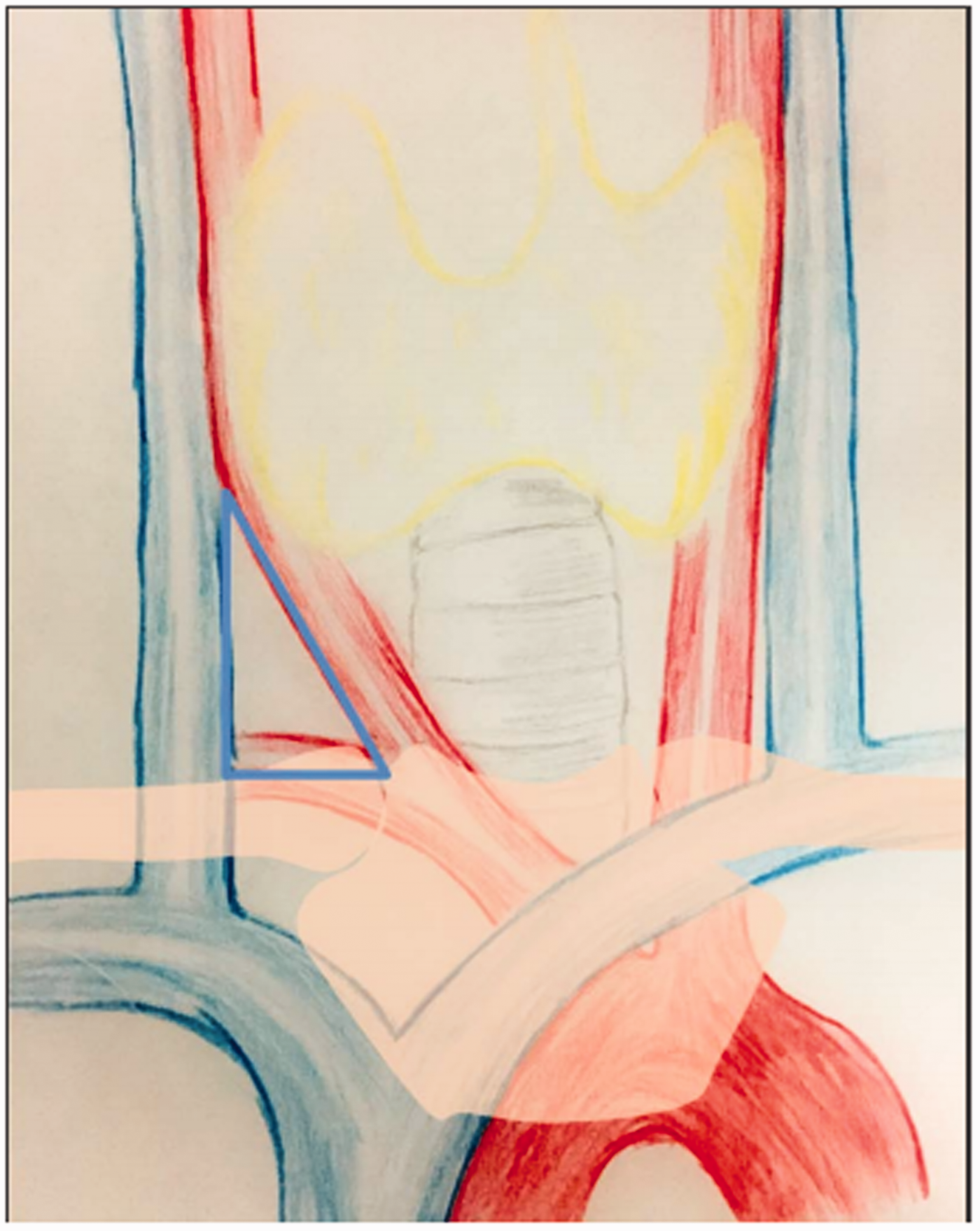
Right carotid sheath space (RCSS) coverage.
RCSS lymph node metastasis of PTC has not been fully discussed in the literature. Furthermore, there have been few reports on the significance of RCSS lymph node metastasis and its association with clinicopathological factors. Therefore, this study was designed to investigate associations between RCSS lymph node metastasis and clinicopathologic factors of PTC patients.
Materials and methods
Between July 2016 and October 2017, 792 patients underwent thyroid surgery in the Department of Head and Neck Surgery at the Sir Run Run Shaw Hospital of Zhejiang University School of Medicine (Zhejiang, China). The inclusion criteria for this study were: 1) pathologically confirmed PTC; 2) no radioactive iodine 131 (RAI) treatment, radiotherapy, or chemotherapy prior to surgery; 3) preoperative computer tomography (CT) scan with intravenous contrast; and 4) informed consent. The exclusion criteria were: 1) inadequate information; 2) revision surgery; and 3) PTC patients with poorly differentiated or undifferentiated components. Ultimately, 232 patients met the criteria and were enrolled in this study. This retrospective study was reviewed and approved by the Ethics Committee of Zhejiang University School of Medicine.
Patients with suspicious lymphadenopathy in the central or lateral neck, as detected by palpation or ultrasound scan and those with high-risk factors such as large tumor size and extrathyroid extension received enhanced CT scan of the neck and superior mediastinum. For low-risk patients, enhanced CT scans were determined by the surgeon’s clinical decision and/or the patient’s preference.
Based on CT findings, the patients were divided into two groups: RCSS suspicious and RCSS negative. Factors that might affect lymph node metastasis were investigated, including preoperative and postoperative examination results, clinical effects, and factors associated with surgery, the patient, and the disease. The American Joint Committee on Cancer (AJCC) 8th edition/TMN Classification for Differentiated Thyroid Cancer was used to determine TNM staging.
In this study, the size of the thoracic inlet was measured as the distance between the strap muscles and the trachea at the upper border of the manubrium on CT images. The anterior border of the thoracic inlet was defined as an imaginary line extending from the posterior border of the sternothyroid muscle, and the posterior border of thoracic inlet was an imaginary horizontal line extending from the anterior wall of the trachea (Figure 2).

Computed tomography (CT) scans of the thoracic inlet. (a) Anatomical markers such as sternothyroid muscle (yellow arrow) and right brachiocephalic trunk (red arrow). (b) Size of the thoracic inlet at the upper border of the manubrium level. The anterior dotted line is an imaginary line extending from the posterior border of the sternothyroid muscle. The posterior dotted line is an imaginary line extending from the anterior wall of the trachea. The distance between these two lines represented the size of thoracic inlet.
According to the Chinese Thyroid Association (CTA) guidelines, our institution performs routine prophylactic CLND, which includes Level VI lymph nodes. Therapeutic LLND is performed for patients with highly-suspicious or biopsy-proven metastatic lateral cervical lymphadenopathy. Procedures that include Levels IIa, IIb, III, IV, and Vb are performed viaa video-assisted approach.
All results are expressed as mean ±standard deviation. Differences between selected variables such as age, gender, tumor size, Hashimoto’s thyroiditis, levels VI and IV lymph node metastasis, number of metastatic lymph nodes, multifocality, extrathyroid extension, primary tumor location, size of the thoracic inlet, and RCSS suspicious lymph nodes were evaluated using the chi-squared test, Fisher’s exact test, and Student’s t-test, as appropriate. A receiver-operating characteristic (ROC) curve analysis was used to identify the cutoff point for primary tumor size and number of metastatic lymph nodes for evaluating the risk of RCSS lymph node metastasis. P<0.05 was considered statistically significant. All statistical analyses were performed using SPSS for Windows, version 16.0 (SPSS Inc., Chicago, IL, USA).
Results
After applying the inclusion and exclusion criteria, we enrolled 232 (29.29%) patients in the study, with ages ranging from 20 to 78 years (mean: 43.16 ± 12.11 years). Among the patients, 169 were female (72.8%), and 63 were male (27.2%). The primary tumor sizes ranged from 0.15 to 4.0 cm (mean: 1.15 ± 0.76 cm). Table 1summarizes the baseline characteristics of the patients enrolled in this study.
Patient characteristics (n = 232).

Data are presented as mean ± standard deviation or n (%).
RCSS, right carotid sheath space; CLND, central lymph node dissection; TT, total thyroidectomy; LLND, lateral lymph node dissection.
Overall, the rate of central-compartment lymph node (CLN) metastasis was 62.5% (145/232), and that of lateral-compartment lymph node (LLN) metastasis was 32.33% (75/232). The number of harvested CLNs was 11.70 ± 6.17 (range: 2–33). Of the 90 patients who underwent LLND, the final pathological results revealed that 75 were positive for lymph node metastasis in the lateral neck. The number of harvested LLNs was 44.16 ± 17.74 (range: 16–102). The numbers of metastatic CLNs and LLNs were 4.30 ± 3.91 (range: 1–19) and 5.19 ± 3.96 (range: 1–26), respectively.
According to the contrast-enhanced CT scans, 18 (7.76%) patients had suspicious RCSS lymph nodes, of which 6 were pathologically confirmed to have lymph node metastasis. Unexpectedly, among the remaining 12 patients, 1 had a pyramidal extension from the right thyroid gland to RCSS on CT scan (Figure 3).

Computed tomography (CT) scans of the right carotid sheath space (RCSS). (a) A normal RCSS CT image. (b) CT image of RCSS lymph node metastasis in one case. (c, d, e) CT image of pyramidal extension from the right thyroid gland to RCSS (yellow arrow).
Next, we analyzed correlations between suspicious RCSS lymph nodes and clinicopathological factors. However, no significant correlations were found between RCSS lymph nodes and age, gender, Hashimoto’s thyroiditis, level VI or level IV lymph node metastasis, multifocality, extrathyroidal extension, or primary tumor location.
Associations between size of the thoracic inlet and RCSS lymph nodes were also analyzed. The sizes of the thoracic inlet were 20.44 ± 5.30 mm (9.5–29 mm) and 16.95 ±4.66 mm (4.9–36.4 mm) in the RCSS suspicious and RCSS negative groups, respectively (data of six patients were missing because of non-standard CT scans). After Ln transformation, the variable conformed to a normal distribution, and the p-value was 0.007 (Table 2).
Univariate analysis for RCSS in 232 PTC patients.

Data are presented as mean ± standard deviation or n (%). P<0.05 was considered statistically significant.
*Information of six patients was missing because of nonstandard CT information; †the data fit a normal distribution after ln transformation.
RCSS, right carotid sheath space; LNM, lymph node metastasis.
ROC analysis was used to determine the cutoff point for the number of metastatic lymph nodes, which revealed that 5.5 was the cutoff point for suspicious RCSS lymph nodes in this cohort. The rates of RCSS lymph nodes for patients with >5 metastatic lymph nodes and ≤5 metastatic lymph nodes were 14.52% and 5.29%, respectively (p = 0.027).
There was marginal evidence suggesting an association between tumor size and suspicious RCSS lymph nodes based on these data. ROC analysis showed that 2.15 cm was the cutoff point (p = 0.043); however, there was no statistical significance when 2 cm was used as the cutoff point (p = 0.065).
Finally, our findings showed that the size of pathologically confirmed metastatic RCSS lymph nodes was, without exception, >1 cm, whereas for the remaining patients with suspicious RCSS lymph nodes, the size of dissected nodes was <1 cm. Therefore, a diameter of 1 cm was determined as the cutoff point for RCSS lymph nodes (Figure 4).

RCSS lymph node sizes (blue dotted line represents the 10-mm cutoff).
Discussion
RCSS contains a small quantity of areolar tissue connecting levels VI and IV; moreover, it communicates with the superior mediastinal lymph nodes (SMLN) inferiorly. Because of the oblique BCT and right common carotid artery, it has been easy to overlook the RCSS lymph nodes. RCSS lymph node metastasis is rare; however, in clinical practice, we found several PTC patients with metastatic RCSS lymph nodes. There are some concerns regarding the omission of metastatic RCSS lymph nodes: 1) routine ultrasound examination has low sensitivity for detecting lymph node metastasis because of interference with the chest wall bones; 2) untreated metastatic lymph nodes might increase the possibility of regional lymph node recurrence, complicate surgical procedures, and induce lift-threatening complications due to their proximity to vital structures; 3) RCSS is connected to the SMLN, so untreated metastatic lymph nodes might result in SMLN lymph node metastasis.
In this study, the number of metastatic lymph nodes was found to be associated with the presence of RCSS lymph nodes. The incidence of RCSS suspicious lymph nodes was 14.52% for patients with >5 pathologically confirmed metastatic lymph nodes and 5.29% for those with 1 to 5 pathologically metastatic lymph nodes. This result is consistent with the new modified American Thyroid Association (ATA) 2015 risk stratification system for the number of metastatic lymph nodes. As defined by the ATA Surgical Affairs Committee for thyroid cancer nodal surgery, five pathologically metastatic lymph nodes was the cutoff point between the low and intermediate risk groups. 4 RCSS lymph nodes were more common among PTC patients with high-volume lymph node metastasis because of the mechanistic downward retrograde route induced by an interruption of the lymphatic circulation and direct extension. 5
Currently, it is well recognized that the risk of recurrence in patients with N1 neck status is correlated with the size and number of metastatic lymph nodes, as well as the presence of extranodal extension of the tumor at the time of the initial treatment.6,7Consequently, a further analysis including more information such as lymph node size and extranodal extension is needed for clinical decisions.
We found that tumor size was marginally associated with RCSS lymph node metastasis. It has been indicated that tumor size is correlated with lymph node metastasis, extrathyroidal extension, recurrence, and poor overall survival.8–12Tumor size is also a risk factor in the American Joint Committee on Cancer TNM system. The small sample size was the primary reason for the marginal correlation seen in this study. More information such as molecular profiles and specific histology might facilitate clinical decisions, and this result merits further investigation.
Initially, RCSS lymph nodes was presumed to correlate with primary tumor location. However, there was no statistical significance among different locations. Of the six pathologically confirmed metastatic RCSS patients, one had left primary thyroid carcinoma. Of the remaining 12 radiologically suspicious RCSS patients, five had left primary thyroid carcinoma.
This investigation showed that regular clinicopathologic factors such as tumor size and high-volume lymph node metastasis were correlated with RCSS lymph nodes. These were tumor-related factors. In addition, we hypothesized that space-related factors might also be correlated with lymph node metastasis. The distance from the sternothyroid muscle to the trachea (Figure 2) was chosen as the indicator of the size of the thoracic inlet and was found to be correlated with RCSS lymph nodes. Lymphatic drainage of the lower thyroid follows the inferior thyroid artery. The right carotid sheath is the only pathway through which the lymphatic drainage passes from the paratracheal lymph node basin to the lateral neck. One drainage pathway is posterior to the carotid sheath and is responsible for level IV metastatic disease, whereas the other lymphatic pathways to the lateral neck can be found anterior to the carotid sheath. 13 The “Blood River” impedes the progress of lymph node metastasis. Because of the oblique BCT and right common carotid artery, RCSS became the “eyot” between the right carotid artery and the jugular vein and communicates with level VI and level IV through the areolar tissue, forming a “bridge” and “tunnel” across the “Carotid river” and under the “Jugular river,” respectively. The larger the space, the higher the “bridge” was, which increased the probability that RCSS harbored areolar tissue, ectopic thyroid, lymph nodes, and even metastatic lymph nodes.
This study had several limitations. First, there may have been a selection bias because of the non-randomized retrospective nature of the study design. Second, the number of patients with RCSS lymph node metastasis is too low to investigate potential risk factors. Third, other pathologic factors, including specific histologic subtype and molecular markers should be investigated. In the future, we would like to design a prospective study to identify potential risk factors for RCSS lymph node metastasis. Additionally, further research regarding the impact of RCSS lymph node metastasis on recurrence and survival is required to assess its significance.
RCSS lymph node metastasis is a rare phenomenon. The necessity and prognostic significance of RCSS dissection remains still unclear. Furthermore, lymph node dissection is challenging for low-volume thyroid surgeons. Insufficient exposure, unfamiliar regional anatomy, including the carotid artery, jugular vein, subclavian artery, vagus nerve, recurrent laryngeal nerve, and lung apex, make RCSS dissection difficult. Therefore, routine RCSS lymph node dissection is not recommended. Therefore, patient selection, including careful preoperative assessment, especially contrast-enhanced CT scans might be helpful for current patients. In future, we will focus on the indications and prognostic significance of RCSS dissection.
Conclusions
The concept of RCSS lymph node metastasis was first introduced in this study. RCSS lymph node metastasis might be associated with clinicopathologic factors such as the size of the thoracic inlet, number of metastatic lymph nodes, and primary tumor size. More attention should be paid to patients who have lymph nodes >1 cm. In the future, we will try to increase the patient volume and focus on the impact of metastatic RCSS lymph nodes on recurrence and survival. Meanwhile, a prospective study will be designed to determine the potential risk factors for RCSS lymph node metastasis.