
Abstract
Rhabdomyosarcoma (RMS) is a rare and aggressive cancerous tumor that arises from embryonal mesenchymal cells with skeletal muscle differentiation, and it is exceedingly rare that occurs specifically in the larynx. To date, only 22 instances of laryngeal pleomorphic RMSs have been documented in adults. Consequently, there is limited information available to assist healthcare professionals in effectively handling RMS in the larynx of adult patients. Here, we present an uncommon occurrence involving a 45-year-old man who experienced progressive hoarseness and received a diagnosis of pleomorphic RMS affecting the larynx. Pleomorphic RMS had been pathologically diagnosed after a vertical hemilaryngectomy. Following the surgical intervention, the patient underwent chemotherapy and radiation therapy. As of now, there have been no indications of tumor recurrence.
Introduction
Rhabdomyosarcoma (RMS) is classified as a type of soft tissue sarcoma, and its pathological features include aberrant myogenesis, which refers to abnormal muscle tissue formation. RMS is predominantly seen in children and adolescents, with an estimated annual occurrence of 0.44 cases per 100,000 individuals. 1 Around 30% of pediatric RMS cases involve the head and neck region, while laryngeal localization is exceptionally uncommon. 2 Pleomorphic RMS (PRMS) is an infrequent form of soft tissue sarcoma that arises from precursor cells of skeletal muscles. Unlike other subtypes of RMS that affect primarily children and adolescents, PRMS can manifest in both children and adults, although the prognosis is significantly more unfavorable for adults, characterized by elevated rates of recurrence and metastasis. 3 In this paper, we report on a patient with laryngeal RMS in an adult who presented gradually worsening hoarseness as the first symptom.
Case Presentation
A 45-year-old male was assigned to the Department of Otorhinolaryngology, Union Hospital for evaluation of a history of progressively worsening hoarseness over a period of 3 months without pain. Although underwent anti-infection and atomization inhalation of budesonide, there was no improvement in symptoms. Flexible laryngoscopy was performed, which showed a prominent mass in the middle section of the right vocal cord, characterized by a smooth surface (Figure 1C). Subsequently, a right vocal cord biopsy was performed and the immunohistochemical staining results were Desmin (+), Myogenin (partial cell +), MyoD1(−), Vimentin (+), and SMA (−), confirming the presence of PRMS.
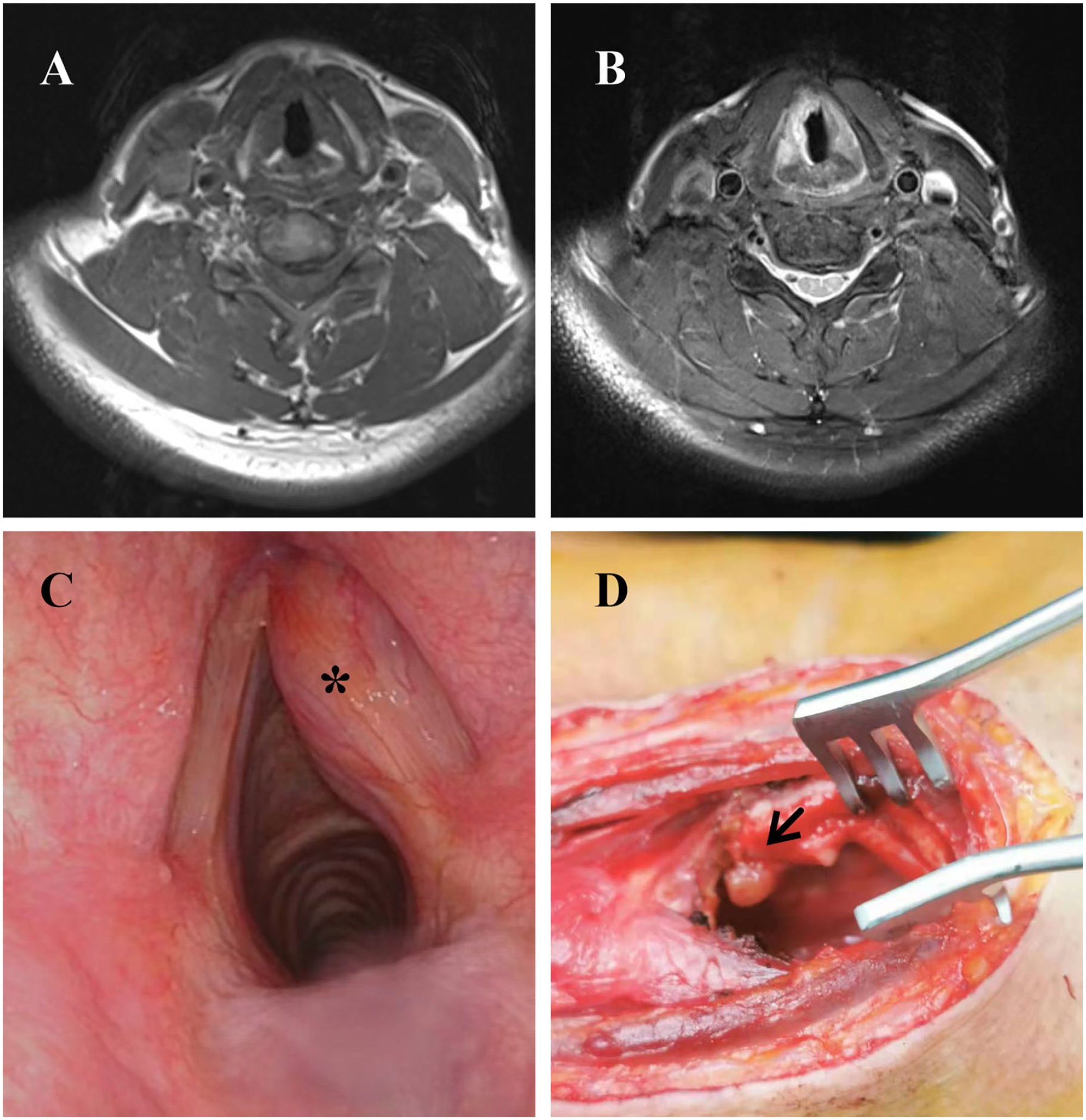
(A, B) The appearance on MRI after the biopsy showed that the right vocal cord is irregularly thickened. The mass in the vocal cord is enhanced while a similar enhancement was seen in the thyroid cartilage to that of the adjacent mass in the T2-weighted image. (C) Fibrolaryngoscopic examination shows a submucosal mass (marked *) that arises from the right vocal cord. (D) The presentation of the larynx after laryngofissure. Tumor with invasion of thyroid cartilage was labeled with an arrow.
A magnetic resonance imaging (MRI) scan of the neck revealed irregularities in the shape of the right vocal cord, with high signal intensity on the T2-weighted image signal, and the strengthening was slightly more evident, the mass caused mild narrowing of the airway (Figure 1A and B). No significant lymph node enlargement was observed in the neck.
Subsequently, the patient underwent a surgical procedure that involved a vertical hemilaryngectomy, along with a selective neck dissection. As part of the surgical intervention, a portion of the thyroid cartilage plate was removed and the laryngeal cavity was repaired to restore its functionality (Figure 1D).
On pathological examination, the present case exhibited distinct characteristics of PRMS (Figure 2A). Immunohistochemical analysis revealed positive expression of Desmin (Figure 2B) while showing negative expression of SMA, MyoD1, and Myogenin. In addition, no evidence of tumor metastasis was observed at the surgical margin or in the right zone IV lymph node.
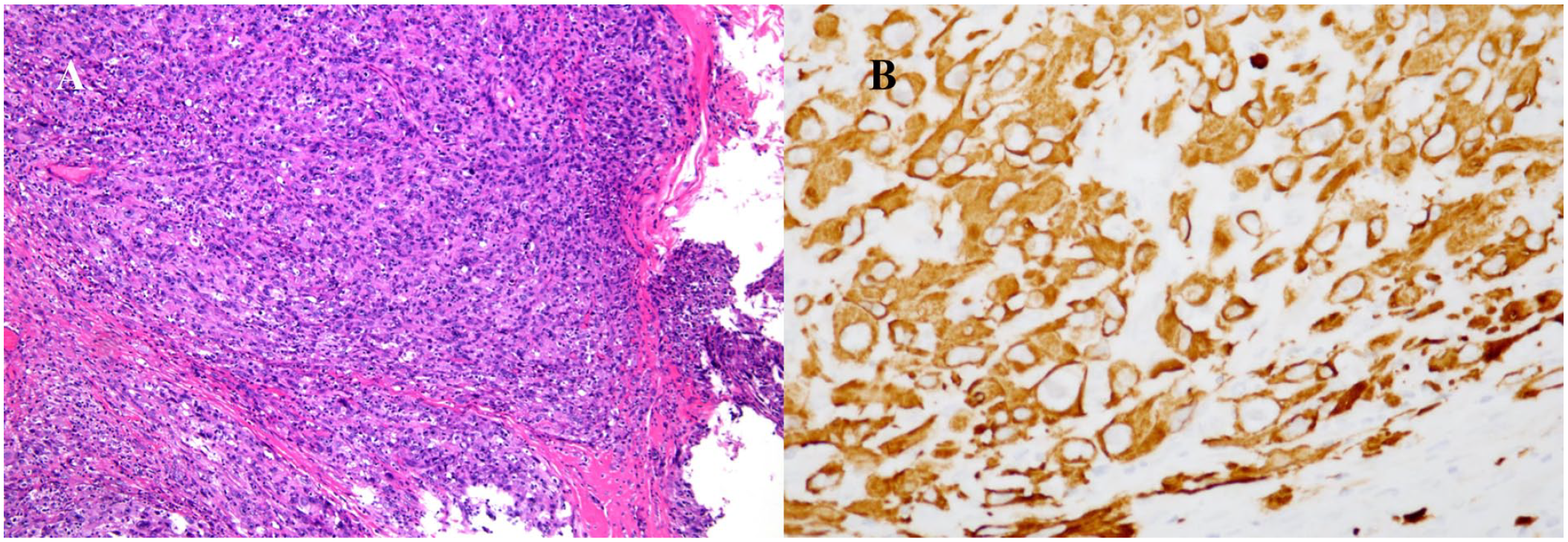
Pathological findings of laryngeal mass. (A) The histopathological section shows myxoid areas with poorly differentiated tumor cells (hematoxylin and eosin staining, ×100). (B) The immunohistochemical result shows a strong expression of desmin in neoplastic cells (×400).
Following surgery, the patient underwent adjuvant chemoradiotherapy. Chemotherapy was administered using the combination of gemcitabine and docetaxel due to the patient’s allergic reaction to Adriamycin. In addition, region-specific radiation therapy was used. Radiation doses administered were 68 Gy in 30 fractions of the gross tumor volume of the neck dissection. Following a thorough 2-year follow-up period, the patient still has persistent hoarseness after surgery, with no difficulty in swallowing or discomfort, and no signs of recurrence. The patient provided his informed consent in writing for this study.
Discussion and Conclusions
Squamous cell carcinoma comprises more than 95% of laryngeal tumors among adults, whereas laryngeal sarcomas constitute less than 1% of all malignant laryngeal tumors. 4 Most reported cases of laryngeal RMS have been observed in children, which occurred very infrequently in adults. 5 Until now, the existing literature has documented a total of 21 reported cases of laryngeal PRMS in adults. 4 Our case, which we consider to be the 22nd instance of pleomorphic RMS in the larynx among adults, 6 stands out as 1 of only 3 cases that occur in individuals under the age of 50 years.
PRMS is an exceptionally aggressive tumor known for its tendency to invade surrounding tissues locally and spread to distant sites through metastasis. The most frequently observed symptoms and signs, such as hoarseness, dyspnea, stridor, dysphagia, and a polypoid appearance, offer limited diagnostic information in identifying the condition. 7 The initial presentation of symptoms in adults with laryngeal RMS can be misleading, often resembling those of inflammatory or benign laryngeal conditions. Consequently, the diagnosis of laryngeal RMS in adults may pose a challenge, 5 requiring a high level of suspicion to accurately identify the condition. 8 At first, our case was identified as a vocal cord cyst based on its characteristic cystic appearance and the presence of a smooth mucosal overlay. Computed tomography (CT) scans were frequently chosen to obtain valuable information on the possible erosion of laryngeal cartilage or bone. 9 The use of MRI allowed for a noninvasive evaluation of tumor size, location, and the presence of nerve or vascular invasion. However, it was found that CT/MRI imaging alone was unable to differentiate RMSs from other malignant tumors of the larynx.
Significantly, the use of immunohistochemical stains and additional studies plays a crucial role in ensuring an accurate diagnosis and distinguishing between these entities. Immunohistochemically, RMS is distinguished by one or more positive muscle-specific markers, including desmin, MyoD1, muscle-specific actin, myoglobin, or myogenin.10 -12 Consequently, the definitive diagnosis is based on the use of an optical microscope and immunohistochemical techniques. 13
PRMS carries a generally unfavorable prognosis, influenced by tumor size, primary site, histological subtype, staging, pathological type, local recurrence, metastasis, and chemotherapy.14,15 While the survival rate of RMS has shown improvement over the years, increasing from 25% in 1970 to approximately 75% today, the challenges of local tumor recurrence and metastasis persist. Interestingly, laryngeal RMSs are believed to exhibit relatively less aggression compared to RMSs that occur in other locations, possibly attributed to the constraining effect of the cartilaginous boundaries of the larynx, which limit the local spread of the tumor. 5
The management approach for RMSs mainly revolves around organ-preserving surgical interventions complemented by chemotherapy and/or radiation therapy. This approach aims to minimize morbidity while effectively treating the disease. The transition to the treatment approach can be credited to the implementation of multimodal protocols introduced by the Intergroup Rhabdom-yosarcoma Study Group over several decades.16 -18 Due to the rarity of RMS in adults, there is currently no established standard chemoradiation protocol specifically tailored for them. In contemporary times, in vitro experiments to determine the sensitivity of anticancer drugs have emerged as crucial evidence in chemotherapy, serving as a significant focus in the pursuit of personalized tumor treatments.19,20
It can be observed that there were variations in the surgical approaches chosen and the subsequent use of postoperative chemotherapy and radiation therapy 6 . Most reported cases involved patients older than a certain age of 55 years, with a common follow-up duration of 8 to 30 months. Limited reports of RMSs in adults have indicated that survival rates are lower compared to children, even with the implementation of multimodal therapy. 21 The specific circumstances and characteristics of each patient should be taken into account to tailor the treatment plan accordingly. This comprehensive approach aims to optimize results by addressing the tumor through various therapeutic modalities. Given its classification as a more aggressive variant of RMS, vigilant monitoring and long-term follow-up are crucial to detect any signs of recurrence or metastasis. In our particular case, the patient is comparatively younger with only a 2-year follow-up period. Continuous close monitoring will be maintained in the future, and we are confident that our treatment approach can serve as a valuable reference for adult patients with PRMS in the larynx.
Conclusions
The case represents a rare incident of PRMS found in the larynx of a middle-aged male. RMSs often present nonspecific symptoms, and early recognition is complex. Therefore, it is crucial for otolaryngologists to maintain a high level of vigilance, allowing them to quickly suspect, confirm, and locate tumors accurately. It is imperative to emphasize the importance of early imaging studies and timely biopsies when there is suspicion of RMS, as they play a crucial role in the rapid initiation of appropriate and targeted therapy. To offer a more valuable treatment plan, it is necessary to gather more cases, conduct closer follow-up, and carefully consider the choice between conservative and radical surgical methods, as well as the need for additional radiation therapy and chemotherapy after surgery, along with its specific plan.
Footnotes
Authors’ Contributions
W-W Wang designed and supervised the work. HC drafted the manuscript. SC conceived and designed the report; HC, Z-Y Zhang, Y-Y Ding, B-H Liu, and B-B Gao diagnosed, treated, and followed the patients, and participated in the collection of clinical data. All authors have read and approved the final version of this manuscript.
Data Availability Statements
All data generated or analyzed during this research are included in this published article. Data supporting the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by research grants from the National Natural Science Foundations of China (Number: 82201301).
Ethical/Consent Statement
Not applicable.