
Abstract

Significance Statement
Inverted papillomas (IPs) are benign tumors most commonly found in the sinonasal cavity. Meanwhile, IPs involving the temporal bone are rare. Malignant transformation of this entity is even less common. Our patient developed temporal bone IP (TBIP) following sinonasal IP resection with subsequent transformation to squamous cell carcinoma (SCC). Diffusion-weighted imaging (DWI) imaging with restricted diffusion and potentially reactive dural enhancement could predict TBIP transformation to SCC. Bone erosion and (fluorodeoxyglucose) FDG avidity also characterize malignant transformation.
Case History
The patient is a 53-year-old man presenting with several months of right sided nasal obstruction. Endoscopic examination revealed a right sided nasal mass extending to the nasopharynx through the choana and then into the left posterior nasal cavity, seen on the CT and MRI examinations (Figure 1). Incomplete resection of the right nasal mass revealed a Schneiderian papilloma with widespread high-grade dysplasia. Five months later, the patient returns with progressive nasal obstruction and bilateral hearing loss and otalgia. Follow-up imaging and endoscopic examination showed disease progression into the left nasal cavity and left maxillary sinus in addition to bilateral mastoid and middle ear opacification with intracranial dural enhancement (Figure 2). The patient underwent complete resection of the sinonasal mass. Final pathology again showed Schneiderian papilloma with high-grade dysplasia without evidence of malignant transformation. Mastoid and middle ear opacification were considered secondary to Eustachian tube obstruction in the setting of recurrent sinonasal disease. Asymmetric frontal dural enhancement was considered a nonspecific finding and the etiology was not determined.
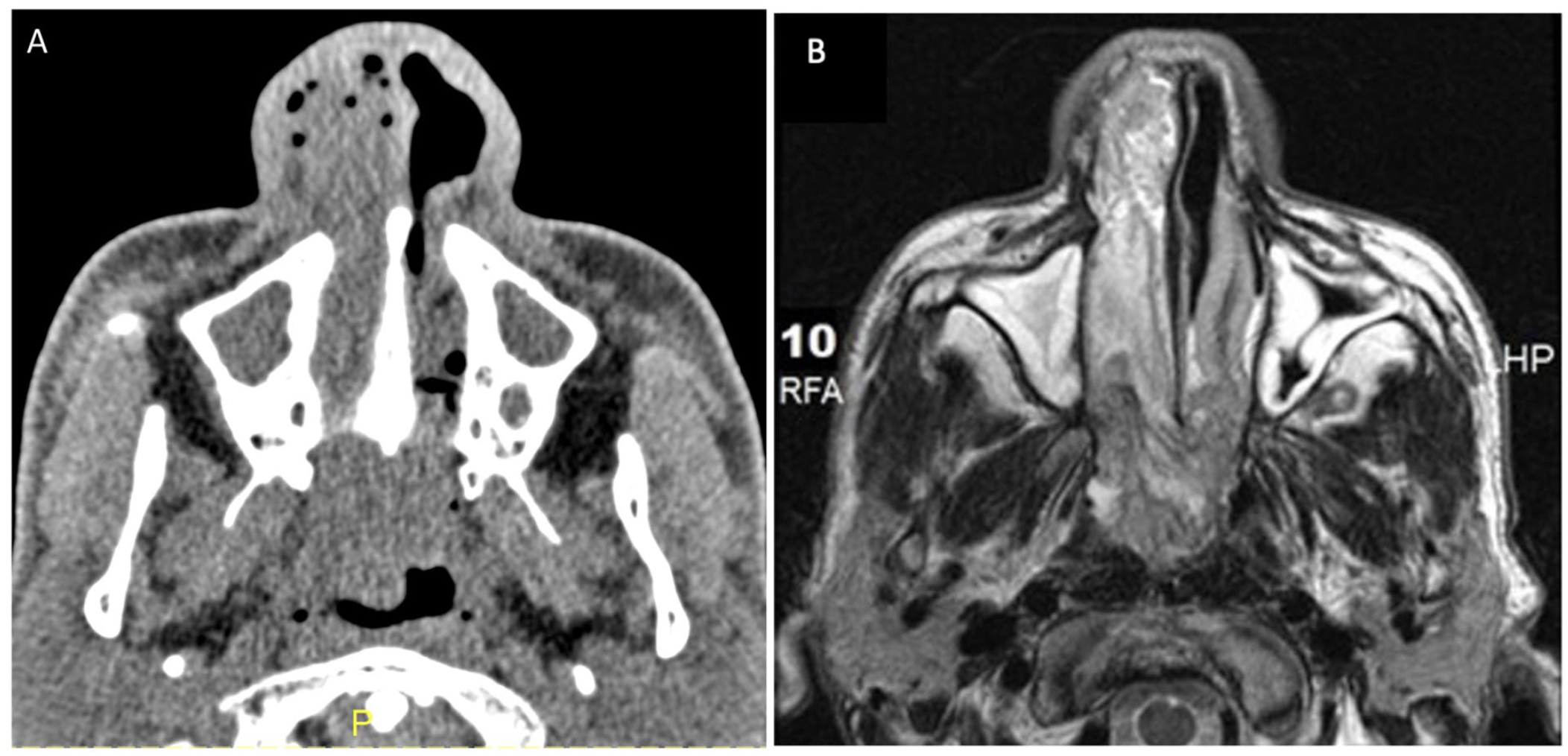
(A) CT of the sinus in soft tissue window shows a right nasal mass extending through the choana into the nasopharynx and into the posterior left nasal cavity. (B) In axial T2-weighted MRI, the nasal mass has a cerebriform appearance which is heterogenous to hypointense.
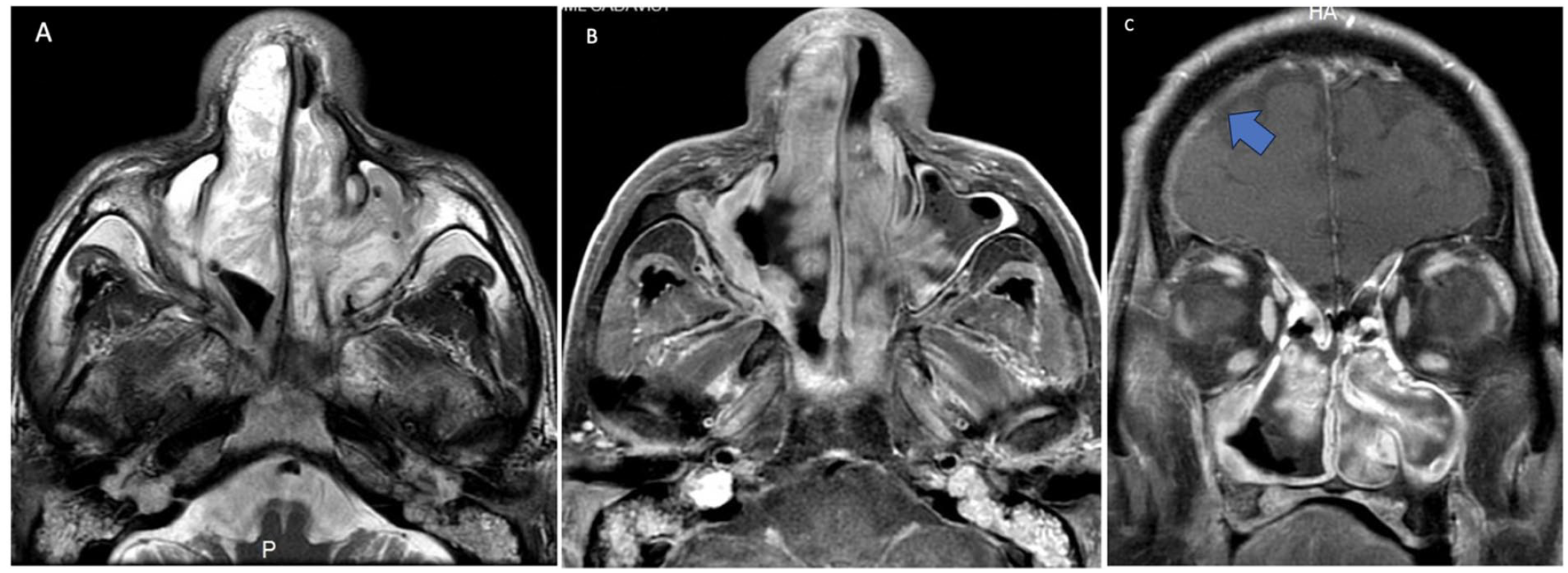
MRI of the paranasal sinuses (A) (B) Axial T2-weighted and post-contrast fat-suppressed axial T1-weighted images show incomplete resection of the right nasal mass with residual disease. Progression of disease into the left nasal cavity and left maxillary sinus is seen. Bilateral mastoid fluid collections from Eustachian tube obstruction are also seen. (C) Post-contrast coronal T1-weighted image shows a nonspecific right frontal dural enhancement (blue arrow), the nature not determined.
Six months later, the patient returned with progressive otalgia. Temporal bone CT (Figure 3a) showed progressive bilateral mastoid, external auditory canal, and tympanic cavity opacification, along with significant septal and cortical destruction of the mastoid air cells. Tegmen mastoideum and tympani erosion were also observed. MRI (Figure 3b) showed the lesion at the level of the Eustachian tube with restricted diffusion. The soft tissue at the level of the Eustachian tube also showed FDG avidity with maximum standardized uptake values (SUV) of 12.1 on the right and 6.5 on the left (Figure 3c). The remaining soft tissue opacifying the mastoid and middle ear showed no restricted diffusion and lacked FDG avidity. Soft tissue excisional biopsy at the level of the left Eustachian tube, tympanic cavity, and tegmen also showed Schneiderian papilloma with high grade dysplasia without any malignant transformation.
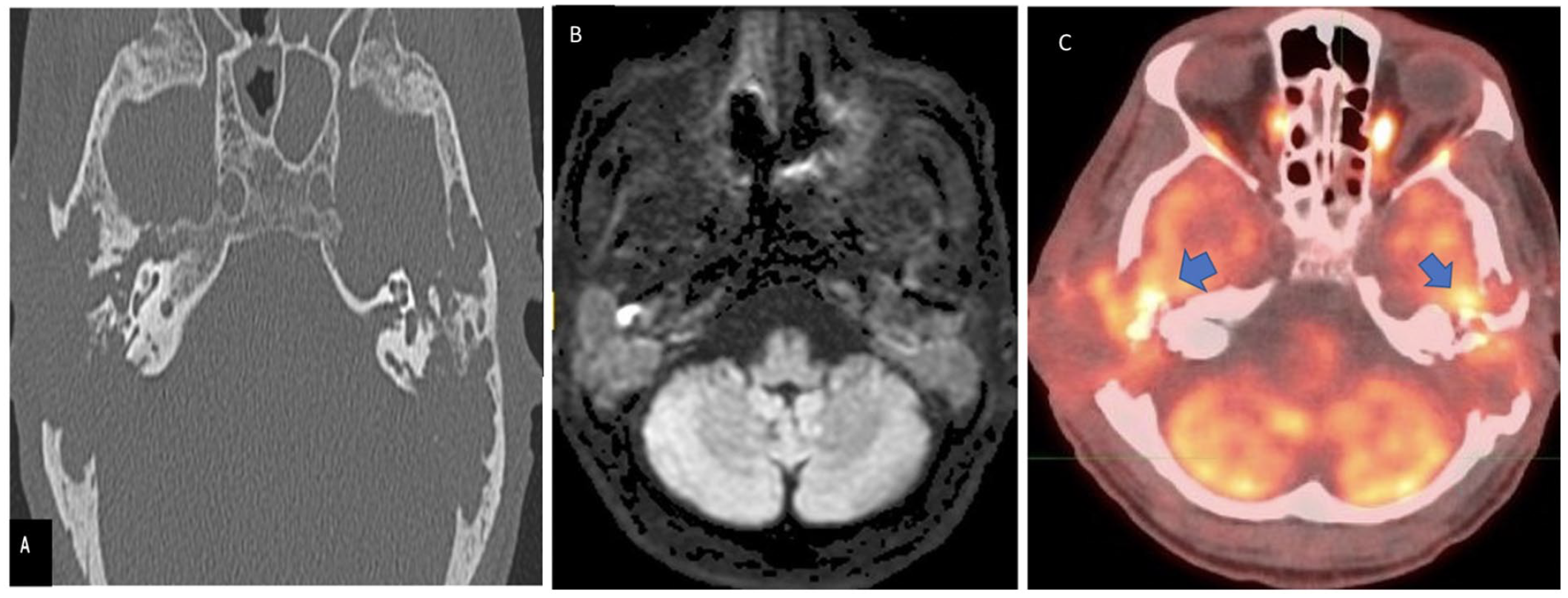
(A) CT of the temporal bone shows bone destruction associated with progression of bilateral mastoid and middle ear soft tissue mass extending to the mastoid and tegmen tympani bilaterally. (B) MRI axial DWI shows restricted diffusion at the site of converted squamous cell carcinoma. (C) PET/CT shows metabolic activity with SUV of 12.1 on the right and SUV of 6.5 on the left.
Discussion
IPs are locally aggressive tumors that show local recurrence if incompletely resected.1,2 IPs outside the sinonasal tract are rare, particularly in the temporal bone. Temporal bone IP could be primary or secondary, presenting after sinonasal tract IP. Secondary TBIP is more aggressive with increasing predilection for severe invasive carcinoma than primary TBIP. 2 Review of the literature identified 13 cases of malignant transformation of secondary TBIP to SCC. We present another case of malignant transformation of secondary TBIP to SCC following treatment of sinonasal tract IP.2–13
Thirteen cases showed mastoid, middle ear, and external auditory canal opacification and involvement. All external auditory canal lesions exhibited a polypoid appearance and Eustachian tube involvement. Eustachian tube direct extension supports the proposed route of development of IP of the temporal bone.
Of the 7 cases with MRI imaging, all showed enhancement of the presumed portion of the IP that converted to SCC. Enhancement alone cannot predict malignant transformation, since IP without malignant transformation can also show enhancement. Enhancement and complete opacification of the mastoid, middle ear, and external auditory systems are less common predictors of malignant transformation of TBIP since these findings could be seen with IP and Eustachian tube obstruction.
In our case, preoperative biopsy revealed restricted diffusion and low apparent diffusion coefficient (ADC) value (1.31 × 10−3) at the Eustachian tube level, confirming SCC transformation of the temporal bone IP. Low ADC values and restricted diffusion has also been described in SCC transformation of IP of the sinonasal tract. Malignant tumors exhibit increased cellularity, leading to increased water diffusion restriction and lower ADC values. 14
On MRI, IP of the sinonasal tract shows a convoluted cerebriform pattern (CCP) with bands of hypo- and hyperintensity on T2-weighted imaging and post-contrast enhancement.15,16 In IP of the temporal bone, this feature is difficult to replicate and appreciate. In the sinonasal tract loss of CCP appearance of the lesion could be used as an indicator for malignant transformation of the IP. 17 Again, this feature cannot be used in temporal bone MRI imaging since the CCP pattern and loss of CCP may not be detected in the temporal bone imaging.
In our case, the SUV of the IP SCC at the right Eustachian tube level was 12.1 versus the SUV value of the left mastoid antrum and Eustachian tube of 6.5, which were also biopsied and showed to be IP without malignant transformation. PET/CT with elevated SUV help to diagnose malignant transformation of IP. 7 In a systematic review, Long showed IP SCC patients had higher SUV max values than patients with IP alone. Our case confirms these findings.
Footnotes
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, Alex Silberzweig, upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases.
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the Mount Sinai Health System’s approved protocols.
Statement of Informed Consent
Informed consent for patient information to be published in this article was not obtained because the institution in which this research was performed does not require informed consent for retrospective case reports.