
Abstract
Immunoglobulin G4-related disease (IgG4-RD) is a rare and complicated clinical disease entity newly identified in recent years. It is a chronic inflammatory disease mediated by the immune system that can affect various organs throughout the body, such as the pancreas, salivary gland (submandibular gland, parotid gland, and sublingual gland), lacrimal gland, and thyroid gland. In rare cases, it involves sinuses and orbits. We describe a 44-year-old patient who was hospitalized with distension and pain in her right eye. The lesions included the nasal sinus and orbit. IgG4-RD was diagnosed after surgery and the patient was treated without complications. This case report helps to provide clinicians with additional information to assist in the diagnosis of the disease.
Introduction
Immunoglobulin G4-related disease (IgG4-RD) is a fibrous inflammatory state with active tubular lesions at multiple sites and therefore is considered to be a systemic disease. 1 It has histopathological characteristics (dense lymphoplasmic cell distention, layered swelling, and obliterative phlebitis) and frequently increases serum IgG4 concentration. 2 The diagnosis of IgG4-RD depends on a combination of histopathological characteristics and increased IgG4-positiveplasma cell counts. The critical histopathological features are dense lymphoplasmacytic infiltration, a storiform pattern of fibrosis, and obliterative phlebitis. IgG4-RD can affect a variety of organs throughout the body, such as the pancreas, salivary glands (submandibular, parotid, and sublingual), lacrimal and thyroid glands, and rarely the sinuses and orbits. 3 Immunosuppressive therapy is considered an effective first-line therapy for IgG4-RD. 1 Here, we report a case of cumulative sinus and orbital IgG4-RD, and the study of this case may provide additional information for the diagnosis of IgG4-RD.
Case Report
A 44-year-old woman was admitted to the hospital with “right-sided eye swelling for 6 months.” She had been diagnosed with “right ocular keratitis” at an external hospital. Physical examination of the nasal septum, nasal floor, bilateral middle and lower turbinates, and lateral wall of the nasal cavity revealed no obvious abnormalities and the mucous membrane was still smooth (Figure 1a). Visio oculus dexter (VOD): 1.0, intraocular pressure (IOP): 15 mm Hg, visio oculus sinister (VOS): 1.0, and IOP: 16.5 mm Hg. Limited downward rotation of the right eye, pressure pain (+). Rotation of the left eye was not constrained and there was no pressure pain. Diplopia on downward gaze of both eyes. Laboratory tests revealed normal liver and kidney function; blood count: 10.85 × 109 L; absolute neutrophil count: 7.97 × 109 L; lymphocyte percentage: 18.3%; absolute monocyte count: 0.81 × 109 L; platelets: 453.0 × 109 L; and the rest were in the normal reference range. Sinus CT showed an irregular mass-like hyperdense shadow with unclear border in the right nasal cavity—sieve sinus—maxillary sinus (MS)—orbit with inhomogeneous enhancement on enhancement scan. Thickening of the mucosa of the septal sinus. Swollen bony destruction of the nasal septum with patchy hyperdense shadowing; a little bony destruction of the frontal process of the left maxilla (Figure 1b and c). The preoperative examinations were completed with an endoscopic excision of the sinus lesion, and the ophthalmologist completed the excision of the orbital lesion. Postoperative pathology revealed severe chronic inflammation of mucosal tissues with fibrous tissue hyperplasia, lymphocytic and plasma cell infiltration, and formation of lymphoid follicles in the lamina propria (Figure 2a). Immunohistochemical findings: Lambda (partial plasma cell +), Immunoglobulin G (IgG; positive cell count ~200 cells/HPF), Immunoglobulin G4 (IgG4; positive cell count ~50 cells/HPF), with an IgG4/IgG-positive ratio of approximately 40% (Figure 2b). Regimen: Rituximab (2 doses) 1000 mg intravenous injection for 2 weeks; concomitantly with the first dose of rituximab prednisone acetate tablets 50 mg orally in the morning until the second dose of rituximab is administered, after which the dose is reduced to 25 mg and then reduced to 5 mg weekly until discontinuation. Postoperative outpatient nasal endoscopic review showed smooth mucosa in the sinuses with no obvious masses (Figure 2c–e).
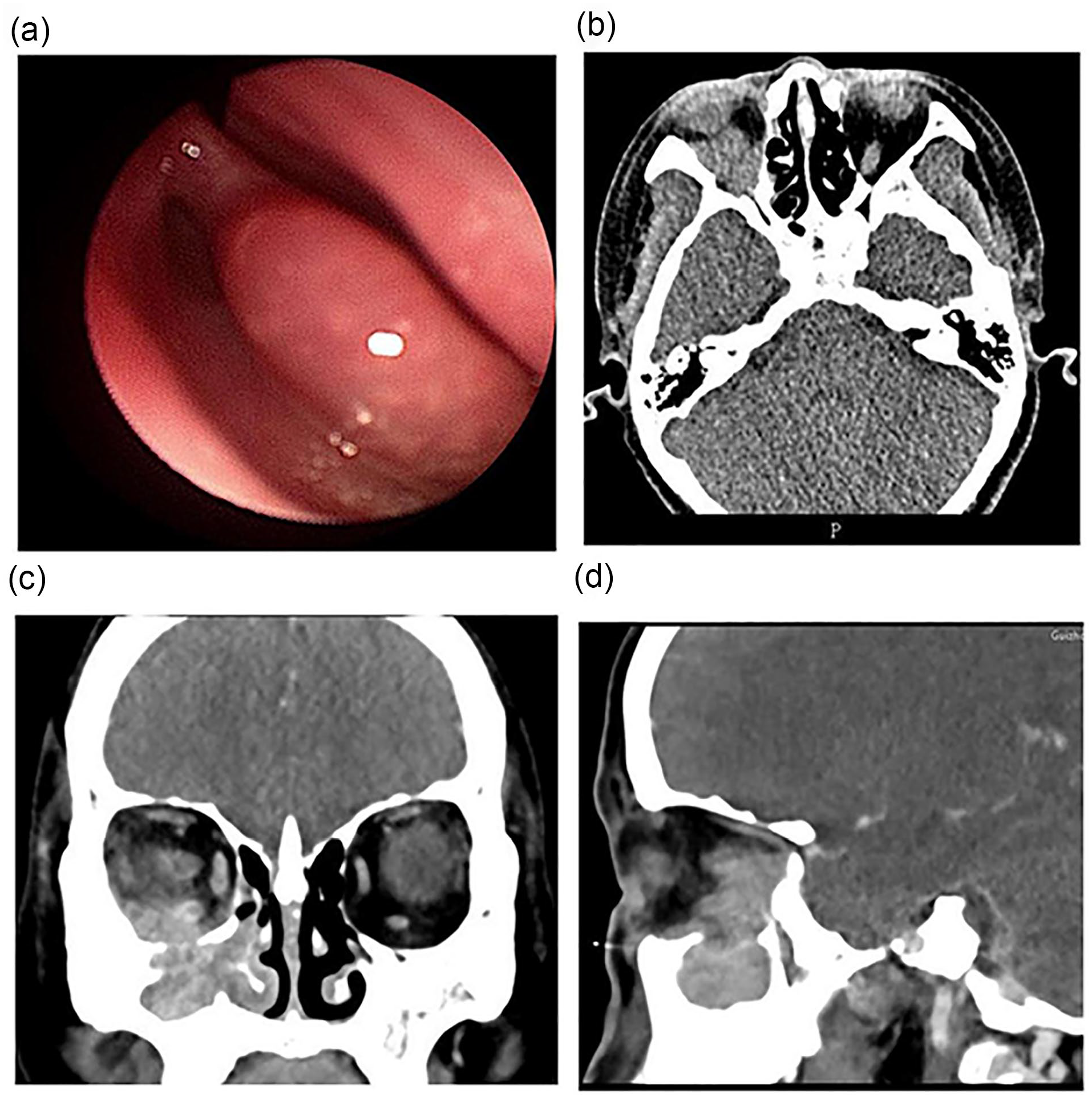
(a) Nasal endoscopy showing no obvious masses in the nasal cavity. (b) CT Horizontal position of sinuses. (c) CT coronal position of the sinuses. (d) CT sagittal position of the sinuses. Sinus CT showing the extent of the lesion spreading to the sinuses and orbit in 3 dimensions.
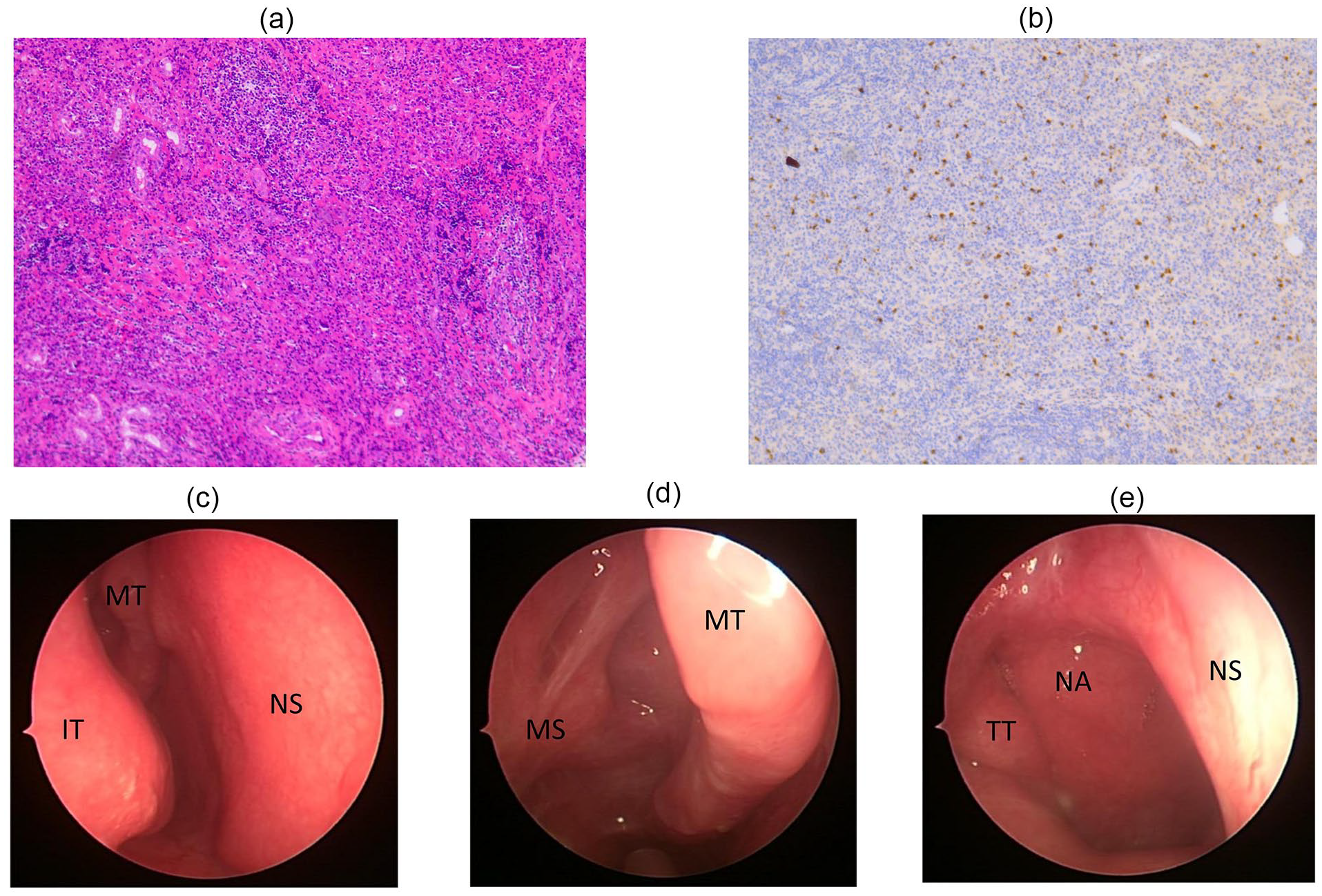
(a) Hematoxylin and eosin staining of lesion tissue showing severe chronic inflammation of the mucosal tissue with fibrous tissue hyperplasia, high lymphocytic and plasma cell infiltration, and formation of lymphoid follicles in the lamina propria. (b) Immunohistochemical staining of lesion tissue showing IgG4-positive plasma cells (positive cell count ~50 cells/HPF). Postoperative follow-up nasal endoscopy showing no recurrence of swelling in the nasal cavity. (c, d, and e). NA, nasopharynx; NS, nasal septum; MT, middle turbinate; IT, inferior turbinate; TT, torus tubarius; MS, maxillary sinus.
Discussion
IgG4-related disease, also known as IgG4 multiorgan lymphoproliferative syndrome, was proposed by Kamisawa in 2003 4 as a chronic, systemic, immune-mediated, and auto-inflammatory disease that generally presents as a tumor-like lesion with elevated serum IgG4 concentrations (but not always) 5 and is characterized histopathologically by massive lymphocytic and plasma cell infiltration, matricial fibrosis, and occlusive phlebitis. Numerous organ systems are involved with IgG4-RD, including the pancreas, biliary tree, salivary glands, periorbital tissues, kidneys, lungs, lymph nodes, meninges, aorta, breast, prostate, thyroid, pericardium and skin. 6 After the pancreatobiliary system, the head and neck is the next most common site for involvement by IgG4-related disease. 7 This disease predominantly affects people over 50 years of age. Patients will typically present with a nonpainful mass lesion in the head and neck region. 8 IgG4-related nasal sinus lesions are part of the IgG4 systemic disease group and are rare in the clinical setting, coexisting with or isolated from other sites. Due to the low prevalence of nasal IgG4-related disease, there is no fixed name specifically for the disease.
The most common symptoms of IgG4-related nasal sinus lesions are a runny nose, nasal congestion, facial swelling, rhinorrhea, loss of smell, and dull headache. Some patients with minor nasal symptoms can be seen in other departments due to significant symptoms elsewhere. 9 The lack of specificity in serum immunological tests, histopathological changes, imaging and clinical manifestations has prompted clinicians to use intranasal glucocorticoids based on their clinical manifestations, and the effectiveness of hormonal therapy has led to the possibility of misdiagnosis as chronic rhinitis, chronic rhinosinusitis, or nasal tumors, or even underdiagnosis. The patient was previously mistaken for sinusitis and received nasal spray hormone therapy without formal examination and treatment. The symptoms recurred and with time the patient developed a feeling of ocular swelling, followed by a refinement of sinus CT: an irregular mass-like hyperdense shadow with unclear borders was seen in the right nasal cavity—septal sinus—MS—orbit, and the enhancement scan was inhomogeneous. The right inferior orbital wall, the inner wall of the MS, the sieve plate, and the bone of the right inferior turbinate were severely damaged. The preoperative evaluation concluded that the lesion was unlikely to be malignant and that the IgG4-related lesion was more likely.
IgG4-related disease often has nonspecific imaging manifestations and is difficult to differentiate from other diseases with imaging alone. 10 Most lesions demonstrated nonspecific homogenous CT attenuation, diffuse enhancement, and isointense/low T1 signal intensity 11 . At T2-weighted MR imaging, they may have relatively low signal intensity owing to their increased cellularity and amount of fibrosis. 10 IgG4-RD is a recently defined multisystem disease. Though radiological findings are not part of the diagnostic criteria for IgG4-RD, there are imaging features that prompt or support the diagnosis. 12 The authors suggest that a general approach in the imaging workup of clinically suspected IgG4-RD should include computed tomography or magnetic resonance imaging of the primary site of suspected disease followed by biopsy if possible, to confirm the diagnosis. 13 Furthermore, the involved site and disease distribution in each case should be assessed generally before treatment. Fluorine-18 labeled fluorodeoxyglucose positron emission tomography (18FDG-PET) is a very sensitive method to identify involved lesions, and thus it is strongly recommended. 14
Hisanori Umehara proposed the diagnostic criteria for IgG4-RD. The diagnostic criteria are 15 : (1) diffuse or mass enlargement in 1 or more organs; (2) elevated serum IgG4 levels (>1.35 g/L); (3) lymphocyte and IgG4-positive plasma cell infiltration on pathological histological examination (IgG4-positive plasma cells > 40% and >10 IgG4-positive plasma cells/high magnification view) with characteristic tissue fibrosis and sclerosis. Definite diagnosis: (1) + (2) + (3); likely diagnosis: (1) + (3); and probable diagnosis: (1) + (2). Although the diagnosis of pathologically related nasal sinus lesions related to IgG4 may be more reliable, in this case there were no serum IgG4 test results, and it has been suggested that serum IgG4 levels may not be a reliable diagnostic indicator of IgG4-RD. 16 Almost a third of the patients with IgG4-RD diagnosed according to histopathological criteria had normal serum IgG4 concentrations at the time of diagnosis. However, IgG4 showed elevated levels in the mucosal tissue of this lesion, and the diagnosis of IgG4-RD was substantially established by a comprehensive analysis of the associated circumstances in this patient. 17 However, diagnostic criteria for IgG4-associated nasal sinus lesions should be based on the above-mentioned diagnostic criteria and should not be generalized. Physicians need to further explore and study more clinical data and experience on IgG4-related nasal sinus lesions.
Similar to Inflammatory pseudotumor (IPT), characteristic histopathological manifestations of IgG4-RD (dense lymphoplasmacytic infiltrate, storiform fibrosis, and obliterative phlebitis). 18 Although there are no uniform norms for the treatment of IgG4-related nasal sinus lesions, the current treatment regimen evolved from the treatment of IPT and other organ immune-related diseases (pancreas, salivary glands, etc.). IgG4-RD is sensitive to glucocorticoid and immunosuppressive therapy.19,20 For nasal-sinus IgG4-RD, the main treatment is oral glucocorticoid therapy with a starting dose of 30 to 40 mg/d and a gradual reduction of the hormone after improvement. 21 The hormone dose is gradually reduced, Rituximab injection was given at the same time, and the prognosis was significant. 22 Surgical treatment provides at least a sample for histopathological analysis; IgG4-associated nasal sinus lesions are benign lesions and surgery is an important treatment tool, especially in patients with extensive and sclerotic lesions. However, the initial dose of prednisone acetate used in this case was 50 mg, mainly due to the extent of the patient’s orbital lesion, and then was reduced. Two infusions of rituximab were administered simultaneously, the patient recovered well. Without any clinical intervention, IgG4-RD can progress progressively to a broad range of tissues and organs, and eventually the patient will die due to organ failure. In this case, there is no loss of visual acuity and no impairment of eye movements in both eyes.
In conclusion, IgG4-related nasal sinus lesions are a rare disease with limited clinical recognition. The possibility of IgG4-associated nasal disease should be considered in patients with diffuse swelling of the nasal mucosa or in some cases of “refractory sinusitis.” Peripheral blood tests for IgG4 and IgG levels can be used as a preliminary screening test, but a definitive diagnosis is based on histopathological examination. Although the utility of positron emission tomography–computed tomography (PET-CT) in the diagnosis of IgG4-RD has been supported, sinonasal IgG4-RD is often limited to the head and neck, and therefore, it should not be used for the initial diagnostic workup. PET-CT can be considered a response. 23 Therefore, the diagnosis and treatment of this disease depend on careful analysis and intensive communication between clinicians and pathologists. Interventions should be adapted according to the clinical presentation of the patient and the progression of the disease, and early diagnosis and effective intervention are of the essence in the control and treatment of IgG4-RD.
Footnotes
Acknowledgements
Not applicable.
Author Contributions
All the authors contributed to the conception and design of the study, material preparation, data collection, and analysis. C.C., Q.L., C.F., and S.G. writing – original draft preparation, C.C., Q.L., and C.F. All authors participated in the review and editing of the previous versions of the article. All authors have read and approved the final article.
Data Availability
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Guiyang Science and Technology Bureau Project (grant number. 2019-2-16).
Ethical Statements
This study was conducted in accordance with the principles of the Declaration of Helsinki. Written consent has been obtained from the patients to publish all relevant data.