
Abstract
This report presents 2 illustrative cases of sinonasal pathologies masquerading as ocular diseases: one of a 43-year-old male with a frontoethmoidal mucocele resulting from multiple prior surgeries for juvenile nasopharyngeal angiofibroma, and the other of a 72-year-old male with sinonasal diffuse large B-cell lymphoma, both presenting primarily with ocular symptoms including diplopia and visual disturbance. Through these cases, we highlight the importance of considering sinonasal pathologies in the differential diagnosis of patients presenting with ocular symptoms and discuss the diagnostic and therapeutic approaches that enabled effective disease management. Multidisciplinary collaboration involving otolaryngologists, ophthalmologists, radiologists, and oncologists was critical in achieving accurate diagnoses and successful management of these sinonasal diseases with ocular involvement.
Introduction
Sinonasal pathologies manifesting with ocular symptoms can present the clinician with diagnostic challenges. These conditions can mimic primary ocular diseases, complicating the clinical picture and delaying appropriate treatment. Mucoceles are cystic lesions resulting from the obstruction of sinus ostia, leading to the accumulation of mucus that can expand and erode surrounding structures, including the orbit. 1 Sinonasal malignancies, although less common, can also extend into the orbital cavity and lead to various ocular manifestations. 2 This report presents 2 illustrative cases of sinonasal pathologies masquerading as ocular disease: one of a frontoethmoidal mucocele and the other of a sinonasal lymphoma, both presenting primarily with ocular symptoms including diplopia and visual disturbance. Through these cases, we aim to highlight the importance of considering sinonasal pathologies in the differential diagnosis of ocular symptoms and to discuss the diagnostic and therapeutic approaches that enabled effective disease management. These cases highlight the critical role of a multidisciplinary approach involving otolaryngologists, ophthalmologists, radiologists, and oncologists in the accurate diagnosis and management of sinonasal diseases with ocular involvement.
Case Reports
Case Presentation 1
A 43-year-old male with a history of juvenile angiofibroma (JNA) that was treated with multiple embolization procedures, open craniofacial resections, and radiation therapy in the distant past presented to the otolaryngology and ophthalmology clinics with worsening headaches, vision changes of the left eye, and bilateral epiphora. He reported that over the last year, he has had increasing diplopia and noticeable hypoglobus of the left eye. Of note, the patient reported that he has had to hold up his chin and turn his head to the left to maintain single vision. He also began noticing some gradually increasing swelling of his left forehead around this time. The patient denied any epistaxis, rhinorrhea, nasal congestion, or other nasal complaints.
In-office nasal endoscopy revealed postsurgical changes from prior JNA excisions as well as a large, bulging, polypoid mass emanating from the left supraorbital area. The bilateral frontal sinus outflow tracts appeared to be scarred and obliterated. Evaluation in the ophthalmology clinic revealed limited extraocular eye movement of the left eye in all directions with normal visual acuity. Computed tomography (CT) and magnetic resonance imaging (MRI) of his sinuses with and without contrast were performed, and a massive frontoethmoidal mucocele filling the bilateral frontal sinuses with associated bony expansion as well as extension into the left orbit with inferior displacement of the globe was found (Figure 1).
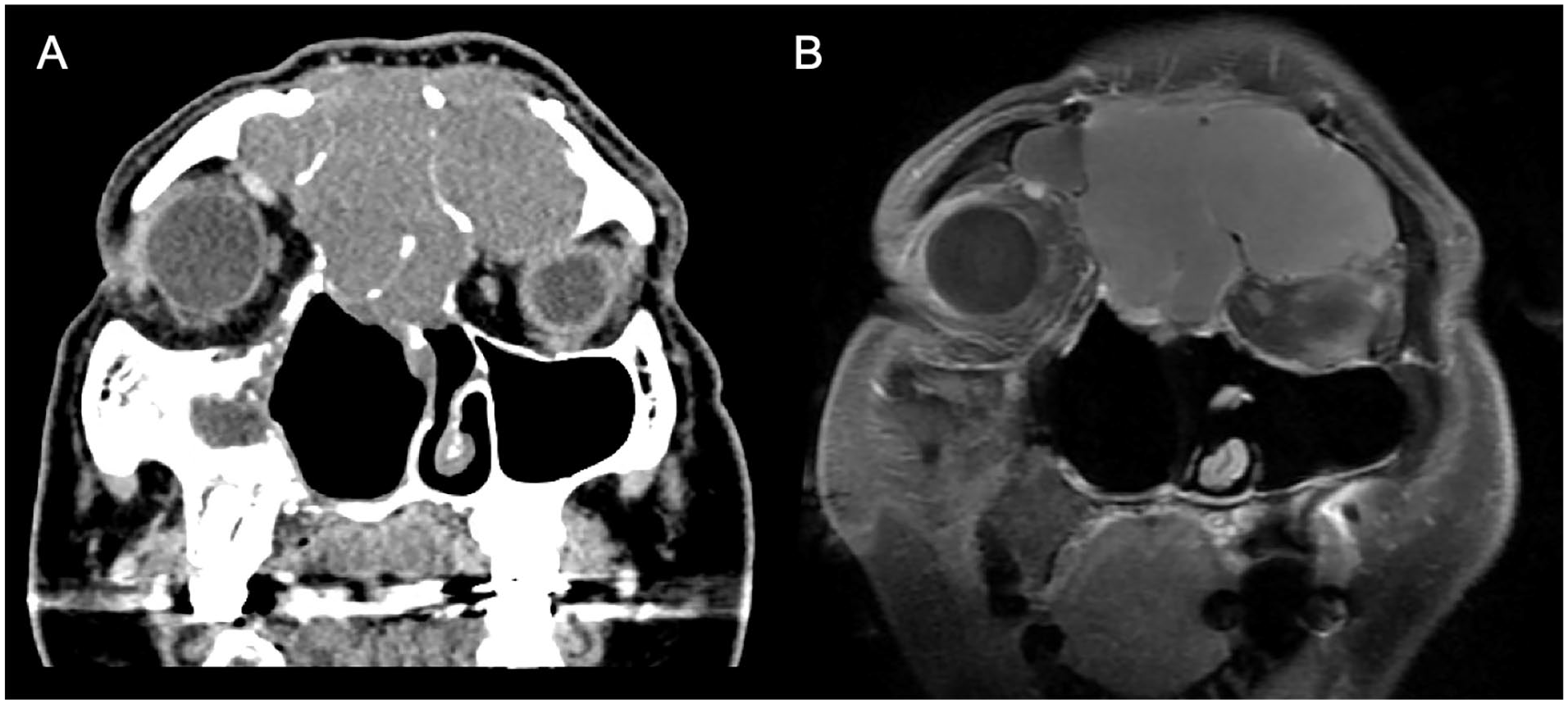
Coronal CT without contrast (A) and MRI T1 post-contrast (B) of the sinuses showing a large frontoethmoidal mucocele involving both frontal sinuses and compressing the left orbit. CT, computed tomography; MRI, magnetic resonance imaging.
The patient subsequently went to the operating room for bilateral image-guided endoscopic sinus surgery (ESS). A Draf III procedure was performed to create a common frontal sinus cavity for accessing and completely resecting the mucocele. 3 The patient was admitted to the hospital for overnight observation and discharged on postoperative day 1. At his 6-month follow-up visit, the patient endorsed normalization of his vision without further diplopia or headaches.
Case Presentation 2
A 72-year-old male presented to the otolaryngology clinic with an 8-month history of right-sided epiphora, diplopia, a slowly growing orbital mass, bilateral nasal obstruction, and purulent rhinorrhea. The patient underwent multiple rounds of antibiotics prescribed at community emergency departments without improvement of his symptoms. A CT scan of his orbits without contrast was performed by an outside provider revealing bilateral nasal masses with involvement of the right orbit, prompting referral to our clinic.
On evaluation, the patient was noted to have a large and firm orbital mass arising from the right lower lid completely obstructing the eye. In-office endoscopy revealed bilateral nasal cavity masses completely obstructing view of the paranasal sinuses with surrounding purulent drainage, suggesting superimposed sinusitis. The patient was also evaluated in the ophthalmology clinic, where he was found to have limited extraocular eye movement in all directions and severe vision loss in the right eye (20/200), while the left eye had normal vision with intact extraocular eye movements. CT and MRI of the sinuses and orbit with and without contrast were performed, revealing a 5.1-cm mass centered in the right medial extraconal orbital fat with intraconal extension that was circumferentially enveloping the right globe, as well as a similar appearing 6.5-cm left nasal cavity mass extending into the medial left orbital extraconal fat without evidence of globe contour abnormality (Figure 2). Of note, the masses were found to be abutting the cribriform plate without intracranial involvement. An MRI with contrast of the neck was also performed, showing prominent subcentimeter cervical lymph nodes in levels 1A, 1B, and 2B of the left neck.
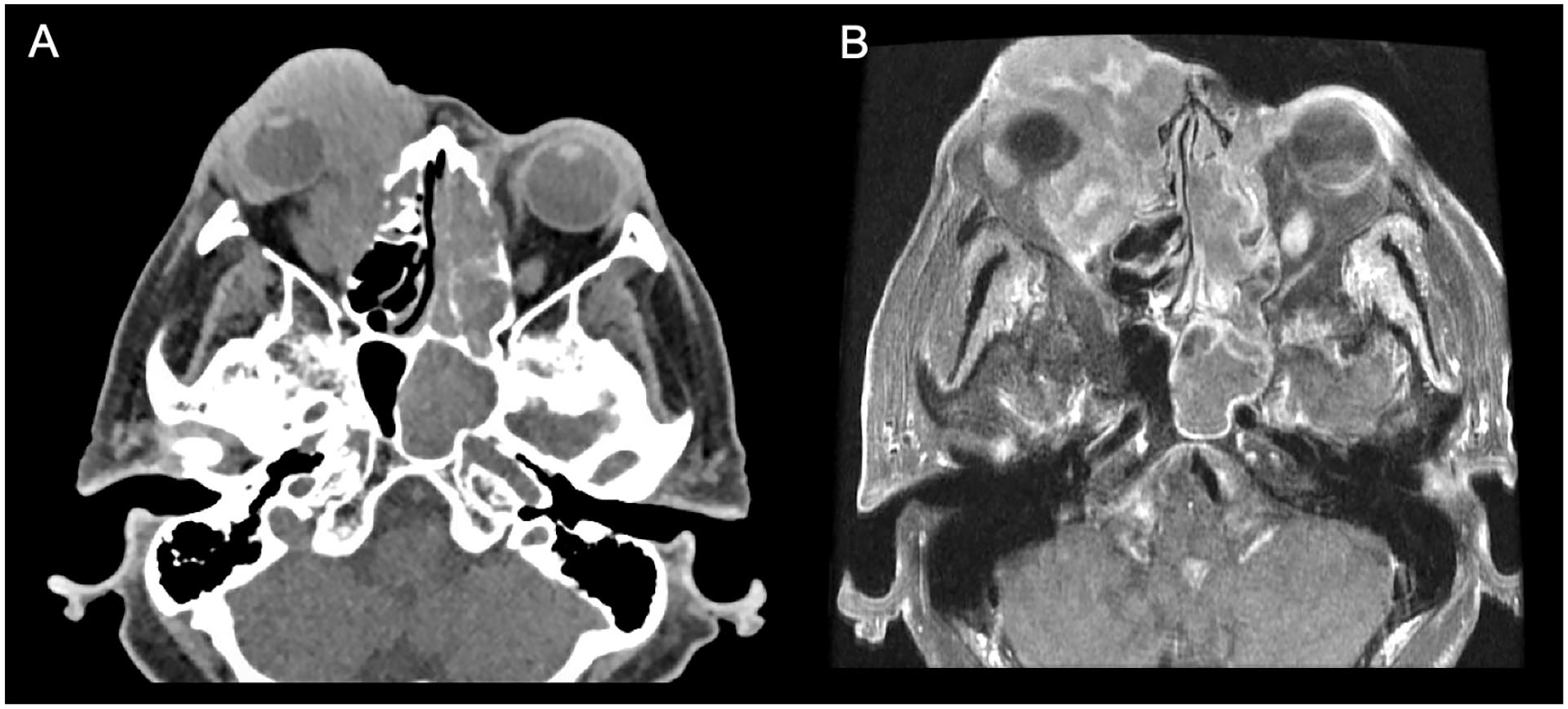
Axial CT without contrast (A) and MRI T1 post-contrast (B) of the sinuses showing bilateral soft tissue masses involving the sinonasal cavities and right orbit with circumferential encasement of the right globe. CT, computed tomography; MRI, magnetic resonance imaging.
Due to history, physical exam, and imaging findings concerning for malignancy, the patient was urgently booked for the operating room with the primary intent of decompressing the right orbit and performing mass biopsy to obtain a diagnosis. Intraoperative frozen histologic sections of the sinonasal and orbital masses were suspicious for lymphoma; therefore, the ophthalmology team was consulted intraoperatively and advised that open resection of the right orbital mass was not indicated. The patient subsequently underwent bilateral image-guided ESS, including right-sided endoscopic medial maxillectomy, dacryocystorhinostomy, and orbital decompression with removal of the lamina papyracea and the medial aspect of the orbital floor, in order to restore the normal sinus drainage pathways, debulk the tumor in anticipation of future chemotherapy treatments, decompress the right eye, and relieve the patient’s epiphora. Final pathology confirmed the diagnosis of diffuse large b-cell lymphoma (DLBCL), germinal center b-cell like subtype. Postoperative metastatic work-up, including whole body positron emission tomography computed tomography (PET-CT), was negative.
The patient’s oncologic treatment consisted of a 5-day cycle of inpatient chemotherapy: rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP), followed by additional outpatient chemotherapy. At his 2-month follow-up visit, the patient had complete resolution of his orbital mass without further diplopia or epiphora (Figure 3).

Preoperative (A) and 2 months post-chemotherapy treatment (B) images highlighting resolution of the right orbital mass.
Discussion
The presentation of ocular symptoms in patients with sinonasal pathologies, including paranasal sinus mucoceles and malignancies, can pose significant diagnostic and therapeutic challenges. Many sinonasal and primary orbital diseases can manifest with similar ophthalmic signs, including proptosis, diplopia, and visual disturbances, necessitating a thorough and systematic approach when forming a differential diagnosis, performing a precise diagnostic work-up, and administering targeted treatment. These cases also highlight the importance of involving a multidisciplinary team early to ensure timely diagnosis and management of these conditions before complications arise.
When patients present with ocular symptoms, the differential diagnosis should encompass a wide range of conditions, including infectious, inflammatory, and neoplastic arising from the orbit or sinonasal cavity. Importantly, because of the similarity in presentation between primary orbital pathologies and sinonasal diseases with secondary orbital manifestations, the clinician must have a high index of suspicion for sinonasal etiologies even in patients presenting without nasal complaints. The initial symptoms of the patient with the frontoethmoidal mucocele led to considerations of orbital abscess, JNA recurrence, and orbital lymphangioma as the underlying cause, while in the case of the patient diagnosed with DLBCL, the initial differential diagnosis included an infected dacryocystocele, primary orbital tumor, orbital metastasis, and sinonasal carcinoma, among other considerations. Frontoethmoidal mucoceles should be suspected in patients presenting with ocular symptoms who report a history of facial trauma or previous sinus or craniofacial surgeries, as these can lead to sinus ostium obstruction, mucus retention, and gradual expansion. By contrast, sinonasal lymphoma is a rarer disease entity accounting for just 11% of sinonasal malignancies, and should be suspected in patients presenting with soft tissue masses seen externally or on endoscopy, particularly in the presence of systemic signs and symptoms including unexplained weight loss, night sweats, fevers and fatigue.4,5
Beyond the history and physical examination, accurate diagnosis of these conditions relies on diagnostic imaging and histopathological confirmation. CT and MRI of the sinuses and/or orbit performed with contrast are the gold standard for providing detailed information on the extent and nature of orbital and sinonasal lesions. In the case of the frontoethmoidal mucocele, CT imaging demonstrated characteristic findings of a cystic expansile lesion causing bony expansion and orbital extension. 5 MRI provided additional soft tissue detail, confirming the benign nature of the lesion. For the DLBCL case, CT and MRI revealed diffusely infiltrating lesions extending along the walls of sinonasal cavity in addition to discrete soft tissue masses, consistent with malignancy. 6
For any sinonasal or orbital malignancy, definitive diagnosis is achieved through histopathological analysis. For tumors without highly characteristic morphological features on histology, immunohistochemistry (IHC) is frequently employed to identify specific cell markers to aid with diagnosis, and in cases of lymphoma, flow cytometry is utilized for immunophenotyping of cells, cell population analysis, and detection of clonality, which are all essential for identifying the specific subtype of lymphoma. 7 In our second case, the lesion was identified as germinal center b-cell DLBCL through flow cytometry showing an abnormal B-cell population consisting of large cells with an immunophenotype positive for CD45, CD19, CD20, and surface Ig Kappa, in addition to characteristic IHC findings and genetic abnormalities identified on fluorescence in situ hybridization. 8 Importantly, once a diagnosis of sinonasal malignancy is obtained, it is critical to perform additional radiologic imaging to evaluate for distant metastases; this work-up typically involves obtaining CT scans of the chest and abdomen or whole-body PET-CT. 6
Treatment strategies for frontoethmoidal mucoceles and DLBCL are markedly different due to their distinct pathophysiologies. Frontal sinus mucoceles are primarily managed surgically, with the goal of decompression, excision, and drainage. ESS is the preferred approach, offering a minimally invasive route to effectively address the mucocele and alleviate symptoms. 9 In the presented case, endoscopic resection of the mucocele resulted in eventual resolution of ocular symptoms and a satisfactory patient outcome. However, it should be noted that these lesions may recur in a significant minority of patients after surgery. For example, a retrospective study by Eren et al found that 13% of patients with frontoethmoidal mucoceles experienced postoperative recurrences occurring at a mean interval of 2 years after ESS. 10
Conversely, the management of DLBCL involves systemic therapy, with surgery typically only playing a role in obtaining a tissue diagnosis, and in our case, for immediate orbital decompression. The primary goal of surgery in our case was to decompress the eye, which required pursuing a medial maxillectomy and dacryocystorhinostomy. DLBCL was also not high on our differential diagnosis prior to surgery. The standard treatment regimen for DLBCL includes R-CHOP. 6 This regimen is effective in achieving complete response in a majority of patients with sinonasal B-cell lymphomas. 11 The patient in this case responded well to R-CHOP, with significant improvement in symptoms and reduction of the tumor mass, although his follow-up period is still very short at just 2 months. Overall survival for patients diagnosed with sinonasal DLBCL is relatively low, ranging from 6 to 10 years after diagnosis.12,13 A recent study by Lehrich et al evaluating the national cancer database found that among 2073 patients with sinonasal DLBCL treated with standard of care systemic therapies, the overall survival at 1, 2, 5, and 10 years was 87.5%, 81.7%, 69.9%, and 51.2%, respectively. 13
Long-term follow-up is essential for patients with sinonasal mucoceles and DLBCL to monitor for disease recurrence and manage any potential complications. For paranasal sinus mucoceles, proper follow-up involves periodic endoscopic examinations and CT of the sinuses every 1 to 2 years to assess for mucocele recurrence. For patients with DLBCL, follow-up should include regular clinical assessments and imaging according to evidence-based clinical practice guidelines to monitor for disease recurrence and initiate early treatment for recurrent disease. 14
Conclusion
Healthcare providers should consider sinonasal pathologies in the differential diagnosis of patients presenting with ocular symptoms. Accurate diagnosis through clinical evaluation, imaging and histopathology, appropriate surgical or systemic treatment, and vigilant follow-up are all crucial for optimizing patient outcomes. These cases of a frontoethmoidal mucocele and sinonasal DLBCL illustrate the complexities involved in managing sinonasal diseases presenting with ocular symptoms and the necessity of collaborative, multidisciplinary care to achieve successful results.
Footnotes
Submission Statement
This article is original and has not been submitted elsewhere in part or whole.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.