
Abstract
Objective:
Posterior neck masses are a relatively poorly characterized entity. The authors attempt to further characterize the anatomy and pathology of the posterior neck by way of a combined single-institution retrospective chart review and systematic review of the literature.
Methods:
A single-institution retrospective chart review was undertaken for all patients undergoing excision of a posterior neck mass between January 1, 2012, and January 1, 2017. A systematic review of the Medline, Embase, Web of Science, and Cochrane database was undertaken in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines in search of case reports and series describing posterior neck masses.
Results:
A total of 28 patients who underwent excision of a posterior neck mass were encountered during the retrospective chart review. All pathologies were benign, the most prevalent of which was lipoma (22/28, 79%). A total of 19 articles describing a collective 36 posterior neck masses were encountered during the systematic review. Lipomas were the most common pathology (15/36, 42%). All but one of the masses reported were benign (35/36, 97%).
Conclusions:
Patients presenting with posterior neck masses can be reassured of a low risk of malignancy. The majority of posterior neck masses can be appropriately evaluated via physical examination and ultrasound.
Keywords
Introduction
Diagnostic algorithms for neck masses have been described for decades. 1 -3 Anterior, lateral, and posterior triangle neck masses are known to represent diverse pathologies, including both benign and malignant disease. Mass lesions of the posterior neck, a relatively less anatomically complex region, have not been commented upon to the same extent as lesions of other areas of the neck. In this article, the authors perform a retrospective review of their own experience with posterior neck masses as well as a systematic review of prior publications to further characterize mass lesions of the posterior neck.
Methods
The authors define the posterior neck as the soft tissue anatomy bordered by the occiput superiorly, the first thoracic vertebrae inferiorly and the trapezius muscle laterally (Figure 1). As defined, the posterior neck is a region that does not contain the great vessels, cranial nerves, or major lymphatics and consists predominantly of subcutaneous fat and skeletal muscle. Mass lesions presenting within or superficial to the trapezius, splenius, and paraspinal muscles are included in these boundaries. Masses of the posterior triangle of the neck, delineated by the posterior border of the sternocleidomastoid muscle, anterior border of the trapezius, and the clavicle are not included in this definition.

Posterior neck schematic.
This retrospective chart review was undertaken at the University of California, San Diego (UCSD). The study was deemed appropriate for an exemption by the UCSD institutional review board given the retrospective nature of the study and the use of preexisting, deidentified patient data. Using the electronic medical record, the operative logs of the entire otolaryngology—head and neck surgery department were surveyed for cases performed between January 1, 2012, and January 1, 2017 (5 years). Any case involving the excision of a posterior neck mass as defined by the aforementioned anatomic boundaries was eligible for inclusion with the exception of cases involving cutaneous pathologies (ie, basal cell carcinoma, melanoma, actinic keratoses, etc). Basic demographic data, preoperative workups, operative details, surgical pathology, and postoperative outcomes were assessed.
The systematic review was performed in accordance with the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (www.prisma-statement.org), 4 which are a standardized and widely utilized criterion for performing effective systematic reviews. Using the search terms, “posterior neck mass OR suboccipital neck mass” a targeted query of the Medline, Embase, Web of Science, and Cochrane databases was performed. The date of the final search was February 11, 2018, and any publication encountered prior to this date was considered eligible. Prospective and retrospective studies were considered. Case reports and case series were eligible for inclusion. No exclusions were made based on patient age. Articles describing cutaneous lesions or masses not confined to the posterior neck were excluded. Articles not available in the English language were excluded. Pathologic data and basic demographic data were assessed and compiled. Statistical analysis was performed in the R statistical software environment and Microsoft Excel (Seattle, Washington).
Results
Retrospective Chart Review
A total of 28 patients undergoing surgical excision of a posterior neck mass were found during the retrospective chart review (Table 1). The patient age range was 38 to 69 with a mean of 54. Fifteen (54%) of the patients were male. For the 18 patients who could estimate how long the mass had been present prior to the clinical evaluation, an average duration of 4.4 years was calculated. Twenty-four (86%) patients had a primary symptom of a painless mass. Two (7%) patients had a history of a previously excised posterior neck mass. Ten (36%) of the 28 patients underwent evaluation with ultrasound (US), while 11 (39%) underwent a computed tomography or magnetic resonance imaging (MRI). Five (18%) patients underwent multiple imaging modalities and 12 (43%) underwent no imaging study prior to surgery. Only 2 (7%) patients underwent a preoperative biopsy. Twenty-two (79%) patients underwent surgery with a general anesthetic, while 6 (21%) underwent monitored anesthesia care. Eight patients had a drain placed at the time of surgery. All specimens were found to be benign on final histopathology. Twenty-two (79%) specimens returned as lipomas, 3 (11%) as epidermal inclusion cysts, 2 (7%) as fibromas, and 1 (4%) returned as a benign lymph node. Averaged across all patients, the mean lesion size was calculated at 5.0 cm × 3.6 cm × 2.8 cm. Patients were typically evaluated in clinic 1 week following surgery, and there were no surgical complications encountered.
Posterior Neck Mass Retrospective Chart Review Summary Data.
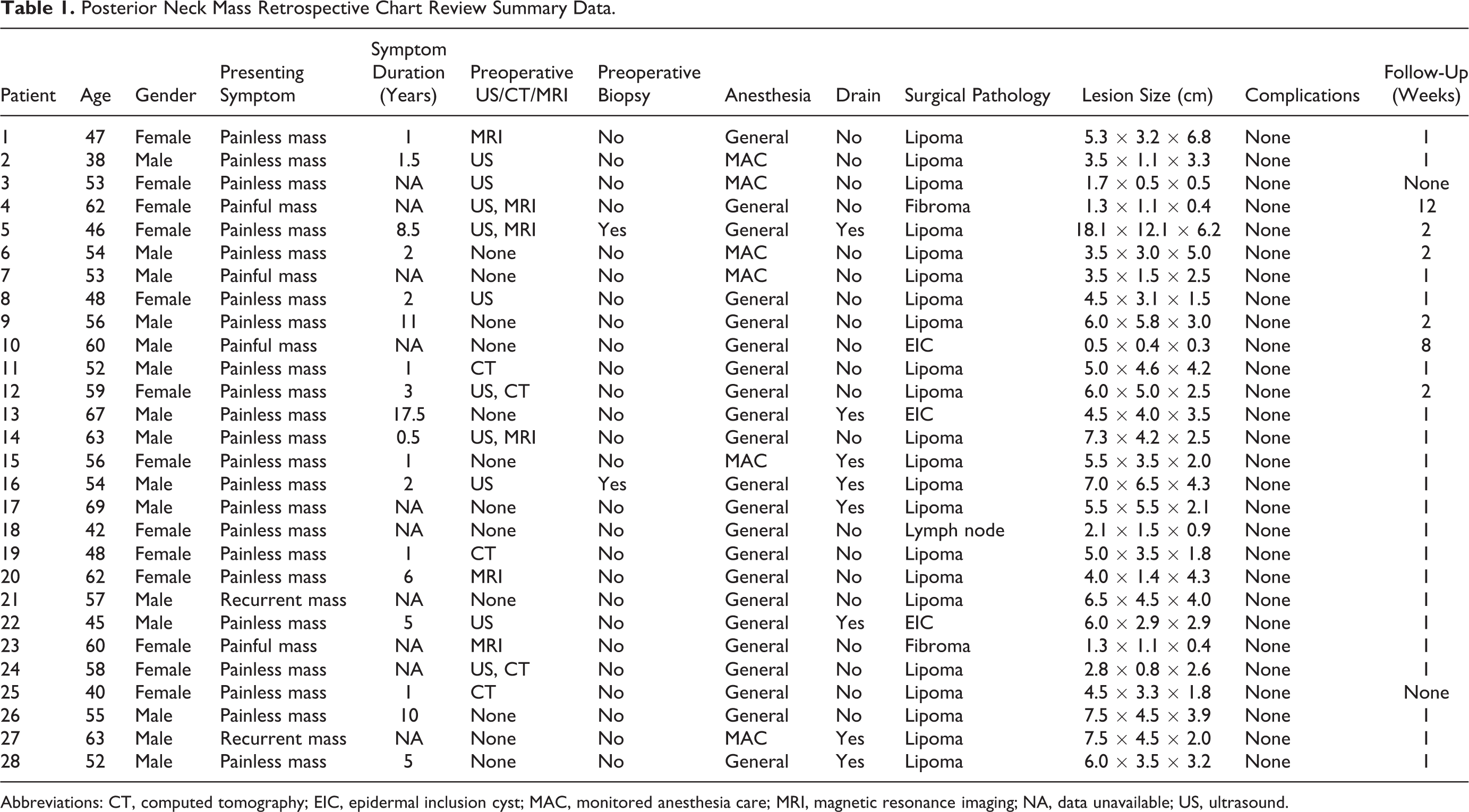
Abbreviations: CT, computed tomography; EIC, epidermal inclusion cyst; MAC, monitored anesthesia care; MRI, magnetic resonance imaging; NA, data unavailable; US, ultrasound.
Systematic Review Results
The systematic review schema used to identify eligible articles is shown in Figure 2. Of the 19 articles ultimately included, 36 total patients with posterior neck masses were represented. 5 -23 The collective pathologies were as follows: 15 lipomas, 10 nuchal fibromas, 3 schwannomas, 2 epidermal inclusion cysts, 1 lipoblastoma, 1 hemangioma, 1 leiomyoma, 1 lymphangioma, 1 benign meningioma, and 1 malignant meningioma (Figure 3). As such, 35 (97%) of the 36 reported masses represented benign disease. Of the 24 patients with detailed demographic data, there were 14 males and 10 females with a mean age of 35 years. Three patients were younger than the age of 18; a 13-month-old female (lipoblastoma), 11 a 9-year-old female (meningioma), 16 and a 13-year-old male (leiomyoma). 5
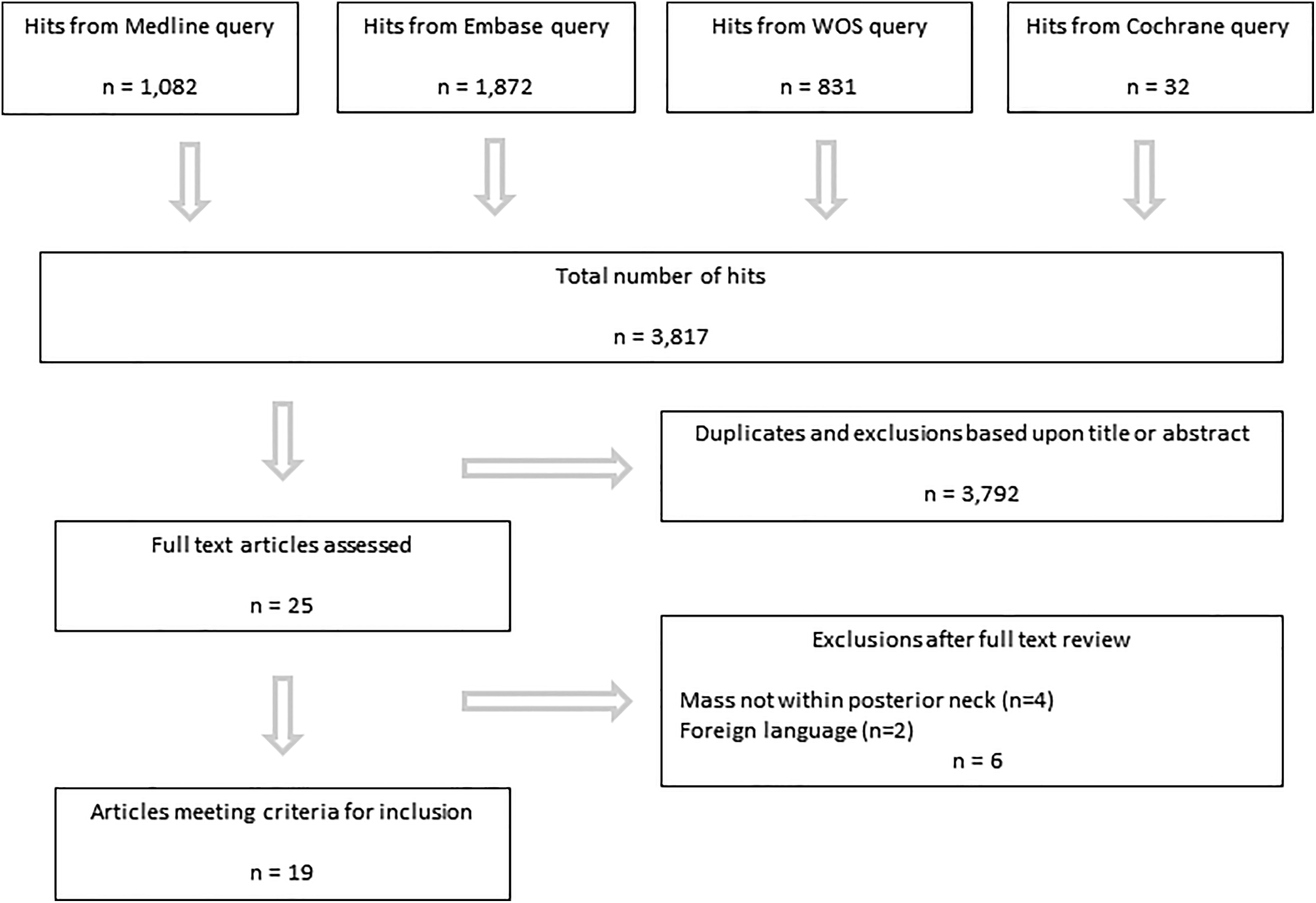
Systematic review flowchart.
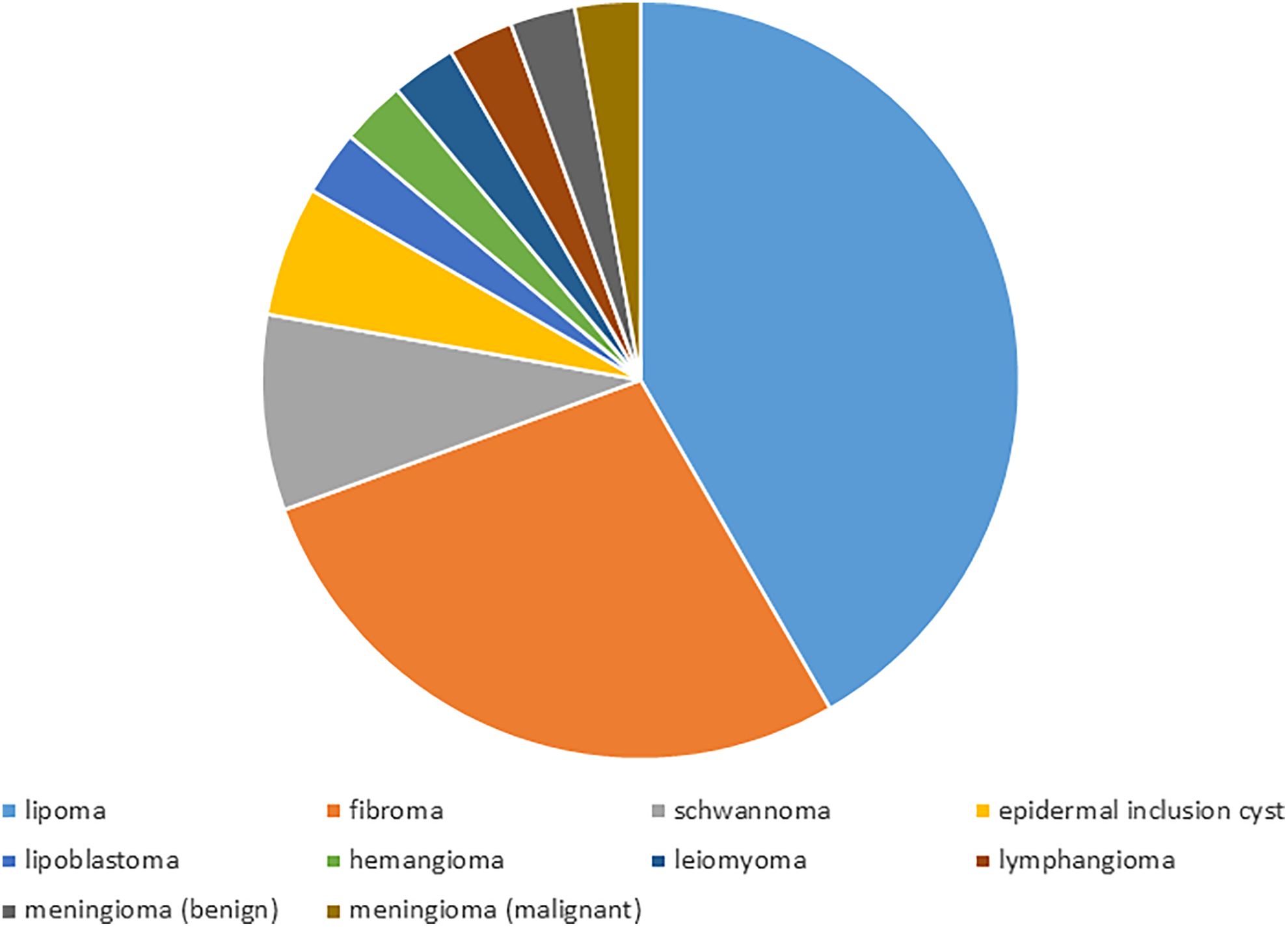
Systematic review posterior neck mass pathologies.
Discussion
The results of this retrospective series and systematic review confirm that mass lesions of the posterior neck represent predominantly benign pathology. There were no instances of malignancy within our single-institution retrospective and only a single case report describing a cancerous pathology was discovered in the systematic review (malignant meningioma). 15 For both our retrospective series and systematic review, lipomas were by far the most common pathology represented. Usually presenting as slow-growing painless masses, lipomas can often be diagnosed by history and physical examination alone. On ultrasonography, lipomas typically have a characteristic, striated appearance that can be very helpful in confirming the diagnosis. 24 -26
For patients who undergo excision of a posterior neck mass, routine preoperative biopsy can often be avoided if the lesion is confined to the subcutaneous tissue and is clinically reassuring. Posterior neck masses can be removed under both local and general anesthesia depending on patient preference and the size of the lesion. Surgical complications are infrequent given the relative lack of critical structures present in the soft issue of the posterior neck.
The results of the systematic review represent some of the more uncommon pathologies that can present as a posterior mass. Many of these lesions developed deep to or within the posterior neck musculature, which would present as a more generalized fullness or bulge rather than a well-demarcated subcutaneous mass. More extensive preoperative workups with anatomic imaging and biopsies can be indicated for these more complex, atypical pathologies.
Given the retrospective nature, weaknesses of this case series include the potential for data inaccuracies and biases. Patients who underwent excision of a posterior neck mass as a minor procedure in the otolaryngology—head and neck surgery clinics were not included in the study design. Similarly, patients with a posterior neck mass who did not undergo surgery were not included in our retrospective review. It is possible that the exclusion of these patients may skew our results. Although no intraoperative or postoperative complications were encountered, our lack of long-term follow-up for most patients may prohibit our detection of delayed complications. Lastly, pediatric patients are poorly represented in both our retrospective case series and the systematic review, which limits our ability to make conclusions in this patient population.
Conclusions
It is unlikely for a posterior neck mass to represent malignant pathology. For many patients, a sufficient diagnosis can be made on history and physical examination alone. An US can be a useful adjunct in certain circumstances. Computed tomography scans, MRIs, and/or biopsies may be indicated for atypical posterior neck masses. Surgical outcomes for posterior neck masses are favorable.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.