
Abstract
Calcium hydroxide is a widely used endodontic medicament with antibacterial activity. When excessive pressure is applied during injection of calcium hydroxide paste or apical perforation occurs, calcium hydroxide can leak into the maxillary sinus and is adsorbed onto the sinus membrane. Although a leakage of calcium hydroxide may not usually cause clinical symptoms, when a large amount of leakage occurs, it can cause degeneration of adjacent tissue and functional disorder, requiring immediate surgical removal. However, due to adsorption to the sinus membrane, calcium hydroxide leaked into the maxillary sinus is difficult to remove completely. Here, we describe the case of a 47-year-old patient in whom a large amount of calcium hydroxide leaked into the maxillary sinus and was successfully removed using modified endoscopic-assisted sinus surgery, and favorable bone regeneration and sinus membrane regeneration were achieved. In addition, histological and ultrastructural changes of the membrane resulted from the calcium hydroxide were presented.
Keywords
Introduction
Calcium hydroxide is a widely used and highly recommended intracanal endodontic medicament with antibacterial activity that results in resolution of apical lesions and promotion of bone regeneration with calcium deposition. 1 For good penetration into the narrow canal system and convenience of use, calcium hydroxide is mostly used in the form of an injection at low viscosity. Therefore, with iatrogenic apical or root perforation, apical external resorption, overfilling with materials, or application of excessive injection pressure, calcium hydroxide paste may leak into adjacent tissues beyond the root apex and spread easily over the maxillary sinus membrane. 2
Leakage of large amounts of calcium hydroxide paste can cause tissue degeneration and functional disorder by causing pressure and chemical burn on surrounding tissue. 3 Therefore, when extensive leakage into the maxillary sinus occurs, normal physiological functions of the maxillary sinus may deteriorate due to damage to the Schneiderian membrane covering the inner surface of the sinus. However, calcium hydroxide leaked into the maxillary sinus is difficult to remove due to adsorption to the sinus membrane, and there are few reports on surgical removal of the leaked calcium hydroxide.4,5 The aim of this study is to describe a case where a large amount of calcium hydroxide paste injected into the maxillary sinus was removed using a modified endoscopic-assisted approach and present histopathologic changes of the sinus membrane directly exposed to calcium hydroxide along with transmission electron microscopy (TEM) images.
Case Presentation
A 46-year-old female patient was referred to the Department of Oral and Maxillofacial Surgery, Seoul National University Dental Hospital with maxillary sinusitis resulting from a foreign body in the left maxillary sinus (Figure 1). The foreign body was suspected as to be calcium hydroxide pasted used as canal-filling material in endodontic treatment. It spreads from the upper left second premolar to the left maxillary tuberosity. On computed tomography images, the foreign material reached up to 19 mm above the maxillary sinus floor, and mucosal thickening around the foreign material and erosion of the posterolateral wall of the maxillary sinus were observed.
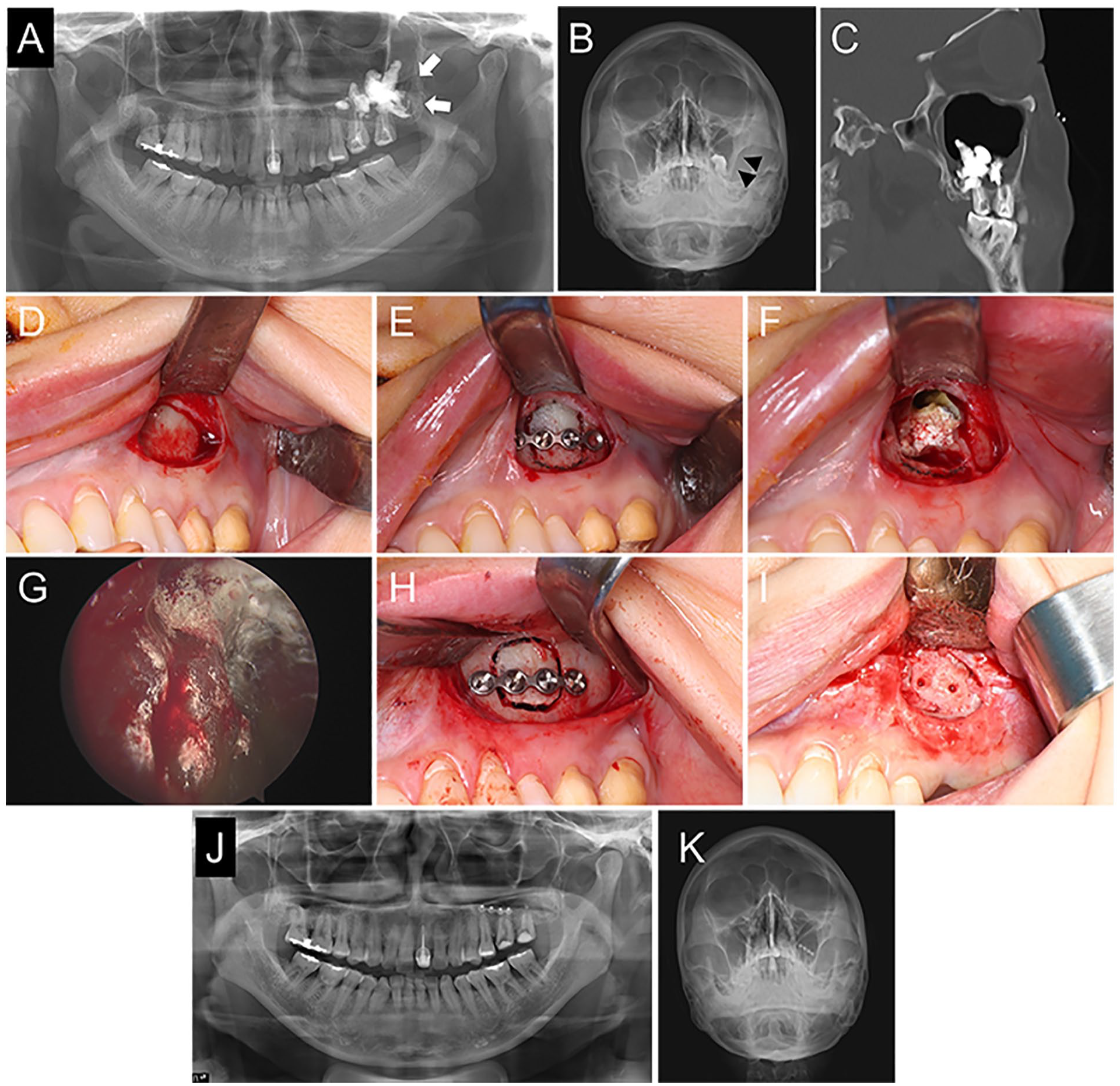
(A, B) Preoperative panoramic view and Water’s view. Foreign material (white arrow) spread from the upper left second premolar to the left maxillary tuberosity, and mucosal thickening (black arrowhead) was found in the left maxillary sinus. (C) Preoperative computed tomography images. (D) Mucoperiosteal flap elevation. (E) Creation of the bony window and application of a microplate. (F) Calcium hydroxide paste in the sinus cavity. (G) Adsorption of the calcium hydroxide paste on the sinus mucosa. (H) Reposition of the bony window and rigid fixation. (I) Restoration of bony continuity around the bony window at 8 months after surgery. (J, K) Postoperative panoramic view and Water’s view taken at 4 months after surgery.
To remove calcium hydroxide paste and pathological sinus mucosa, modified endoscopic-assisted approach was performed under general anesthesia. Briefly, the bony window was created on the antero-lateral wall of the sinus using a rotary instrument. After application of a 4-hole microplate® (KLS Martin Co., Tuttlingen, Germany) to the bony window with 2 screws, the bony window was separated completely. An incision was made on the sinus mucosa and visualized calcium hydroxide paste with surrounding inflamed mucosa under endoscopic view. Due to the inherent properties of the material, calcium hydroxide paste was adsorbed to the maxillary sinus mucosa and was not completely removed by multiple aqueous irrigation cycles. The remaining calcium hydroxide paste was carefully removed along with the pathologic, inflamed mucosa, while the normal sinus membrane and the periosteum below the inflamed mucosa were preserved for postoperative regeneration. The bony window was repositioned to its original position using the previously attached plate and was fixed rigidly. The surgical wound was closed with a layer-by-layer technique.
On histopathologic examination, brown-colored calcium hydroxide paste granules were aggregated or spread over the mucosal tissue (Figure 2). Infiltration of inflammatory cells such as eosinophils, plasma cells, and lymphocytes and engulfment of the granules by macrophages were shown with many accompanying microcalcifications. Ultramicrostructural examination using TEM showed not only calcium hydroxide paste granules phagocytosed by macrophages, but also large amounts of granules in the cytoplasm of macrophages.
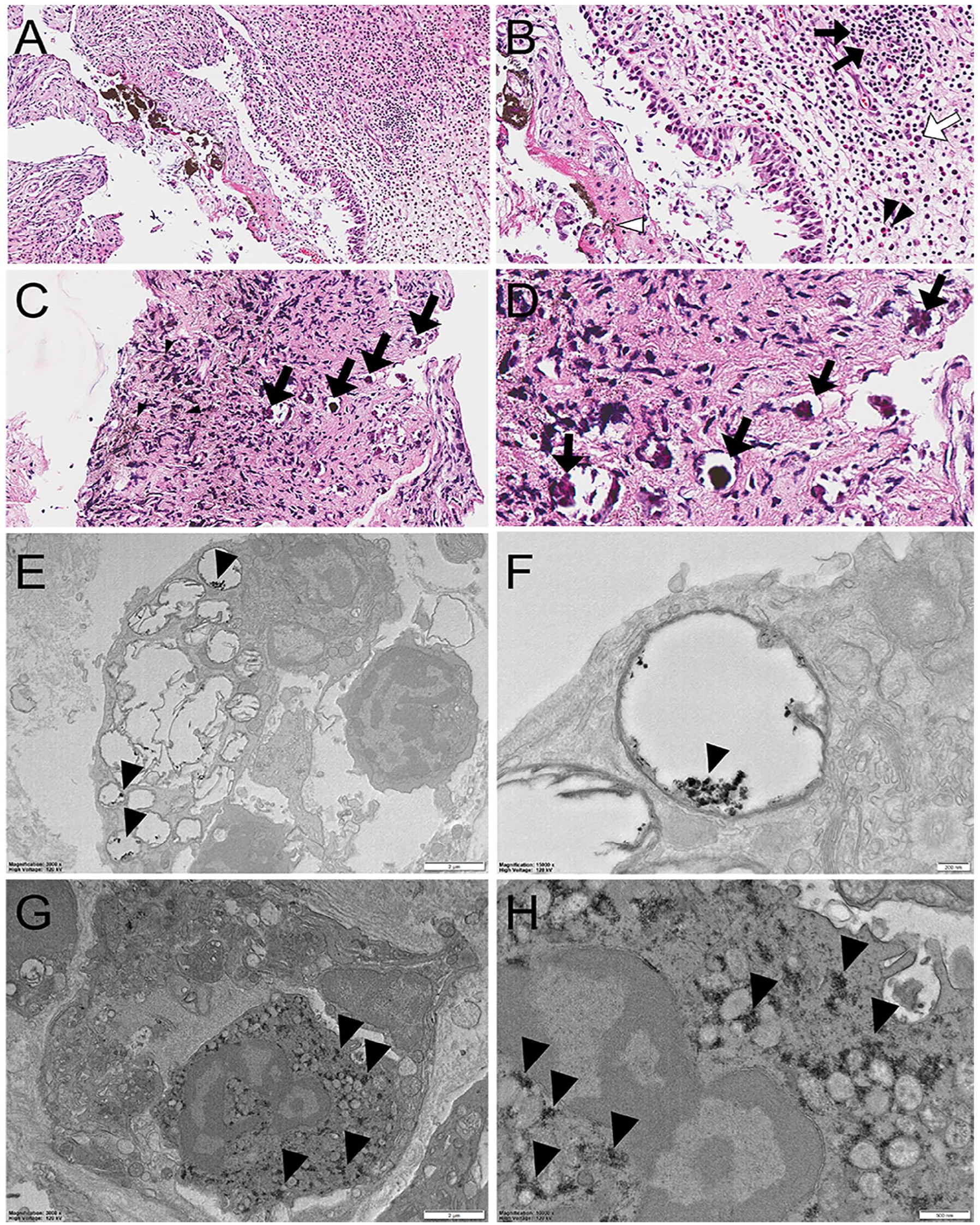
Microscopic and transmission electron microscopic findings of calcium hydroxide paste granules in a lesion. (A, B) Infiltration of inflammatory cells such as eosinophils (black arrowhead), plasma cells (white arrow), and lymphocytes (black arrow) with macrophages engulfing calcium hydroxide paste granules (white arrowhead). Original magnification: A, 100×; B, 200×. (C, D) Brown-colored calcium hydroxide paste granules (black arrowhead) and many spots of microcalcifications (black arrow) in the mucosal tissue. Original magnification: C, 100×; D, 400×. (E, F) Phagocytosis of calcium hydroxide paste granules by macrophages. Original magnification: E, 300×; F, 15,000×. (G, H) Large amounts of granules (arrowhead) in the cytoplasm of macrophages. Original magnification: G, 3000×; H, 10,000×.
At the 4-month follow-up after surgery, panoramic radiograph and Water’s view revealed no significant postoperative complications related to the sinus surgery. During the plate removal at 8 months after surgery, favorable bone regeneration around the bony window was observed with restoration of bony continuity.
Discussion
Although functional endoscopic sinus surgery (FESS) has become the mainstream treatment of maxillary sinus diseases, it may be difficult to completely remove root canal-filling material using only FESS for the following reasons. First, since most of the root canal-filling material leaked into the maxillary sinus is located around the root apex, endoscopic access through the ostium is limited and difficult in FESS. In addition, calcium hydroxide paste has a low viscosity and spreads easily from the root apex to the maxillary sinus, where it is adsorbed. The adsorbed material is difficult to completely remove with only multiple aqueous irrigation cycles through endonasal approach.
Previously, modified endoscopic-assisted sinus surgery (MESS) has been performed for treatment of various maxillary sinus diseases.6,7 The main features of MESS is that a bony window is created on the antero-lateral wall of the maxillary sinus, and the bone fragment is repositioned with a microplate after removing the sinus pathologies using an endoscope. 7 In addition, in MESS, when the natural ostium is obstructed, widening of natural ostium is performed through endonasal approach for adequate ventilation and drainage. In the present study, a calcium hydroxide mass in the maxillary sinus cavity could be identified and removed via transmaxillary approach that provided easy access and sufficient field of view. However, calcium hydroxide paste adsorbed to the maxillary sinus mucosa was not completely removed by multiple cycles of aqueous irrigation. Eventually, with the help of an endoscope, adsorbed calcium hydroxide was completely removed through curettage of the surrounding inflamed sinus mucosa, while the normal, intact maxillary sinus mucosa was preserved.
In terms of postoperative healing, MESS has been reported to result in Schneiderian membrane regeneration and favorable bone regeneration around the bony window. 7 For effective regeneration of the sinus membrane, closure of the sinus membrane after removal of the sinus pathologies can be helpful. However, in the present study, it was difficult to suture the sinus membrane before repositioning the bony window due to adsorption of calcium hydroxide and severe inflammation. Nevertheless, the patient showed resolution of sinus opacification without clinical sinusitis symptoms at 4 months after surgery, and favorable bone regeneration could be achieved with restoration of bony continuity at 8 months after surgery.
In previous studies, calcium hydroxide paste that penetrated beyond the root apex into adjacent tissue caused a foreign body reaction with formation of a granuloma as a tissue reaction, sometimes leading to chronic maxillary sinusitis.5,8 Even though the paste did not flow directly into the maxillary sinus cavity, it migrated to the sinus mucosa and then was secreted into the sinus cavity. Microscopically, the calcium hydroxide paste found in granuloma was primarily engulfed by macrophages and endocytosed by stromal fibroblasts.5,8 It also infiltrated into the cytoplasm of the macrophages. However, these engulfing macrophages eventually experienced cellular apoptosis rather than degrading the calcium hydroxide paste. For the direct leakage of calcium hydroxide paste into the maxillary sinus cavity, several investigators have reported absence of pathological changes and clinical symptoms. 9 However, a radiopaque calcium hydroxide paste remained after 1 year of endodontic treatment. 10 In addition, the histopathological changes of the sinus mucosa caused by direct contact with calcium hydroxide paste are still unclear. In the present study, unlike previous reports, the patient complained of maxillary sinusitis and pain at the related tooth, for which we performed surgical treatment for the removal of leaked calcium hydroxide paste. On histopathologic examination, calcium hydroxide paste invaded the mucosal tissue, and many inflammatory cells were infiltrated with macrophages that engulfed the calcium hydroxide paste granules, similar to granuloma in the previous studies. In addition, many spots of microcalcification were observed. Consistent with previous studies on histologic examination, ultrastructural analysis using TEM in the present study revealed that macrophages phagocytosed calcium hydroxide paste granules, and a large amount of calcium hydroxide was also present in the cytoplasm of macrophages.
To the best of our knowledge, this study is the first to report surgical removal of calcium hydroxide paste leaked into the maxillary sinus with histological and ultrastructural changes of the sinus mucosa. This study suggests that MESS can be useful for effective and complete removal of calcium hydroxide paste that leaked into the maxillary sinus along with satisfactory postoperative outcome.
Footnotes
Consent Statement
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this case report.
Data Availability statement
The data that support the findings of this study are available from the corresponding author, upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (No. 2020R1C1C1014734).
Ethical Statement
This case report was exempted from approval of the institutional review board of Seoul National University Dental Hospital (ERI23027).