
Abstract
Purpose:
The tongue and hyoid bone are responsible for the oral phase of swallowing. The purpose of this study was to assess tongue strength and endurance, and to evaluate swallowing functions in patients who underwent hyoid bone resection surgery.
Material and Methods:
This was an experimental, non-randomized trial. It included participants who underwent hyoid bone resection surgery, divided into 2 groups; post-Sistrunk procedure and post-total laryngectomy. Swallowing problem history was recorded, and tongue strength and endurance were measured using the Iowa Oral Performance Instrument (IOPI). Post-Sistrunk procedure participants also underwent flexible endoscopic evaluation of swallowing (FEES) to assess objective swallowing function. Descriptive and bivariate statistics were used to analyze the association between the tongue strength and endurance, and the type of surgeries.
Results:
The study involved 26 participants, including 16 males and 10 females, with a mean age of 58.4 ± 12.8 years. A total of 10 subjects underwent the Sistrunk procedure and 16 underwent total laryngectomy surgery. The average tongue strength of all participants was 40.8 ± 11.7 kPa and the average tongue endurance was 30.6 ± 13.2 s. The difference in average tongue strength between the post-Sistrunk procedure group and post-total laryngectomy group was not significantly different (37.5 ± 11.6 kPa vs. 44.1 ± 11.3kPa, P = .153). However, there was a statistically significant difference in average tongue strength between male and female participants (46.3 ± 10.0 kPa vs. 32.0 ± 8.5 kPa, P = .001). FEES did not reveal any evidence of objective swallowing abnormalities in the post-Sistrunk group.
Conclusion:
The resection of the hyoid bone, whether partial or total, did not significantly affect tongue strength and swallowing functions.
Introduction
The tongue is a vital organ for maintaining normal food intake, particularly during the oral phase of swallowing. 1 Unlike other bones in the human body, the hyoid bone is not connected to any adjacent bones. It is supported by muscles from the anterior, posterior, and inferior directions, facilitating tongue movement and swallowing. 2 Several tongue muscles, such as the genioglossus, hyoglossus, and inferior longitudinal muscle, are attached to the hyoid bone. Extrinsic tongue muscles attached to the hyoid are the hyoglossus and genioglossus muscles. The hyoglossus muscle originates from the lateral side of the body and the entire length of the greater cornu of the hyoid bone. The hyoglossus depresses and retracts the tongue, causing the dorsum to become more convex. The genioglossus arises from the mandibular symphysis and inserts into both the body of the hyoid bone and the entire length of the tongue. The fibers of the genioglossus contribute to different functions with the inferior fibers protruding the tongue, middle fibers depressing the tongue, and superior fibers retracting the tip back and downward. Although each tongue muscle has its specific action, they do not work independently, and some muscles perform multiple actions in coordination. 2
The Sistrunk procedure is a surgical operation that involves the resection of the central portion of the hyoid bone. It remains as an established technique for the surgical treatment of thyroglossal duct cysts. 3 During the procedure, the hyoid bone is divided between its 2 lesser cornua (Figure 1). The body part of the hyoid bone is removed together with the cyst, en bloc. Conversely, total laryngectomy, a standard procedure for advanced laryngeal cancer, involves dissection of the larynx from above the hyoid bone to below the cricoid cartilage (Figure 2). Thus, both of these aforementioned procedures involve the resection of the hyoid bone.
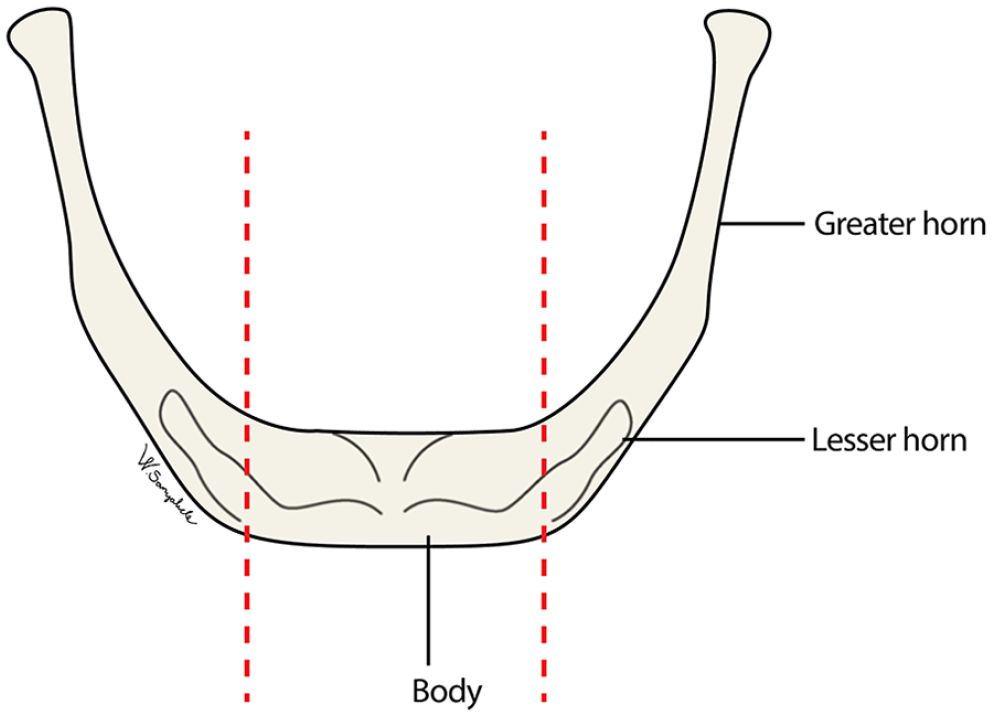
Illustration of removal of the body part of the hyoid bone during Sistrunk procedure.
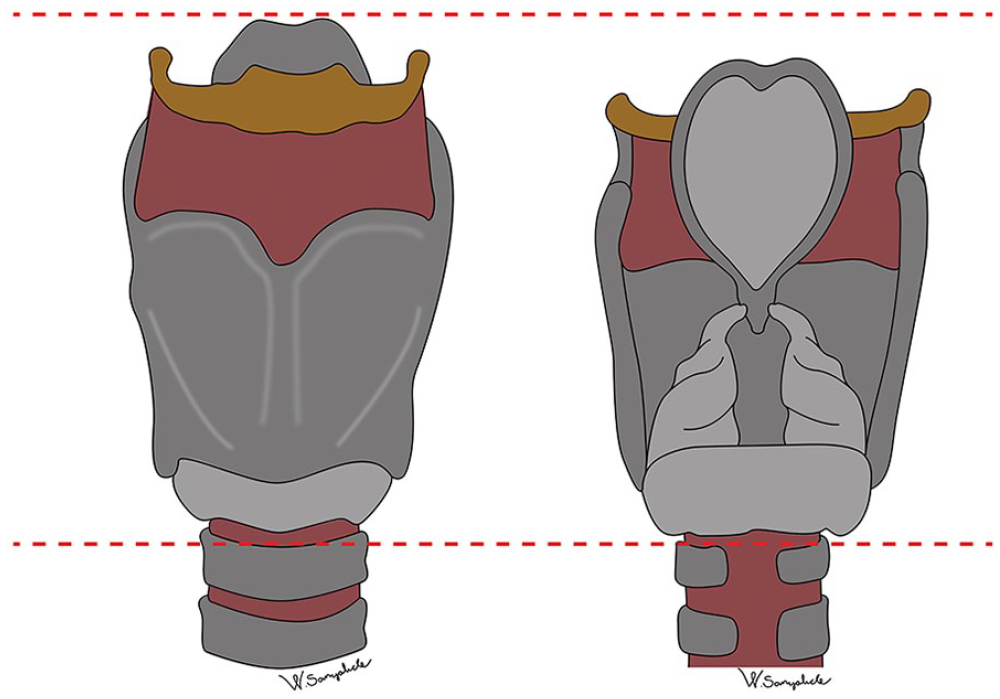
Illustration of total removal of all parts of the hyoid bone during total laryngectomy.
The Iowa Oral Performance Instrument (IOPI) is a widely used tool for measuring tongue strength and is known for its standardization and reliability.4,5 Systematic review and meta-analysis studies have reported mean tongue strength values ranging from 43 to 78 kPa in healthy adults. 6 Furthermore, these studies found that the younger group (≤60 years old) exhibited significantly greater tongue strength compared to the elderly group (>60 years old). However, no significant differences in tongue endurance were observed among different age groups.6,7
A previous Thai study conducted by Keskool et al 8 in a Thai population concluded that the average anterior tongue strength in healthy individuals was 59.5 ± 13.3 kPa, and the average anterior tongue endurance was 10.60 ± 4.1 s. Moreover, they identified 35 kPa as the appropriate cutoff value for anterior tongue strength, indicating a high risk of aspiration. Interestingly, no prior English literature has investigated whether the resection of the hyoid bone affects tongue strength. The objective of our study was to evaluate the tongue strength and swallowing outcomes in patients who underwent hyoid bone resection surgery. Additionally, we aimed to compare tongue strength between patients undergoing partial and total resection of the hyoid bone.
Material and Methods
Study Design and Sample
An experimental, non-randomized study was conducted by investigators at a tertiary care center, specifically a university hospital. This study was carried out between August 1, 2020 and May 31, 2022 following an approval by the Siriraj Institutional Review Board (COA No. Si. 605/2020). The study population consisted of participants aged 18 to 80 years who had undergone hyoid bone resection surgery and were capable of following commands. Participants with a history of cerebrovascular accidents, oral cavity or oropharyngeal mass, and neuromuscular or neurodegenerative diseases were excluded from the study.
Study Variables
The primary predictor variable was the type of hyoid bone resection surgery. Participants were divided into 2 groups: post-Sistrunk procedure group and post-total laryngectomy group. The outcome of interest was tongue strength, including both strength and endurance. Swallowing functions were determined using flexible endoscopic evaluation of swallowing (FEES) which served as an objective swallowing function test. Other covariates included demographic data including gender (male/female), age (≤60 and >60), history of previous radiation, duration from the surgery to the test (<1 month, 1-12 months, and >12 months), and history of swallowing problem after the surgery.
Data Collection
The medical records were reviewed to document the participants’ history of swallowing problems. Subsequently, tongue strength measurement (strength and endurance) was conducted using a new tongue bulb connected with the IOPI.
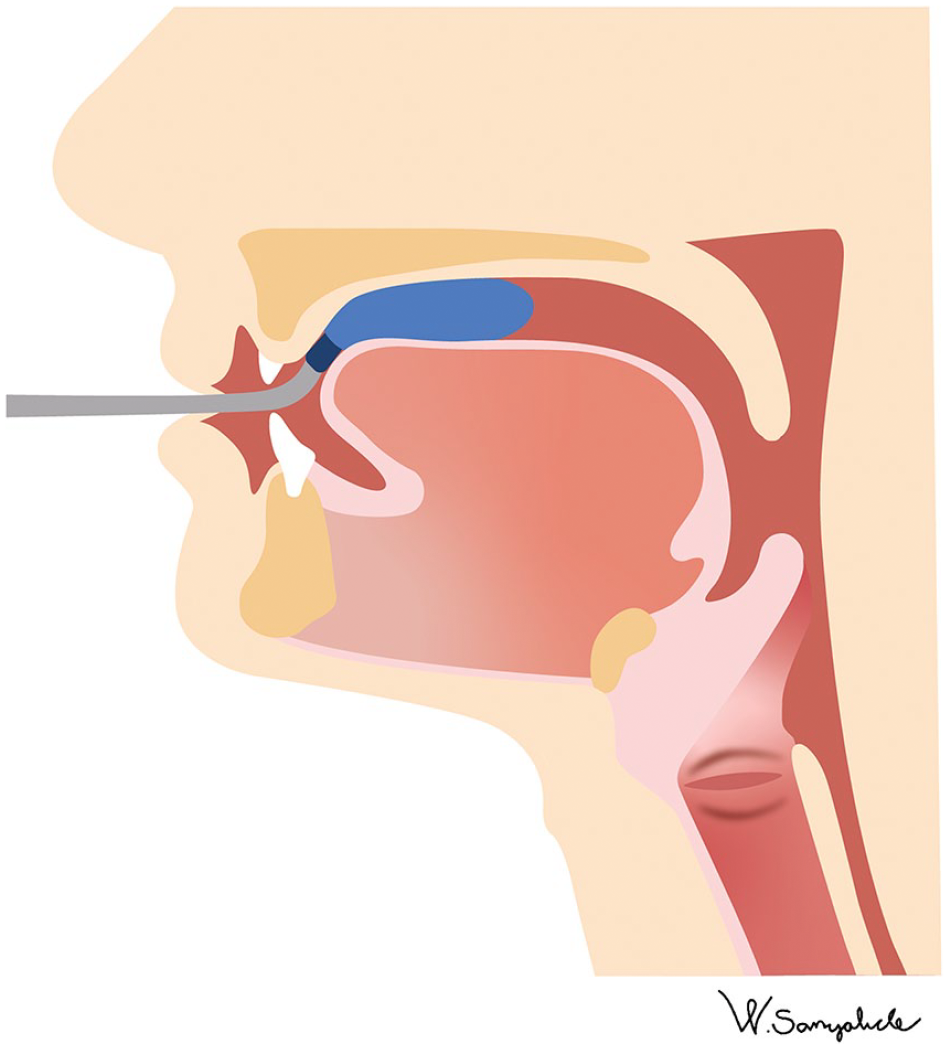
The measurement of tongue strength was performed using an IOPI tongue bulb placed on the anterior part of the oral tongue. Participants were instructed to push the tip of their tongue together against the hard palate just behind the alveolar ridge, while the IOPI tongue bulb was in place (Figure 3). 4 The peak pressure achieved during this procedure was displayed on a large, easy-to-read Liquid Crystal Display (LCD) screen as kilopascals (kPa) (Figure 4). Tongue endurance was assessed using the IOPI by measuring the length of time (seconds) that a patient could maintain 50% of his or her maximum pressure. In this procedure, the target mode on the IOPI was set to 50% of a participant’s maximum pressure. Each participant underwent this procedure 3 times.
A tongue bulb applied to measure tongue strength and endurance.
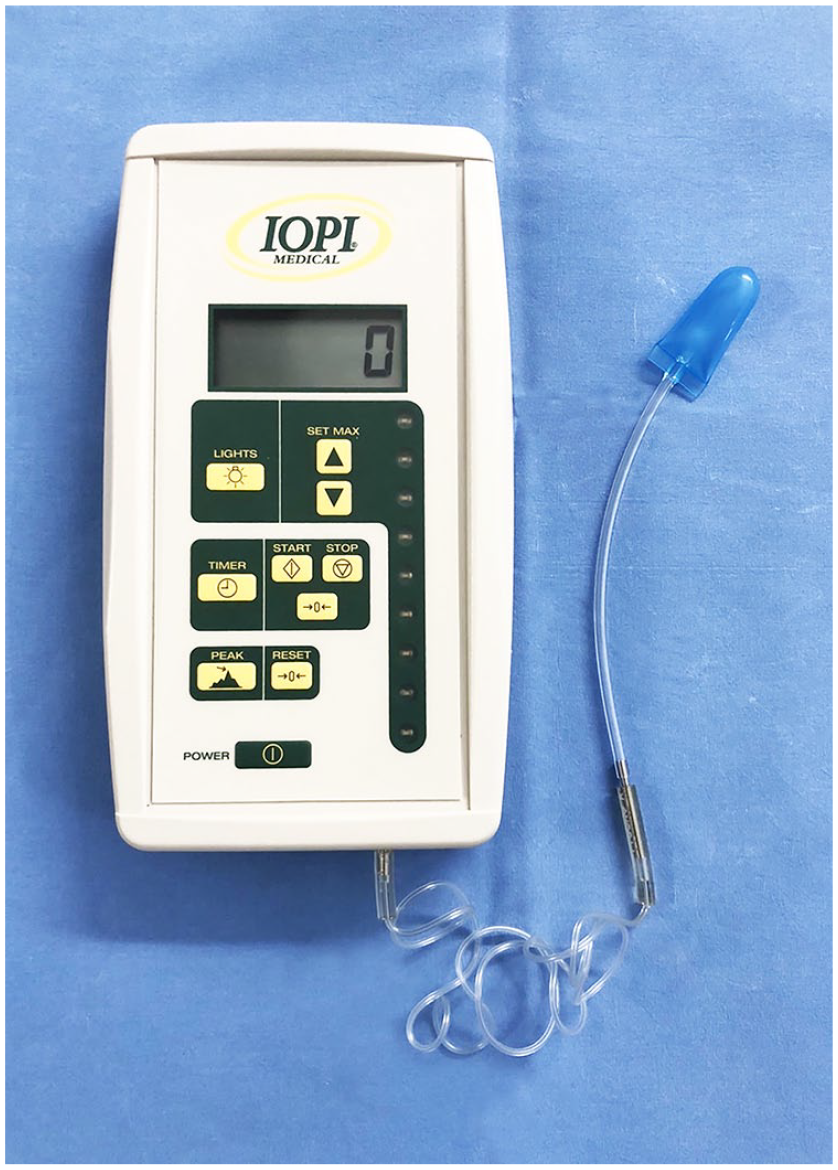
A large, easy-to-read LCD screen of Iowa Oral Performance Instrument.
Participants in the post-Sistrunk procedure group then underwent FEES to assess the objective swallowing parameters, including premature oropharyngeal spillage, nasopharyngeal regurgitation, laryngeal penetration, aspiration, and post-swallow residues.
Data Analysis
All data analyses in this study were conducted using SPSS version 26 (IBM@). Descriptive statistics, including the number and percentage of categorical data, as well as the mean ± standard deviation of continuous data with a normal distribution, were calculated to examine the distribution characteristics of group performance on tongue measures. Between-group comparisons were examined using ANOVA for quantitative data. The relationship of tongue strength and endurance with age was assessed using Pearson correlation, while the relationship of tongue strength/endurance with the duration from surgery to the examination was assessed using Spearman correlation. Linear regression analysis was performed to compare gender with operation while adjusting for age.
Results
A total of 26 adult participants were enrolled in this study (16 males and 10 females). All participants underwent hyoid resection surgery at the Department of Otorhinolaryngology, Faculty of Medicine Siriraj Hospital, Mahidol University, Thailand. The mean age of participants was 58.4 ± 12.8 years. To examine the potential differences based on age, the participants were divided into 2 groups: ≤60 (n = 14) and > 60 years (n = 12). The participants were further categorized into 2 groups based on their diagnosis and surgery type. The first group consisted of individuals diagnosed with thyroglossal duct cyst who underwent “Sistrunk procedure” (n = 10). The second group consisted of individuals diagnosed with advanced laryngeal cancer who underwent total laryngectomy (n = 16). Among the laryngeal cancer group, 10 subjects had a previous history of radiation. The duration between the surgery and the test varied from 1 to 16 months. Based on the questionnaire regarding swallowing problems, none of the patients reported subjective swallowing problems. The demographic characteristics of the patients are presented in Table 1.
Demographic Data of 26 Participants Undergoing Hyoid Bone Resection Surgery.
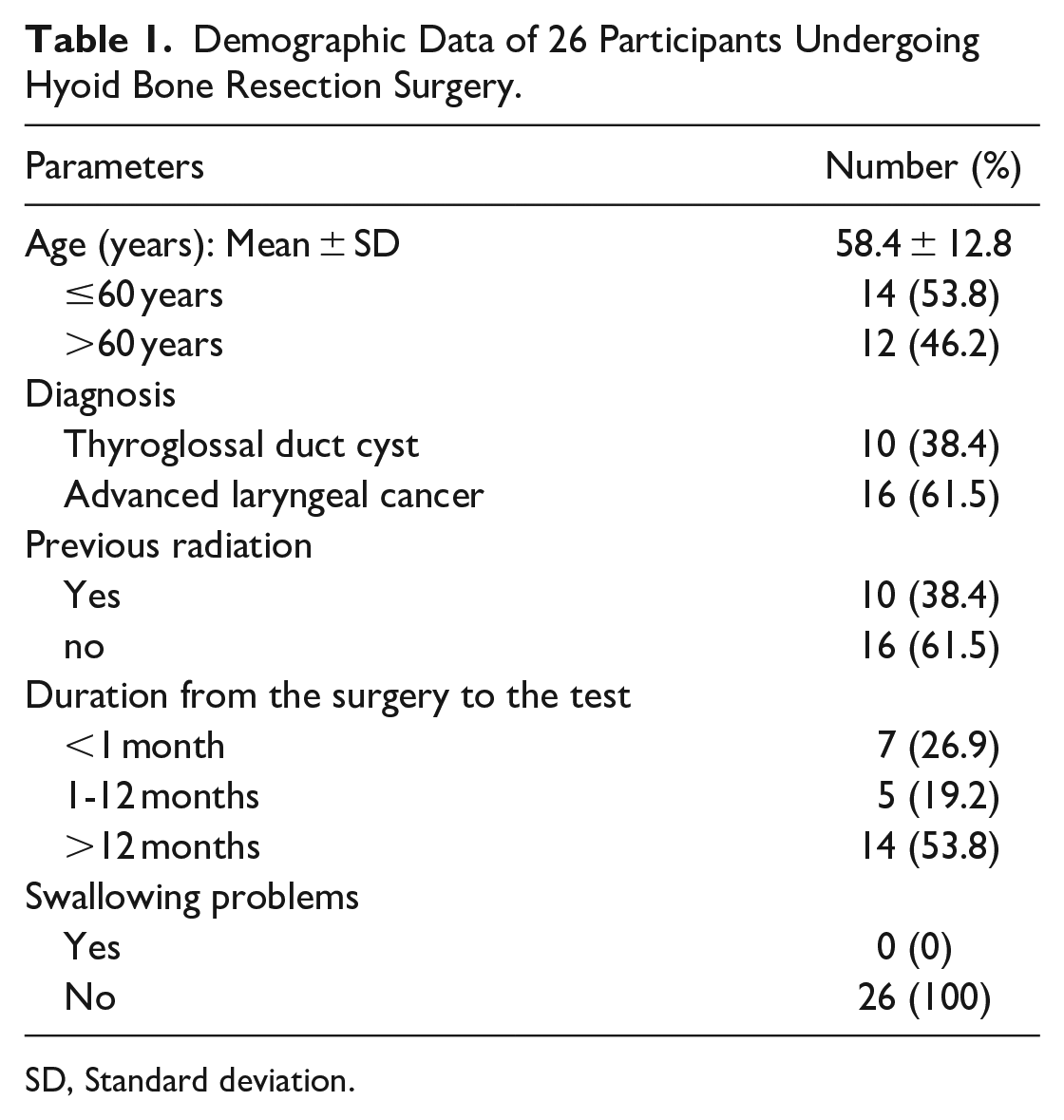
SD, Standard deviation.
Table 2 presents a comparison of tongue strength and endurance among groups with various parameters. The average tongue strength in male participants was 46.3 ± 10.0 kPa, while in female participants, it was 32.0 ± 8.5 kPa respectively, with a statistically significant difference (P = .001). However, tongue endurance in males and females did not differ significantly. Age was found to have a negative correlation with both tongue strength and endurance, with a Pearson correlation (r). It indicated that for each year of increase in age, tongue strength and endurance decreased by 0.239 kPa and 0.270 s, respectively. The tongue strength in the post-Sistrunk procedure group was 37.5 ± 11.6 kPa, whereas in the post-total laryngectomy group, it was 44.1 ± 11.3 kPa. However, there were no significant differences in tongue strength and endurance between these 2 groups (P = .153 and .353, respectively). It is important to note that due to the presence of only one female participant in the post-total laryngectomy group, statistical analysis was not performed for this subgroup. Among the remaining participants, females in the post-Sistrunk procedure had the lowest tongue strength (33.2 ± 8.1 kPa, P = .012), while there was no significant difference in tongue endurance. The analysis did not reveal any significant difference in tongue strength and endurance between participants who had radiation exposure and the non-radiation group. Furthermore, when comparing tongue strength and different surgery durations, tongue strength appeared to be least within the first month after operation; however, there was no statistically significant difference.
Comparison of Tongue Function (Strength and Endurance).
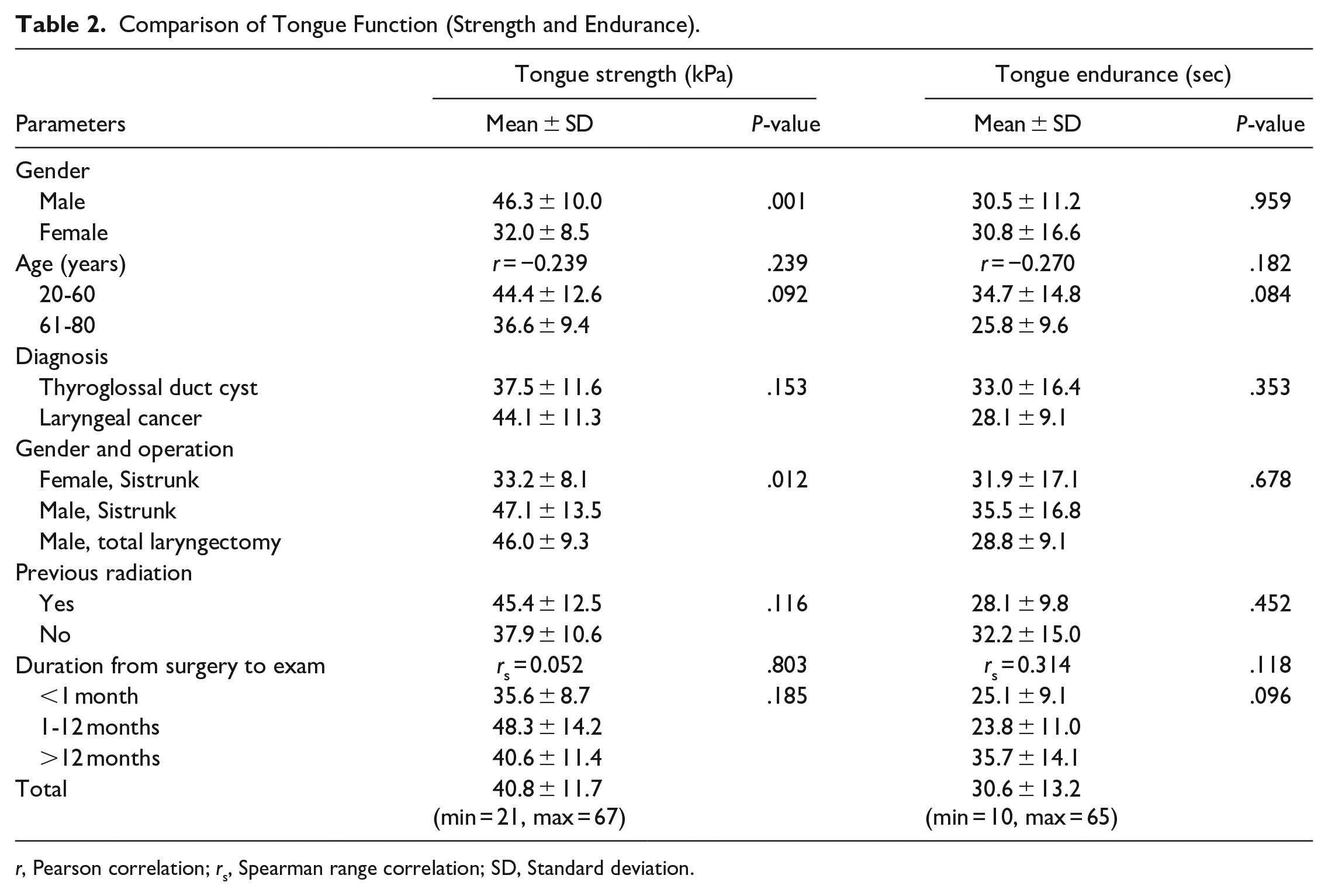
r, Pearson correlation; rs, Spearman range correlation; SD, Standard deviation.
When comparing tongue strength between female and male participants who underwent Sistrunk procedure, females had significantly lower tongue strength, with a regression coefficient of 14.723. Intriguingly, male patients who underwent total laryngectomy had significant higher tongue strength than female patients who underwent Sistrunk procedure (Table 3).
Results From a Multiple Linear Regression of Tongue Strength.
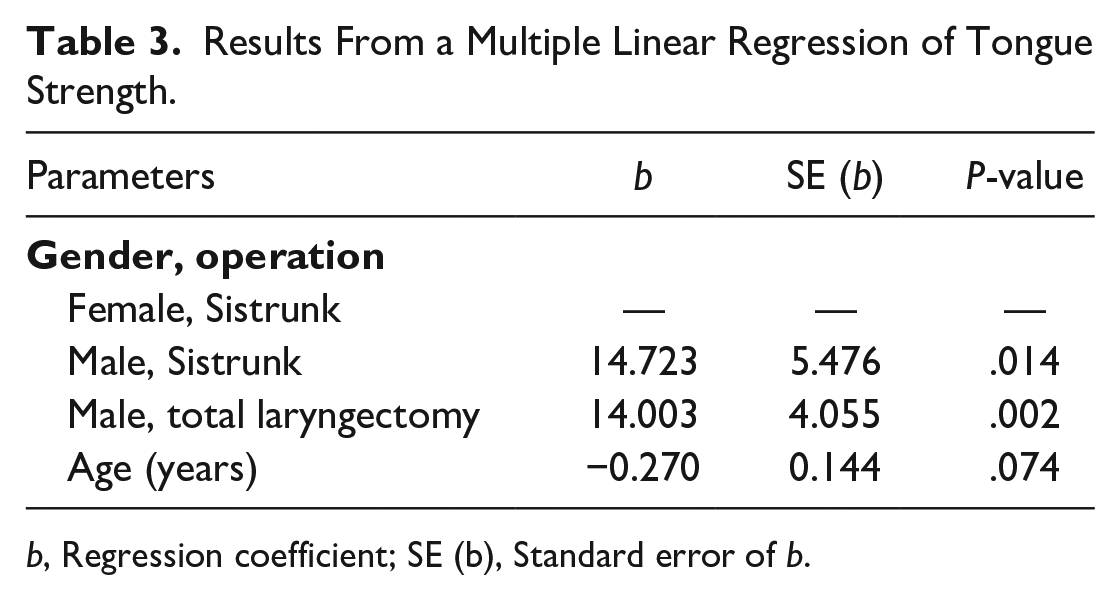
b, Regression coefficient; SE (b), Standard error of b.
The FEES of all participants in the post-Sistrunk procedure group revealed normal findings. There was no evidence of premature oropharyngeal spillage, nasopharyngeal regurgitation, laryngeal penetration, aspiration, or post-swallow residues.
Discussion
The objective of this study was to assess tongue strength in patients who underwent hyoid bone resection surgery by comparing tongue strength between those who had partial and total resection of the hyoid bone and evaluating swallowing function post-surgery. The average tongue strength in all participants who underwent hyoid resection surgery was 40.8 ± 11.7 kPa, while the average tongue endurance was 30.6 ± 13.2 s. None of the patients reported any swallowing problems after the hyoid bone resection. Among subjects who underwent Sistrunk procedure, no objective evidence of premature oropharyngeal spillage, nasopharyngeal regurgitation, laryngeal penetration, or aspiration was observed during FEES.
There was a statistically significant difference in average tongue strength between male and female participants, with a difference of 14.3 kPa and statistical significance (P = .001). Tongue endurance did not show significant difference between genders. When considering the gender and type of operation, significant differences were found among various groups. Male patients in both the post-Sistrunk procedure and post-total laryngectomy groups exhibited higher tongue strength compared to female patients in the post-Sistrunk procedure group (P = .012). This gender-related effect may contribute to the difference in tongue strength. 9 Among male participants, the tongue strength was similar between those who underwent Sistrunk procedure (47.1 ± 13.5 kPa) and total laryngectomy (46.0 ± 9.3 kPa). This result suggests that the presence or absence of the greater horn of the hyoid bone does not significantly affect tongue strength. Other tongue muscles not attached to the hyoid bone may compensate, maintaining adequate tongue strength. Our study also showed that the duration from the surgical date influenced tongue strength, especially within the first month. It is possible that pain or wound-related issues during the early postoperative period affected patient cooperation. Although tongue strength tended to increase over time, this increase is not statistically significant and may be due to patient adaptation.
Despite numerous studies on tongue strength and endurance, there has been no previous research exploring the correlation between tongue strength and hyoid resection surgery. Keskool et al 8 established a cutoff value of 35 kPa for tongue strength, indicating a high risk of aspiration. In our study, the average tongue strength of females was 32.0 ± 8.5 kPa, but no patient experienced clinical aspiration. Many previous studies have revealed that younger patients (<60 years) had greater tongue strength and endurance compared to the elderly population.7,9,10 Park et al 9 confirmed that maximum tongue strength is affected by age-related sarcopenia, which involves a decrease in muscle fibers and motor units, gradual denervation, and a decline in nerve conductance speed. 10 The average tongue strength of patients without previous radiation exposure was 37.9 ± 10.6 kPa compared to 45.4 ± 12.5 kPa in patients with prior radiation exposure. Although these findings contradict previous research, 11 it is worth noting that the radiation group consisted mostly of males, which may have had a significant impact on the higher tongue strength observed in this group.
Besides tongue strength and endurance, ultrasonography plays a crucial role in assessing tongue functions. The tongue, with its multiple musculatures, is uniquely suited for evaluation using ultrasound. Onal et al 12 revealed that pressure exerted by the tonsillar retractor during pediatric tonsillectomy surgeries can lead to subacute tongue edema. They demonstrated the possible role of ultrasonography in detecting tonsillar retractor-induced tongue edema in pediatric patients. Similarly, procedures involving pressure on the tongue, such as suspension rigid laryngoscopy, can result in tongue edema due to ischemia-reperfusion injury. Onal et al 13 also reported the possible use of ultrasonography in detecting tongue edema caused by suspension laryngoscopy procedures, even when it is not visually apparent. Therefore, one limitation of our study was that we only measured tongue strength without visualizing the tongue using ultrasonography.
Conclusion
Our study indicates that the resection of the hyoid bone, whether partial or total removal, did not significantly impact tongue strength and swallowing function in patients. Although tongue strength after hyoid resection was slightly lower than the average in the normal population, it did not reach the cutoff point indicating a high risk of aspiration.
Supplemental Material
sj-docx-1-ear-10.1177_01455613231191019 – Supplemental material for Assessing Tongue Strength and Swallowing Function Following Hyoid Bone Resection Surgery
Supplemental material, sj-docx-1-ear-10.1177_01455613231191019 for Assessing Tongue Strength and Swallowing Function Following Hyoid Bone Resection Surgery by Massupa Sanguanchom, Phawin Keskool, Paiboon Sureepong and Sunun Ongard in Ear, Nose & Throat Journal
Supplemental Material
sj-pdf-2-ear-10.1177_01455613231191019 – Supplemental material for Assessing Tongue Strength and Swallowing Function Following Hyoid Bone Resection Surgery
Supplemental material, sj-pdf-2-ear-10.1177_01455613231191019 for Assessing Tongue Strength and Swallowing Function Following Hyoid Bone Resection Surgery by Massupa Sanguanchom, Phawin Keskool, Paiboon Sureepong and Sunun Ongard in Ear, Nose & Throat Journal
Footnotes
Acknowledgements
We would like to express our sincere appreciation to Assist. Prof. Dr. Chulaluk Komoltri, who was our consulting statistician, all patients involved in this study, Ms. Jeerapa Kerdnoppakhun, and Ms. Ngamrat Treerassapanich for assistance with article preparation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a grant from the Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand. (grant number R016332028).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.