
Abstract
Objectives:
Laryngomalacia is an established cause of stridor and sleep-disordered breathing in children. However, the relationship between laryngomalacia and dysphagia has not been well characterized. The objectives of this study were to (1) describe the patient characteristics, symptoms, and prevalence of dysphagia in children with laryngomalacia and (2) examine the effectiveness of supraglottoplasty in improving feeding.
Methods:
This was a retrospective study of patients with laryngomalacia who underwent a modified barium swallow study (MBSS) at a tertiary academic pediatric medical center between March 1, 2014, and March 1, 2018. Patients were excluded if they did not undergo a MBSS. Comorbidities, airway and feedings symptoms, MBSS results, and surgical history were recorded from each patient’s electronic medical record.
Results:
Forty-four children met inclusion/exclusion criteria. The median age at presentation was 96 days. There was a male predominance (66%). About one-third had a genetic or neuromuscular comorbidity. Most children had stridor (93%) and feeding difficulty (86%), while 50% had parent-reported poor weight gain. Fifty-seven percent of patients had evidence of penetration or aspiration on MBSS. All patients with a positive MBSS had dysphagia symptoms. Fifty-seven percent of patients underwent supraglottoplasty. Postoperatively, 92% reported improvement in dysphagia symptoms.
Conclusion:
Dysphagia is prevalent among a subset of children with laryngomalacia. Symptomatic children may benefit from a swallow evaluation to help determine the need for further intervention. Children who undergo supraglottoplasty for laryngomalacia have improved dysphagia at follow-up, though the amount of improvement directly attributable to surgery is unclear and warrants further investigation.
Introduction
Laryngomalacia is the most common cause of stridor in infants and a well-established cause of sleep-disordered breathing. However, there is a paucity of data examining the relationship between laryngomalacia and swallowing dysfunction. The objectives of this study were the following: To estimate the prevalence of dysphagia in children with laryngomalacia who underwent a modified barium swallow study (MBSS). To identify predictors of abnormality on MBSS among children with laryngomalacia. To determine impact of supraglottoplasty on dysphagia outcomes in children with laryngomalacia.
Methods
The medical records of all patients who were diagnosed with laryngomalacia and subsequently underwent a MBSS at a pediatric academic medical center between March 1, 2014, and March 1, 2018, were retrospectively reviewed and considered for inclusion in the study. Patients were excluded from the study if they did not have laryngomalacia or did not undergo a MBSS at our institution. Pertinent clinical information including medical comorbidities, swallow and airway symptoms, and weight at initial presentation and at follow-up was recorded from each patient’s medical record.
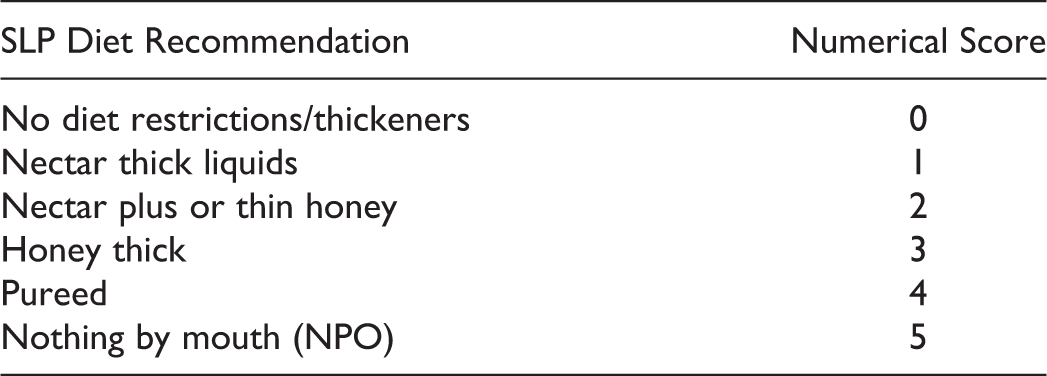
A modified barium swallow study results and speech-language pathology (SLP) diet treatment recommendations before and after treatment were recorded. The MBSS findings were quantified using the SLP recommended diet liquid thickness (RLT) at baseline and follow-up time points as follows:
Subgroups defined by treatment group (observation vs supraglottoplasty) were compared. Differences in categorical variables were tested using Fisher exact test, and differences in continuous variables were tested using Student t test. In addition to these bivariate tests, the impact of supraglottoplasty versus observation on weight gain was also assessed using multivariate linear regression, adjusting for relevant covariates. Statistical analysis was performed using STATA v15.0 software with statistical significance set at P < .05.
Results
Sixty-five children met initial inclusion criteria, while 21 patients met exclusion criteria, leaving a final sample size of 44 patients. The median age at initial presentation was 96 days after birth. There were slightly more males than females (28/44, 64%). Almost one-third (13/44, 30%) had an underlying genetic, craniofacial, or neuromuscular comorbidity (see Table 1).
Demographics of Study Population.a
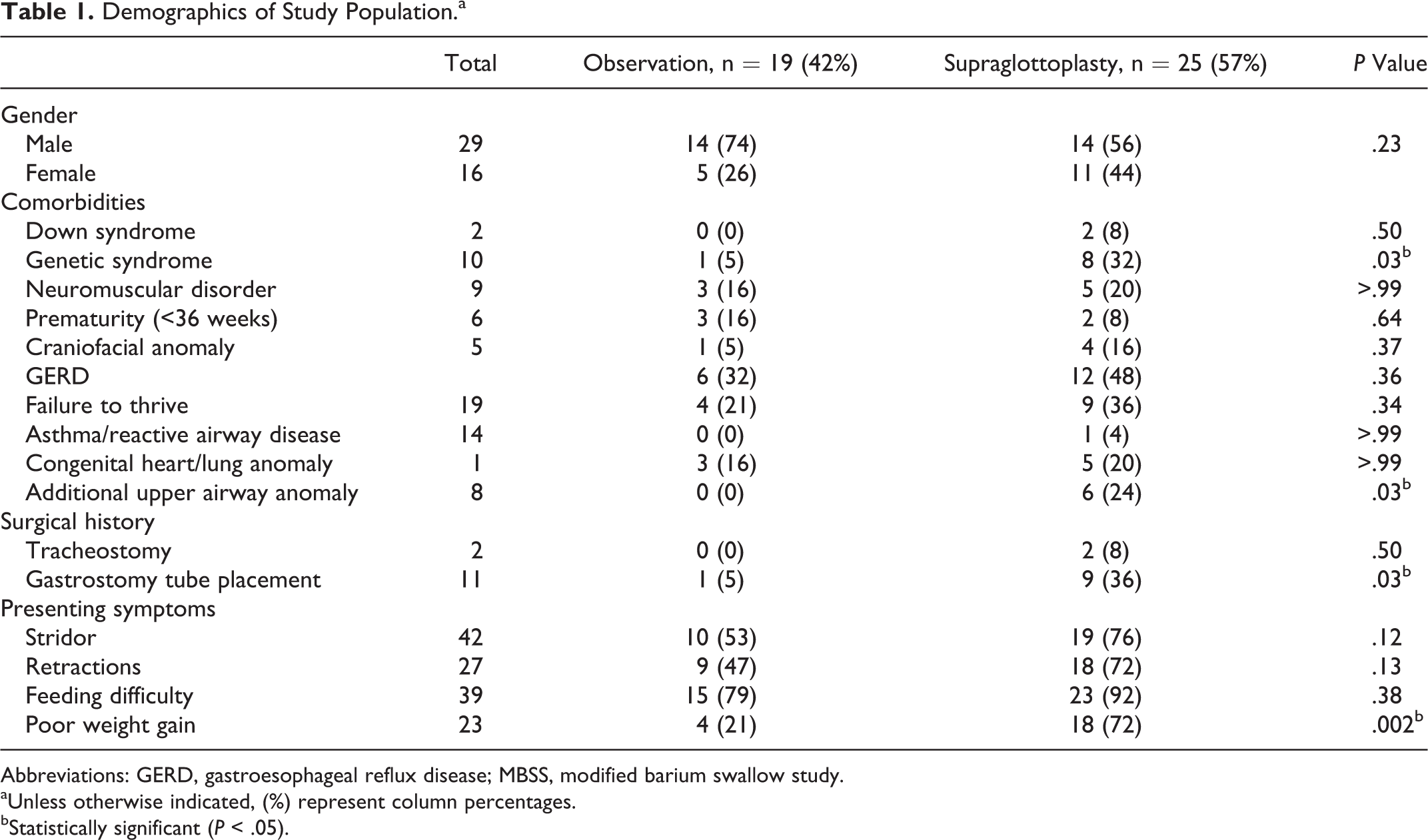
Abbreviations: GERD, gastroesophageal reflux disease; MBSS, modified barium swallow study.
aUnless otherwise indicated, (%) represent column percentages.
bStatistically significant (P < .05).
Most children had symptoms of stridor (41/44, 93%) or feeding difficulty (38/44, 86%). Half had a history of poor weight gain (22/44, 50%) and the majority were found to have laryngeal penetration or aspiration on MBSS (25/44, 57%). All patients with a positive swallow study reported dysphagia or aspiration symptoms such as coughing or choking with feeds.
Just over half (25/44, 57%) of patients underwent supraglottoplasty. Compared to children who were observed, those who underwent supraglottoplasty were more likely to have a genetic syndrome (P = .03), have additional airway abnormalities (P = .03), and have a history of gastrostomy tube placement (P = .03; see Table 1). Most children (23/25 92%) who underwent supraglottoplasty experienced major improvement or resolution of dysphagia symptoms. The two patients who did not report improvement in dysphagia symptoms following supraglottoplasty had an underlying genetic syndrome. Preoperatively, the mean diet score was 2.3 (nectar plus/thin honey), which improved to a mean of 1.1 (nectar thick), as demonstrated in Figure 1. There was no significant difference in final weight or weight gain between children treated with observation versus supraglottoplasty (1.6 kg vs 2.3 kg, P = .06; see Table 2 and Figure 2). In linear regression analysis, when adjusting for baseline age and length of follow-up, there was no significant association between treatment type (observation vs supraglottoplasty) and weight gain (β = .21, P = .52).
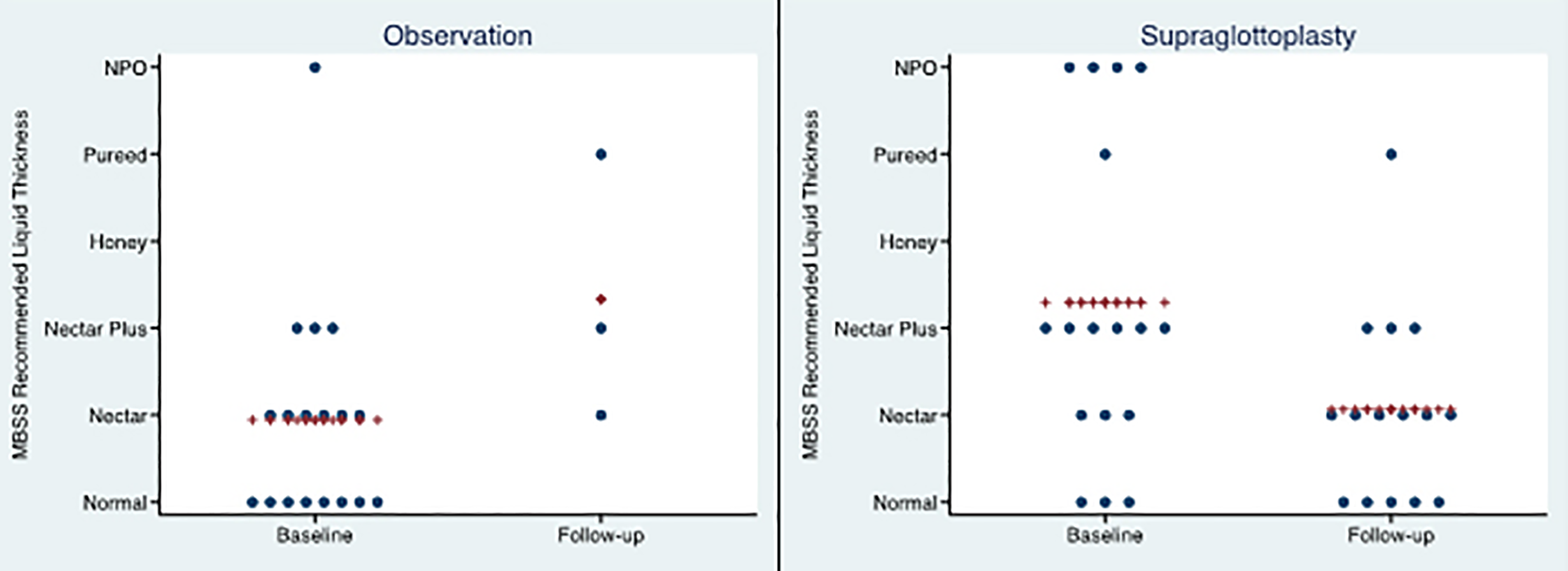
Speech-language pathology RLT at baseline and follow-up. Each dot represents an individual patient’s RLT. The crosses represent the mean RLT. RLT indicates recommended liquid thickness.
Mean Weight and Modified Barium Swallow Study Outcomes.a
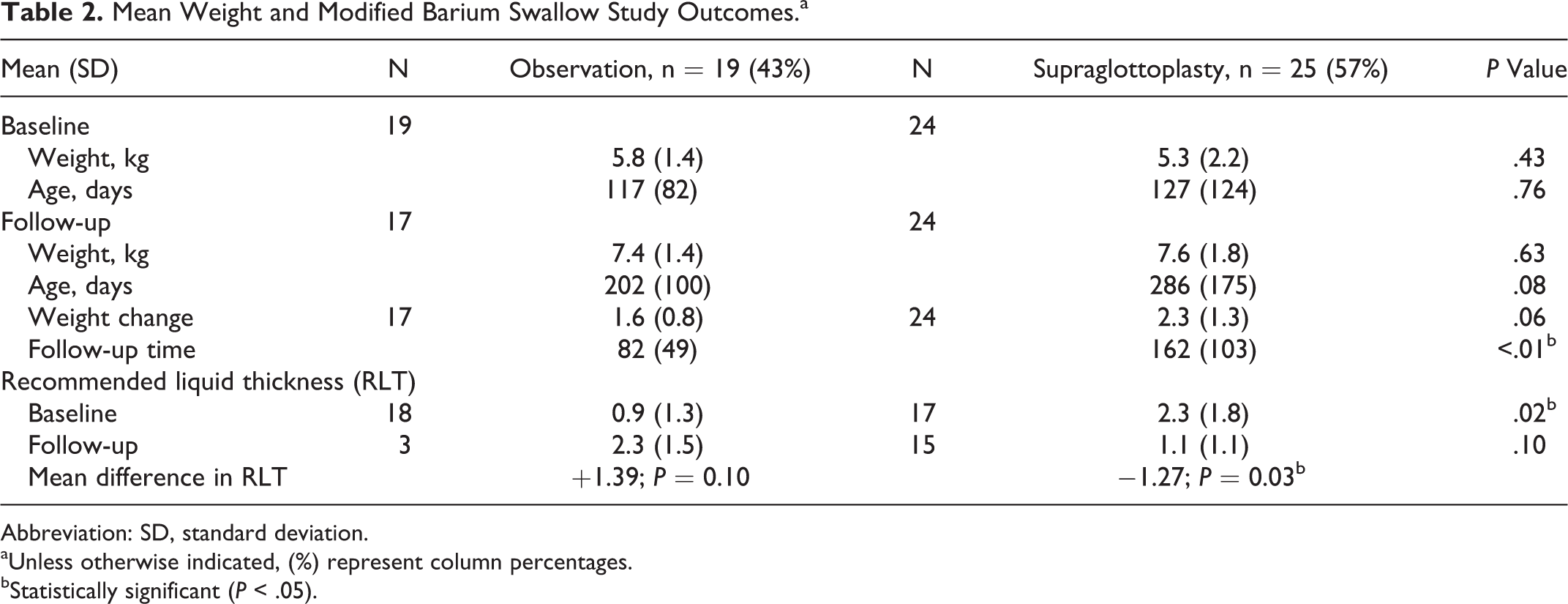
Abbreviation: SD, standard deviation.
aUnless otherwise indicated, (%) represent column percentages.
bStatistically significant (P < .05).
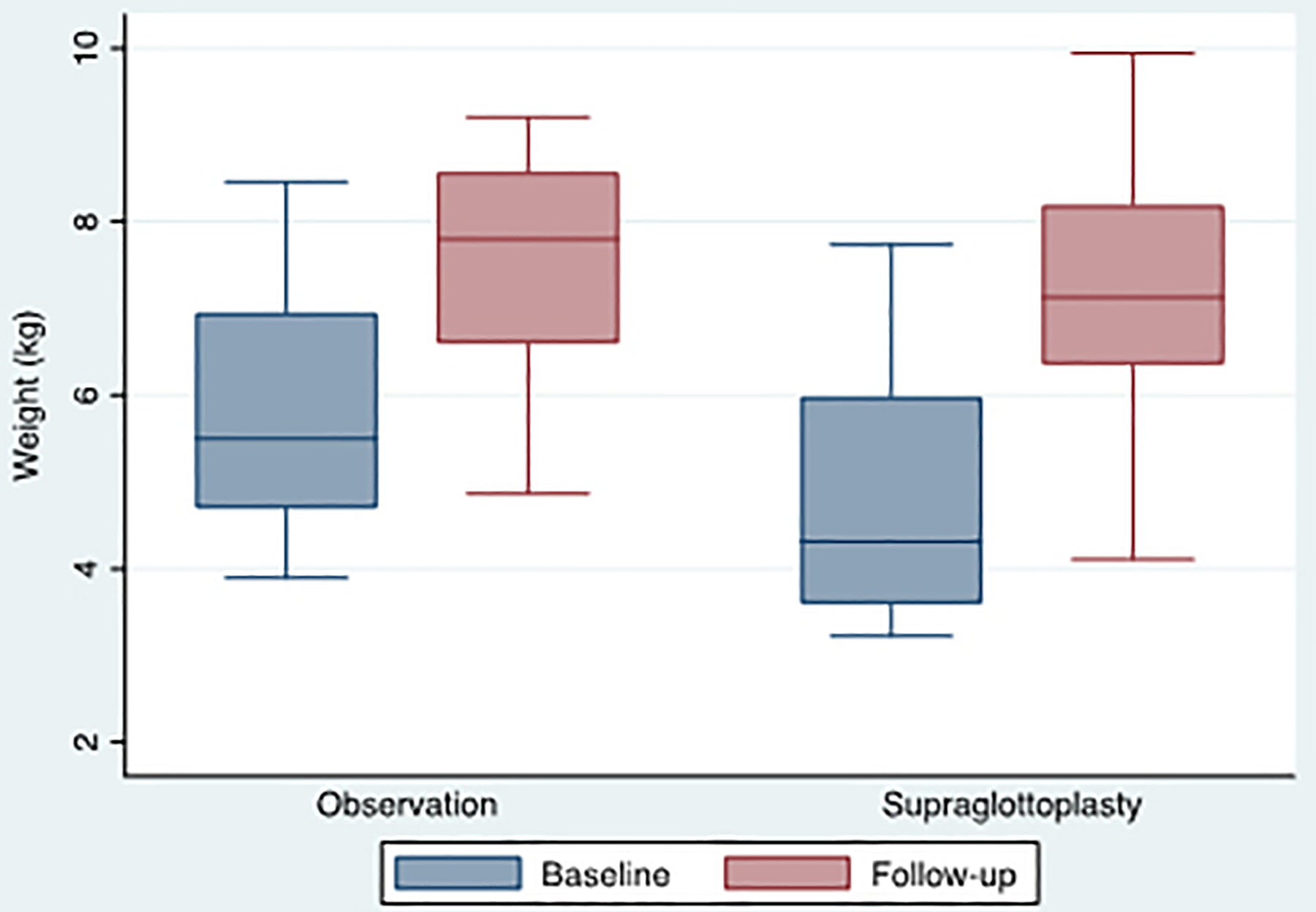
Baseline and follow-up weight by treatment group. Box plot demonstrating baseline and follow-up weights. Horizontal bar represents the mean weight.
Discussion
Laryngomalacia is a common congenital anomaly leading to supraglottic tissue laxity and collapse into the airway. Laryngomalacia is the most common cause of stridor in infants, with a symptom peak at around 6 months of age and gradual resolution in most children by age 24 months. 1 In addition to stridor, laryngomalacia is a well-established and treatable cause of respiratory distress and sleep-disordered breathing. 1,2
In our study population, children who underwent supraglottoplasty had improvement in dysphagia with less stringent diet restrictions based on MBSS at follow-up. However, we were not able to demonstrate a statistically significant difference in degree of MBSS improvement when comparing patients who underwent surgery and those who did not, likely due to insufficient follow-up MBSS data in the observation group.
The relationship between laryngomalacia and dysphagia has not been well characterized in the literature. 1,2 Potential mechanisms that might link laryngomalacia with dysphagia include insufficient laryngeal inlet mechanical coverage during swallow, increased negative pressure in the subglottis due to inspiratory obstruction, and disruption of the highly coordinated normal suck–swallow–breathe mechanism.
Determining the true prevalence of dysphagia in children with laryngomalacia is difficult due to the low sensitivity (<50%) of the bedside swallow evaluation in identifying dysphagia in this population due to high rates of silent aspiration. 3 Hence, many children with laryngomalacia likely go undiagnosed. In our study, 57% of the children with laryngomalacia who were tested with an MBSS showed evidence of aspiration or laryngeal penetration. However, patients at our institution only undergo an MBSS if there is clinical suspicion for aspiration, so this likely overestimates the true prevalence of aspiration in children with laryngomalacia.
With regard to the efficacy of supraglottoplasty in improving swallow, our findings are in agreement with prior studies on the topic. Richter and Thompson studied 50 patients with laryngomalacia who underwent functional endoscopic evaluation of swallow (FEES) and subsequent supraglottoplasty. Of this group, 44 (88%) had laryngeal penetration and 36 (72%) frank aspiration on FEES. After surgical repair of the laryngomalacia, they found an 82% resolution rate of aspiration and 86% resolution of penetration. 4 Simons et al. studied 324 patients with laryngomalacia who were evaluated in an academic medical center’s aerodigestive clinic. In that study, 140 of 185 (75%) patients who underwent a swallowing assessment had abnormal results. 1 Our research is also in general agreement with the work by previous authors who have demonstrated improved oral intake and weight gain following supraglottoplasty. 5,6
In contrast, Rastatter et al. examined 39 patients with laryngomalacia who underwent a surgical repair (supraglottoplasty) for respiratory distress. Of this cohort, 10 were found to aspirate preoperatively by clinical examination or videofluoroscopic swallow study, and only 2 patients had resolution of aspiration postoperatively. 7
The conclusions that can be drawn from this study are limited by a small sample size and the retrospective nature of the study design. Children in our study had high rates of genetic syndromes, medical comorbidities, and symptoms of dysphagia, so care should be taken in generalizing our results to the broader population of children with laryngomalacia who often lack these same attributes and tend to see resolution of symptoms with conservative management. In addition, our study is limited by a selection bias, as children who underwent supraglottoplasty generally had more severe dysphagia and more comorbid medical problems. The fact that children who were observed had less severe dysphagia at baseline might explain why we did not find a relatively greater weight gain in children who underwent surgical repair. In addition, given the natural self-limited nature of laryngomalacia, we are unable to definitively determine how much of the improvement in swallowing outcomes can be attributed directly to supraglottoplasty.
Another limitation was lack of consistent patient follow-up in certain subsets of patients. In particular, few patients who did not undergo supraglottoplasty had repeat evaluations by SLP, and it is likely that those who did continue to follow-up were those still experiencing swallowing or feeding difficulty. This may account for the greater degree of recommended thickening at follow-up among those children who were observed. As a result, it is difficult to make conclusions about the impact of supraglottoplasty on RLT relative to patients who did not undergo an operation.
Given the paucity of research on this topic, and the potential to impact clinical practice, randomized controlled trials are needed to further evaluate the relationship between laryngomalacia and dysphagia.
Conclusion
Among children with laryngomalacia who underwent MBSS, there was a high prevalence of dysphagia. Children with laryngomalacia and symptoms of dysphagia should undergo an objective swallow evaluation to help optimize feeding and prevention of aspiration. Children who undergo supraglottoplasty for laryngomalacia have improved dysphagia with less restrictive diets at follow-up. However, determining whether this improvement is directly attributable to surgery rather than the natural history of the disease warrants further investigation. Children with underlying genetic syndromes are more likely to have persistent dysphagia following supraglottoplasty.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Presentations
This article was presented at the American Society of Pediatric Otolaryngology summer meeting, July 2018. Vail, Colorado.