
Abstract
This case report presents a 65-year-old woman with multiple complications during a revision tracheotomy including subcutaneous emphysema and a pneumothorax. Management of her airway was complicated by a history of recurrent follicular B-cell lymphoma associated with extensive cervical lymphadenopathy. We detail the importance of heightened clinical awareness and the use of intraoperative safety adjuncts when performing revision tracheostomies.
Keywords
Introduction
A tracheostomy is a routinely performed procedure to maintain a secure airway in the setting of prolonged intubation or airway obstruction. Perioperative complications include bleeding and, in more rare cases, subcutaneous emphysema or pneumothorax. 1 Patients requiring revision tracheostomy are at increased risk of both intraoperative and perioperative complications. Here we describe several complications encountered during a revision tracheostomy.
Case Presentation
A 65-year-old-woman with a past medical history of tracheostomy and recurrent follicular B-cell lymphoma, treated with chemotherapy at an outside hospital, was transferred to our center. She was intubated 2 weeks prior at an outside hospital after a pulseless electrical activity arrest. The otolaryngology service was consulted by the ICU for airway evaluation given extensive cervical lymphadenopathy (Figure 1) and in ability to pass spontaneous breathing trials in the setting of prior tracheotomy (Figure 2).
Significant cervical lymphadenopathy secondary to follicular B-cell lymphoma. Taken upon patient presentation prior to any intervention.

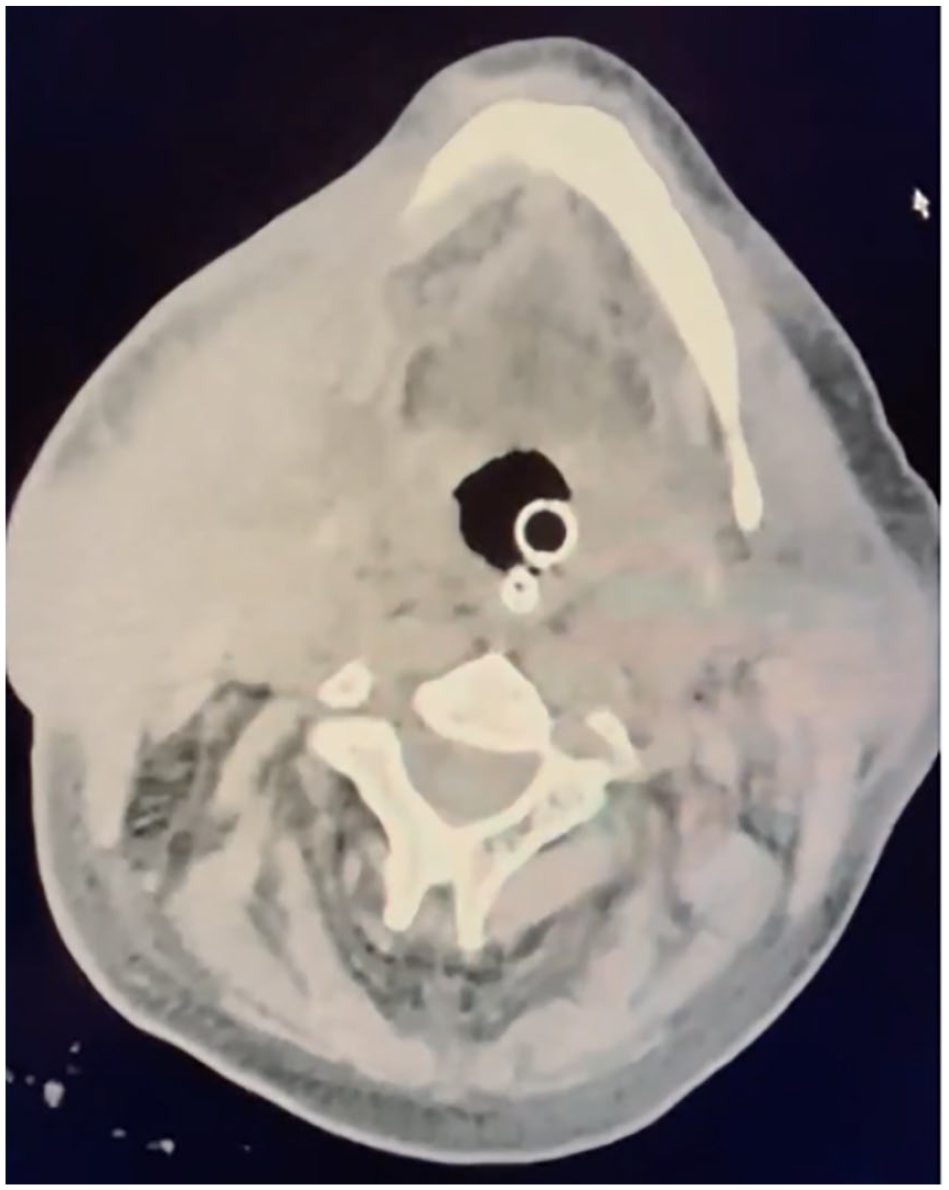
Posterior tracheal wall perforation after open tracheotomy.
Extubation was contraindicated as the patient continued to require ventilatory support, so the decision was made to proceed with a revision tracheostomy. Surgery was delayed for several days due to several social factors: the patient presented with diminished mental capacity, was institutionalized at baseline, and had no family or healthcare proxy established for informed consent. After coordination between social workers, psychiatry, and risk management, informed consent was obtained from the patient and an appointed healthcare proxy.
The patient was brought to the operating room for a revision tracheostomy 5 weeks after an endotracheal tube (ETT) placement. Preoperative computed tomography of the head and neck revealed extensive cervical lymphadenopathy with minimal swelling in the larynx. Dissection and exposure of the airway were without complications. The tracheotomy incision was then made and the ETT was visualized. Withdrawal of the ETT by anesthesiology was met with substantial resistance; however, the tube was pulled back and the tracheotomy tube was placed under direct vision. Following tracheotomy tube placement, anesthesia reported low tidal volumes and end carbon dioxide end tidal carbon dioxide (ETCO2). Aggressive manual ventilation was initiated. Due to steadily declining oxygen saturation, the tracheotomy tube was removed and the patient was intubated per orally with a 6.0 endotracheal tube with return of ETCO2. Oxygen saturation did not exceed 85% despite aggressive ventilatory support.
A flexible bronchoscope was used to confirm the placement of the endotracheal tube. At this point the decision was made to secure the airway with an endotracheal tube placed into the tracheostomy stoma under direct bronchoscopic visualization. Saturation levels remained between 75% and 85% despite confirmed placement of the ETT in the airway. Throughout the case no subcutaneous air was noted. The patient was returned to the ICU at this time.
Immediate postoperative chest X-ray revealed a large left pneumothorax, suspected to be due to aggressive manual ventilations. A chest tube was placed with immediate improvement in oxygen saturation. The following day, the patient remained stable and the decision was made to stabilize the airway by exchanging the endotracheal tube in the tracheostomy stoma for a cuffed tracheotomy tube. The operating room could not accommodate the case until late into the evening. After discussing the case with anesthesiology, ICU, and another attending otolaryngologist, plans were made to exchange the tube at the bedside. Equipments available included multiple tracheostomy tubes, a tracheostomy tray, endotracheal tubes, bougie, endoscopy tower, and multiple personnel on standby including ICU and anesthesia attending physicians.
The ETT was removed, and a #6 cuffed Shiley tracheotomy tube was placed. The tube passed easily and without resistance. There was no return of ETCO2, and with continued ventilation, substantial cervical and facial subcutaneous air was noted. The patient began to desaturate, and the patient was arrested. Immediate initiation of Basic Life Support (BLS) protocol, during which time digital palpation of the stoma revealed a posterior wall defect. With continued palpation of the defect, a tracheal bougie was placed through the tracheostomy stoma beyond the defect. An endotracheal tube was then advanced over the bougie with confirmed ETCO2. There was subsequent return of spontaneous circulation.
The patient was transferred emergently to the operating room where the stoma was explored and the posterior tracheal wall defect was clearly visualized. Stay sutures were placed and a flexible bronchoscope was used to confirm placement of a #6 cuffed Shiley tracheotomy tube. Intraoperatively, thoracic surgery was consulted and found no evidence of esophageal trauma. The patient was transferred back to the ICU in stable condition. The cuff remained inflated for 10 days and she was taken back to the operating room (OR) for her first tracheostomy tube change. At this time the posterior wall defect had healed and a cuffless #6 Shiley tracheotomy tube was easily placed.
Discussion
It is estimated that the annual prevalence of tracheostomy in the United States from 2002 to 2017 was on average 37.5 per 100,000 adults. 2 Tracheostomy is commonly used as a reliable method to secure the airway in head and neck cancer patients, either prophylactically 3 or postoperatively after oncological operations. 4 In some cases, ventilation with ETT has been used in patients with complicating factors where challenging airway maintenance has been predicted, for example, relating to underlying malignancy following intraoral resection; 5 however, this is not an effective long-term strategy for airway management. Extubation following tracheostomy can be complicated by malignancy in setting of appreciable postoperative edema seen in this patient, as well as by the tracheal defect observed in this case.
Current studies suggest that the optimal time for a tracheostomy in patients who require continued mechanical ventilation is 1 to 2 weeks after their initial intubation. 6 In this case, our patient was intubated for 5 weeks as her scheduled surgery time was delayed due to several social factors. There are multiple risks that can arise with prolonged intubation time: ventilator-associated pneumonia, tracheomalacia, vocal cord paralysis, laryngotracheal stenosis, and sinusitis. 7 The patient also presented with a history of a previous tracheostomy and extensive cervical lymphadenopathy. Revision tracheostomies are often associated with both intraoperative and perioperative complications. Common tracheostomy complications include tracheoesophageal fistula, tracheal hemorrhage, and tracheal stenosis. These risks can be further complicated by upper airway infections, obesity, and congestive heart failure. 8 Furthermore, this patient had multiple predisposing factors that placed her at risk for postoperative complications, including poor preoperative nutritional status, prior surgical history, and comorbidities including long-standing follicular B-cell lymphoma, all of which have been shown to adversely affect major surgical outcomes.9,10 However, a tracheostomy is still the preferred management for patients requiring long-term mechanical ventilation. A retrospective study that looked at ICU patients revealed that there was a lower in-hospital mortality rate and higher rate of successful weaning in patients who underwent a tracheostomy in comparison to those that maintained translaryngeal intubation for longer than 14 days. 6
The etiology of the patient’s posterior tracheal defect was likely due to a complication of her initial tracheostomy, damage following the removal of the tracheostomy tube during the code, or during the attempted percutaneous tracheotomy (PDT). While 1 meta-analysis from 1999 has shown higher prevalence of perioperative complications such as tension pneumothorax and subcutaneous emphysema with PDT, more recent studies have shown the opposite, in 1 notably a 6.1% versus 1.4% rate of subcutaneous emphysema in open surgical tracheotomy (OST) and PDT, respectively (P = .05), as well as a 27.2% versus 8.8% risk of minor complications in OST and PDT, respectively (P = .01), and a 11% and 7% risk of major complications in OST and PDT, respectively (P = .03). 11 However, PDT has still been associated, particularly with posterior tracheal wall perforations. 11
Prolonged intubation time along with the patient’s history of recurrent follicular B-cell lymphoma are plausible explanations for the challenges that arose during extubation and subsequent revision tracheostomy. Furthermore, this case highlights the necessity of interdisciplinary communication when performing revision tracheostomies. There are important safety measures to take during airway surgery such as working with anesthesia, utilizing stay sutures, and intraoperative safety adjuncts. Providers should extensively prepare for potential challenges that could arise during airway surgery. In this case, the bedside operation was supplied with multiple tracheostomy tubes, a tracheostomy tray, endotracheal tubes, bougie, and an endoscopy tower in case a backup plan needed to be implemented.
Conclusion
The patient in this case is a 65-year-old woman with significant airway impaction due to cervical lymphadenopathy secondary to follicular B-cell lymphoma. She presented intubated after cardiac complications and required continued ventilation and placement of a tracheotomy tube. The revision tracheostomy was attempted via open surgical technique but became complicated by a tension pneumothorax and consequently resolved with a chest tube insertion. Follow-up beside PDT was then attempted, failing due to the acute development of subcutaneous emphysema via an unidentified posterior tracheal wall perforation of uncertain etiology, likely secondary to one of her attempted tracheostomies. Emergent OR-based open surgical tracheostomy was completed with assistance from thoracic surgery specialists, and the patient was stabilized.
Tracheostomy for treatment of airway obstruction is often unavoidable and indicated in patients such as the woman in this case. There are numerous complications associated with the procedure, regardless of choice of technique. Therefore, taking appropriate precautions to avoid complications such as subcutaneous emphysema and pneumothorax via placement of stay sutures is essential to optimize patient outcomes, including to avoid tracheal perforations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent was waived and not sought in our case study due to the lack of any identifying patient information.