
Abstract
We present a case of a 58-year-old male with type II diabetes managed with metformin and insulin, who presented to the clinic with left chronic otitis media, persistent drainage, a stenotic meatus, and a prior history of 3 canal wall-down mastoidectomies and antibiotic therapy. A revision tympanoplasty with mastoidectomy was performed, and during the postoperative period, the patient had persistent pain and otorrhea, which were managed with opioids and several courses of antibiotic therapy. After symptoms persisted, imaging and culture ultimately led to the diagnosis of fungal skull base osteomyelitis, which was eventually treated successfully. While these complications are rare, their likelihood is increased with treatment delay and in the immunocompromised patient. Close management of immunocompromised patients, including diabetic patients, is vital in identifying complications early to aid in timely diagnosis and treatment to lead to the best possible outcome.
Introduction
Chronic otitis media is surgically treated with tympanoplasty and mastoidectomy to remove the infection and cholesteatoma. If left untreated, several potential complications may cause damage to the surrounding anatomic structures. In some cases, the complications can be fatal.
Infection spreading into the temporal cortical bone is of great concern as it can lead to a series of potentially fatal complications. Zygomatic abscess formation or skull base osteomyelitis are 2 formidable complications, especially in immunocompromised patients.1-3 In immunocompromised patients, skull base osteomyelitis is most commonly caused by Pseudomonas aeruginosa; however, other causative agents such as methicillin-resistant Staphylococcus aureus and fungi have also been previously described.3,4
While these secondary complications from otitis media are rare, there is an increased likelihood of fatal complications in immunocompromised patients or when a principal diagnosis is delayed. 5 For optimal clinical outcomes, it is essential for clinicians to identify and treat the complications early.
The treatment of choice for these cases is modified radical mastoidectomy, followed by abscess drainage and antibiotic therapy.
Case Presentation
We present a case of a 58-year-old male with type II diabetes managed with metformin and insulin who presented to the clinic with left chronic otitis media persistent drainage and a stenotic meatus. The patient had a history of 3 prior canal wall-down mastoidectomies and had previously been on therapy (ototopical drops, ototopical powder, and oral antibiotics). On coronal computed topography (CT), debris in the mastoid and tegmen dehiscence was observed. Because of the small meatus, a tympanoplasty with mastoidectomy and with meatoplasty was recommended.
During surgery, a large mastoid cavity was encountered, which was partially obliterated with cartilage and bone pate to make it smaller. In addition, a meatoplasty was performed to facilitate easier postoperative cleaning. Significant inflammation was observed, and no middle ear structures were visualized. The stapes was most likely eroded as a consequence of a previous cholesteatoma or infection. The tympanic membrane was not regrafted.
During the postoperative period, the patient reported feeling better, and drainage was resolved after the sixth day postoperatively, and ototopical drops were started.
At 3 weeks post-op, the patient reported moderate pain and bleeding. The ear was cleaned, drops were continued, and opioid pain medication was refilled. Two weeks later, the patient returned to the clinic, reporting increased pain and purulent sanguineous drainage. The patient also reported that his blood glucose was well controlled. The patient was prescribed a 1-week course of Keflex.
Four weeks later (9 weeks post-op), the patient returned to the clinic with persistent pain and drainage. The patient was prescribed a 2-week course of ciprofloxacin, sulfamethoxazole, and trimethoprim. The patient’s persistent pain and otorrhea symptoms were still not resolved at 3 months post-op. The patient’s opioid medication was refilled, and the patient’s primary care physician and an infectious disease specialist were consulted. Linezolid was prescribed for 4 weeks per the recommendation of the infectious disease specialist.
A week later, the patient still had persistent pain and went to the emergency room (ER). In the ER, a CT showed an abscess over the zygoma, which was subsequently drained and cultured (Figure 1). In addition, a peripherally inserted central catheter was placed, IV antibiotics were administered, and the abscess was re-aspirated in clinic. The patient reported to the clinic 3 times in 1 week for aspiration of the abscess and IV antibiotics. The culture showed no bacterial growth; however, mold was isolated, but species and sensitivity were not reported.
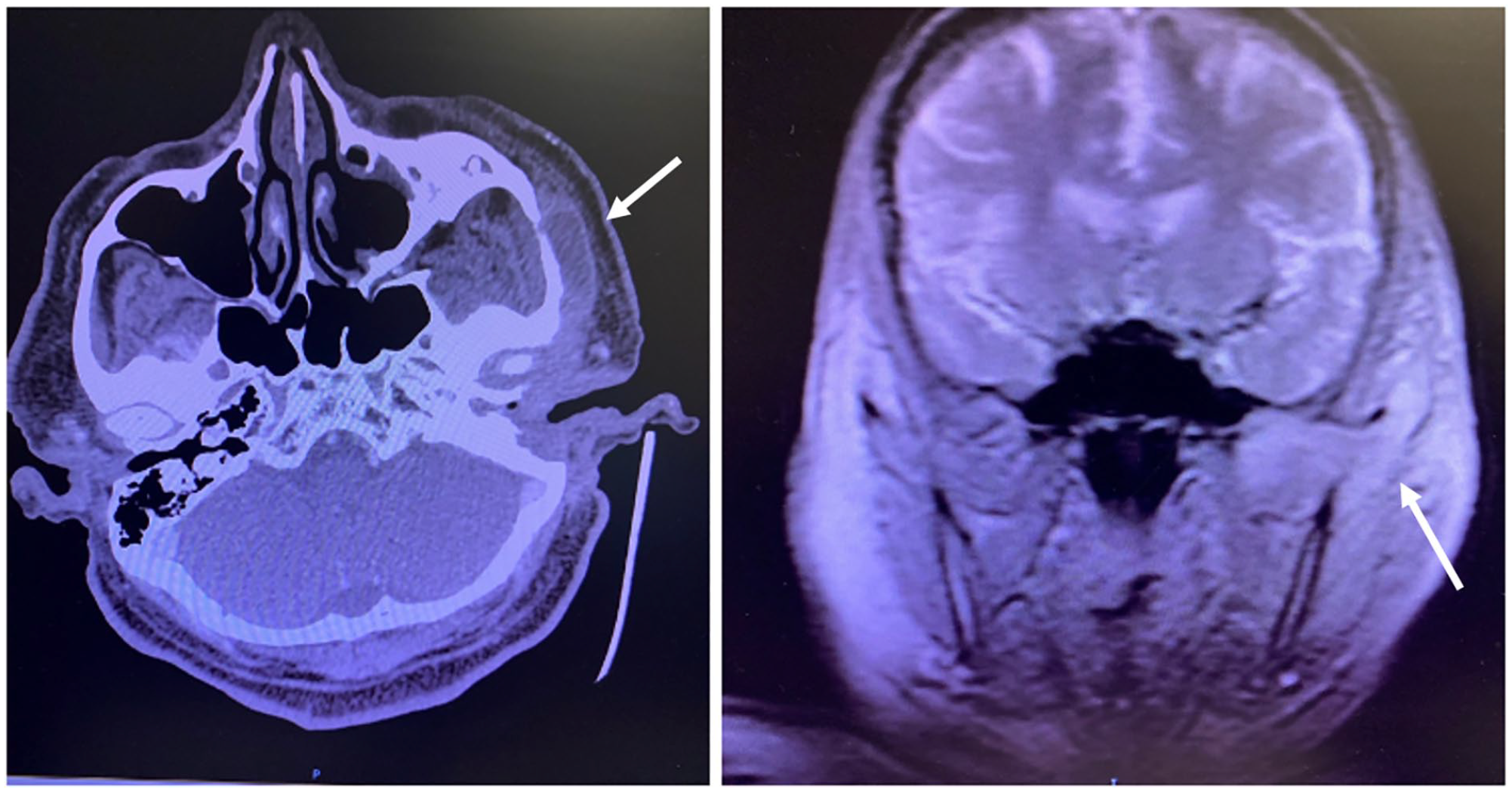
Zygomatic abscess on CT. CT, computed topography.
A repeat magnetic resonance image (MRI) was ordered which showed extensive skull base enhancement, maxillary sinusitis, and extensive inflammation of the infratemporal fossa (Figure 2). The patient was diagnosed with skull base osteomyelitis and 2 weeks later, at 4 months post-op, the culture returned positive for Scedosporium apiospermum. The patient was admitted for pain management, and antifungal therapy (voriconazole) was initiated. On admission, the patient’s fasting glucose was above 200. The patient was eventually transferred to another hospital for debridement by a head and neck surgeon, after which the patient was discharged on continuing antimicrobials and experienced an improvement in symptoms. At 6 months postoperatively, the patient’s symptoms had resolved entirely.
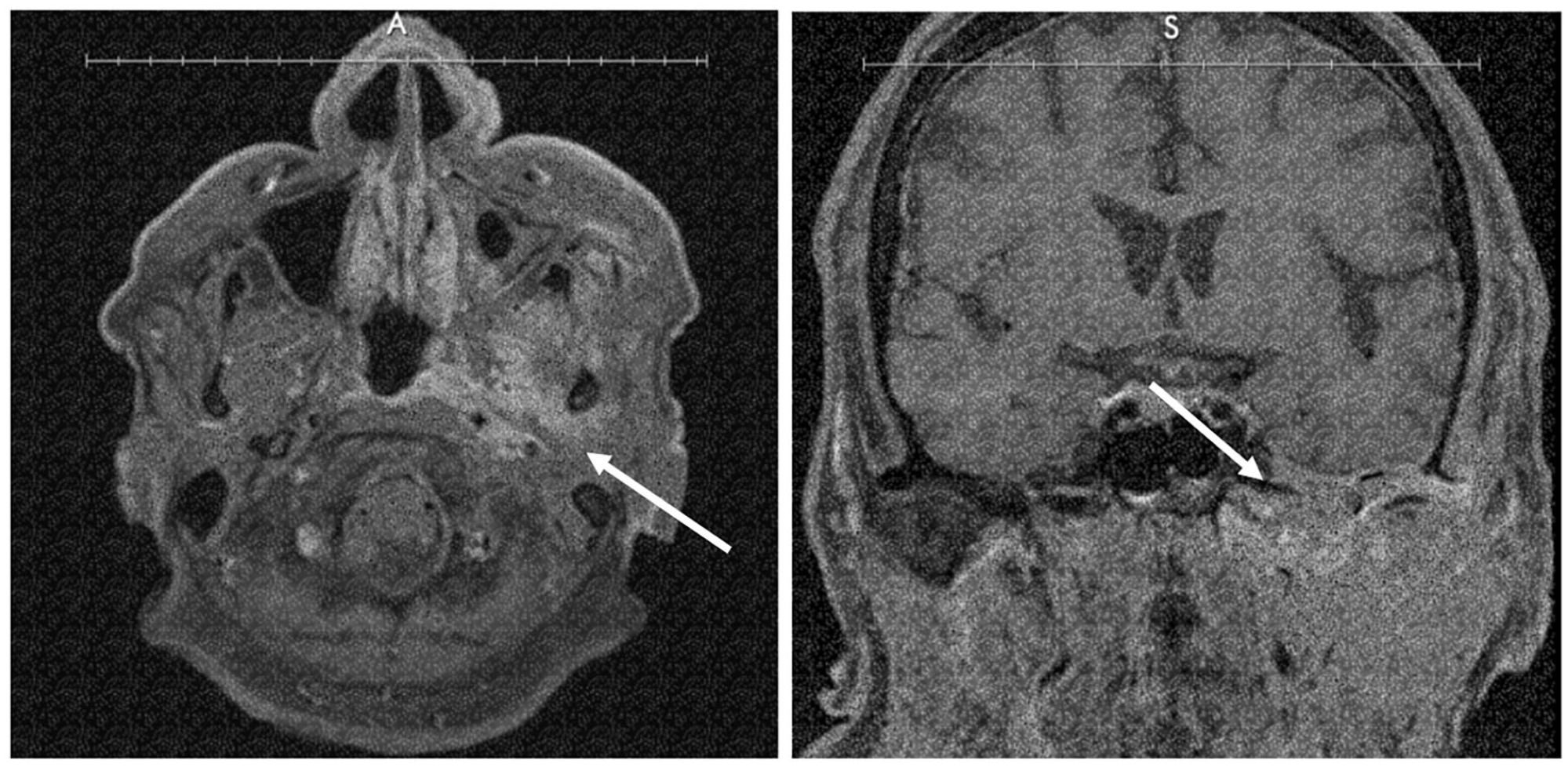
MRI showing extensive skull base enhancement, maxillary sinusitis, and extensive inflammation of the infratemporal fossa.
Discussion
Skull base osteomyelitis can be mistaken as persistent otitis externa or media in earlier stages both otitis externa and media present clinically with nonspecific symptoms such as persistent otalgia, headache, and otorrhea. Indeed, overlapping symptomology can cause delayed diagnosis and treatment as the disease course progresses.5,6 In immunocompromised patients, where the infection can spread quickly, it is important to recognize such complications and their nuanced presentation to mitigate the spread of infection. Early cultures should be considered with unusual clinical presentations, such as a patient with significant pain requiring opiates or marked progression of symptoms despite antibiotic therapy.
Arsovic et al 3 published a series of patients with malignant otitis externa reporting diabetes mellitus type II to be the most common comorbidity observed among the patients. Malignant otitis externa has significant potential to progress to skull base osteomyelitis in uncontrolled diabetics, underscoring the importance of closely monitoring blood glucose levels in malignant otitis externa management. In addition, Khan et al 7 reviewed skull base osteomyelitis and the diagnostic and therapeutic challenges. They identified paranasal sinus infections and direct inoculation from iatrogenic or post-traumatic conditions as the most common route of infection in diabetics and immunocompromised patients. Similar to other colleagues, we recommend CT and MRI examination as soon as possible to aid in prompt diagnosis and avoid treatment delay.5,7,8 Imaging should be ordered as quickly as possible when there is a prolonged persistence of symptoms despite antibiotic therapy.
Conclusion
Timely diagnosis, treatment, and close management of patients with chronic otitis media or externa, particularly in immunocompromised patients, are pivotal since life-threatening complications such as skull base osteomyelitis can present atypically in early stages. In addition, blood glucose levels in diabetic patients should be closely monitored and tightly controlled, as hyperglycemia is highly associated with disease progression. Multimodal imaging strategies should be considered to identify atypical presentations of chronic otitis externa and media in susceptible patient populations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent Statement
Informed consent was obtained for the subject in the study.
Submission Statement
This article is original and has not been submitted elsewhere in part or in whole.