
Abstract
A physically independent and mentally competent 61-year-old gentleman was diagnosed with left upper alveolar spindle cell carcinoma. He underwent left infrastructure maxillectomy with reconstruction and had bismuth iodoform paraffin paste packed in the post-operative cavities. The patient subsequently exhibited labile emotions and acute delirium. Further investigation showed that his urine iodine level was highly elevated. He eventually made a full recovery and returned home.
Introduction
Bismuth iodoform paraffin paste (BIPP) is a commonly used antiseptic dressing in ear, nose, and throat (ENT), dental, and neurosurgical practices for the prolonged packing of cavities. Aside from having bacteriostatic properties that can induce tissue to granulate, its stability in the presence of necrotic tissue often prompts a clean and manageable cavity. BIPP toxicity is rare; however, its prolonged or extensive application can potentially cause neurotoxicity due to systemic absorption of bismuth or iodoform. 1 Several cases of neurotoxicity secondary to iodoform or bismuth toxicity have been reported in the literature, and while it is preventable and reversible, is likely to be fatal if remains unaddressed. This case report explores BIPP intoxication as 1 of the causes of sudden neuropsychiatric symptoms. The findings hope to provide insight for surgeons to recognize the issue and administer immediate removal of BIPP to reverse potential toxicity.
Case Report
A 61-year-old gentleman with underlying diabetes mellitus and hypertension was diagnosed with spindle cell carcinoma on the left upper alveolar in our center. He underwent left open infrastructure maxillectomy and left buccal reconstruction with a split skin graft from the left anterior thigh and palatal obturator placement. BIPP packing was placed on top of the obturator and filled the left maxillary cavity intraoperatively. He was recovering well until 4days post-operatively when his mental state fluctuated with agitation and restlessness. He also exhibited labile emotions and acute delirium. Upon examination, he was disoriented to time and place and could not follow simple commands. He had occasional myoclonus seizures, manifested with facial muscle twitches. Otherwise, the operative site was clean and had no signs of infection. Results from the contrasted magnetic resonance imaging and serial contrasted computed tomography scans of his brain were normal and did not suggest cerebral infarct or paraneoplastic encephalitis.
Paraneoplastic workup was also negative and lumbar puncture ruled out potential infection. Electroencephalogram showed diffuse polymorphic theta–delta slowing with intermittent background suppression, which was consistent with diffuse moderate cortical dysfunction and metabolic encephalopathy. Iodoform intoxication was suspected, and the BIPP packing was removed on post-operative Day 7. Unfortunately, the patient was intubated as his condition further deteriorated. Urine iodide investigation on post-operative Day 14 showed more than 600 mcg/L elevation, suggesting high systemic absorption of the iodoform components. Ultimately, his mental state and overall condition improved with conservative treatment, including neurorehabilitation and aggressive physiotherapy. A repeated urine iodide result was within the normal range. He was discharged home after 2 months of hospitalization (Figure 1).
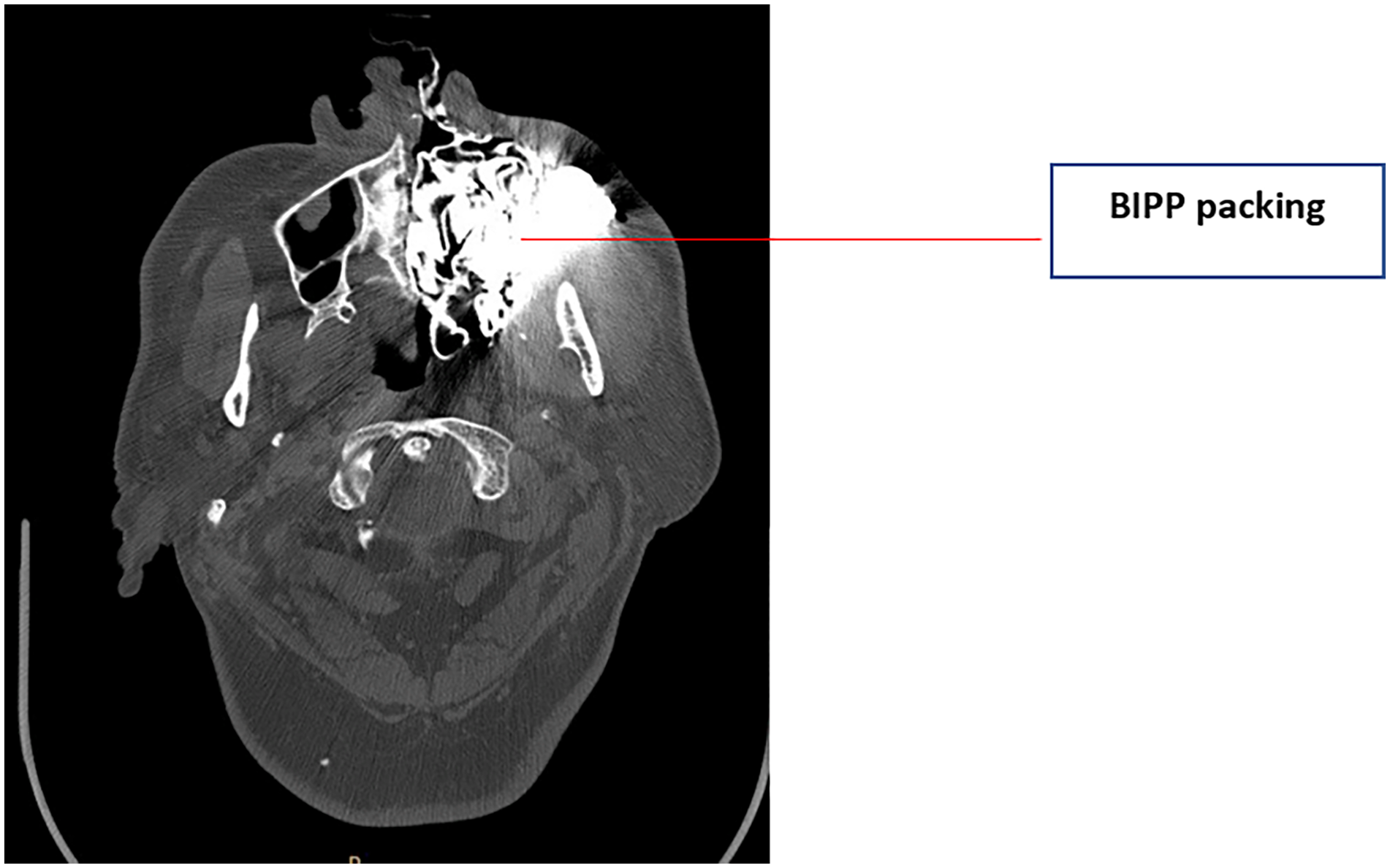
BIPP packing occupying the left maxillary area post left infrastructure maxillectomy. BIPP, bismuth iodoform paraffin paste.
Discussion
Ribbon gauze impregnated with BIPP is a type of dressing routinely used in clinical practices. It was first introduced by Rutherford Morrison in 1916 and contains bismuth subnitrate, iodoform, and sterilized liquid paraffin. 1 Bismuth can cross the blood–brain barrier and bind to enzymes involved in oxidative metabolism, causing reduced oxygen consumption and cerebral perfusion that may lead to metabolic encephalopathy. 2 Roy et al. found a high concentration of iodine and detectable iodoform in the cerebrospinal fluid; the lipid soluble nature of iodoform enhances its penetration into brain tissue. 3 Furthermore, the structure of iodoform (HCI3) is similar to chloroform (HCCI3) and is likely to have an anesthetic effect on the brain. 4 The exact pathophysiology of iodoform encephalopathy has been poorly understood due to limited number of reported cases. However, some hypotheses suggest the potential formation of iodoform metabolites, such as carbon monoxide and formaldehyde, during the metabolism of iodoform. These metabolites are known to have neurotoxic properties and can potentially damage brain tissue, leading to encephalopathy.
Iodoform reacts with granulating tissue to liberate elemental iodine; therefore, plasma iodine should reflect iodoform levels. 4 Besides plasma iodine, urinary iodine can also indicate iodoform exposure as nearly 90% of absorbed iodine is excreted into urine. To the best of our knowledge, no report currently exists regarding the best timing for urine iodide testing. It is not a readily available test in our center and needs to be done in a different center where the result can take between 1 and 2 weeks to be ready. A well-studied outbreak of bismuth encephalopathy in France and Australia in the 1970s established the typical initial manifestation of confusion, myoclonic jerks, and dysarthria within 24 to 48 hours. 2 As myoclonus only occurred later in our patient, we did not suspect bismuth intoxication. Like urine iodide testing, plasma bismuth testing is unavailable in our center. Hence, it must be outsourced at a much more expensive cost, and the result will only be ready after 30 days. Since cost and duration are an issue, we recommend the test be done early upon clinical suspicion. Ergo, having the knowledge about BIPP intoxication and clinical judgment, is crucial to recognize neuropsychiatry symptoms related to the toxicity.
ENT surgeons frequently use BIPP for dressing operative cavities following maxillectomy, mastoidectomy, and ethmoidectomy. It is also commonly used for nasal packing in refractory epistaxis. O’Connor et al. described BIPP as a safe packing for small cavities such as those created after temporal surgery; however, extra caution should be taken when dealing with large cavities such as those produced from maxillectomy. 1 Therefore, the size of cavity and the amount of BIPP pack used correspond well with the iodine concentration in the body. O’Connor et al. had 3 different cases, in which 1 case demonstrated severe iodoform toxicity in a patient after a total maxillectomy whose cavity was packed with BIPP—the patient later recovered upon removal of the BIPP. 1 Apart from the size of cavity, injured mucous membranes of the nasopharynx and nasal cavity accelerated the direct absorption of bismuth and iodine into the bloodstream. Pterygoid venous plexus communicates with the cavernous sinus, undoubtedly augmenting the risk of neurological side effects as it has direct access to the brain. 2 The patient’s renal function was normal and facilitated the excretion of both iodoform and bismuth toxicity. His timing of neurological recovery was consistent with the expected time of 4 weeks to 2 months following iodoform intoxication. 3 The recovery time following bismuth intoxication is less established, although rapid improvement has been seen as early as 2 days.
During the prodromal phase, patients may manifest neuropsychiatric symptoms such as depression, anxiety, irritability, and possibly mild incoordination that can last for weeks or months, followed by rapid deterioration over 24 to 48 hours.5,6 The common presentation includes reduced concentration, memory impairment, as well as myoclonic seizures and tremors. 6 The onset is usually sub-acute and reversible upon withdrawing the BIPP. Alternatively, the use of BIPP can be substituted with whitehead’s varnish as the mixture contains a significantly lower concentration of iodoform, making it a safer option for huge post-operative cavities such as in post maxillectomy.1,6,7
We recommend cautious use of BIPP, especially among elderly patients with renal and liver impairment. Early identification of signs and symptoms followed by prompt packing removal can reduce potential BIPP intoxication and prevent morbidity. Finally, good rehabilitation and physiotherapy are critical as there is no known antidote to iodide.
Conclusion
BIPP packing is generally safe for post-operative cavity dressing in ENT surgery; however, long-term or extensive application of large BIPP packing may cause bismuth or iodoform encephalopathy. Surgeons and neurologists must be attentive to neurological and psychiatric symptoms in patients treated long term by BIPP packing, particularly in cases where the packs are immediately adjacent to neural tissue.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent/Patient Consent
Verbal informed consent was obtained from the patient for their anonymized information to be published in this article.