
Abstract
Objectives:
Good Eustachian tube (ET) function is necessary in order to equalize middle ear (ME) pressure with ambient pressures and avoid barotrauma among divers. Since placement of ventilation tubes is not compatible with diving, balloon eustachian tuboplasty is a potential surgical solution for divers with ET dysfunction (ETD). This is the first report of the outcome of balloon tuboplasty for ETD among divers.
Methods:
A retrospective analysis of medical records and clinical examinations of adult divers treated in a single tertiary medical center.
Results:
Four male divers (age range 21-71 years, 5 ETs) underwent balloon tuboplasty for ETD. None had identifiable risk factors for ETD. Symptom duration ranged from 2 to 5 years and was restricted to diving in 3 patients. The most common symptom was difficulties in equalizing air pressure during descent and ascent, followed by aural fullness and hearing loss. The validated Hebrew version of ETD-7 questionnaire (ETDQ-7H) results were normal in 3 ears and pathological (2.9 and 3.3) in 2 ears. The averaged postoperative ETDQ-7H score was 1.2 points, significantly better than the preoperative score (P < .05). While diving, pressure-equalizing sensation improved in all ears.
Conclusion:
Balloon eustachian tuboplasty is a safe method for treating diving-induced baro-challenge ETD. This procedure can improve symptoms and enable the patient to resume diving.
Introduction
Eustachian tube dysfunction (ETD) is common. Symptoms may include aural fullness, hearing loss, pain and inability to equalize middle ear (ME) pressure. Eustachian tube dysfunction is thought to have a role in the pathogenesis of pathologies, such as acute and chronic otitis media, tympanic membrane (TM) retraction, and cholesteatoma, with their well-known morbidity and rare mortality. 1 Risk factors for ETD include sinusitis, smoking, gastrooesophageal reflux disease, and obstructive sleep apnea, 2 -8 but these are seen only in some of the patients with ETD.
Self-contained underwater breathing apparatus (SCUBA) diving’s popularity is increasing; there are more than 27 million certified sport scuba divers in the world. 9 While diving, good Eustachian tube (ET) function is necessary to allow air to enter the ME spaces in order to equalize ME with ambient pressures and to avoid barotrauma. 10 Eustachian tube dysfunction may cause failure to equalize ME pressure, manifesting with pressure sensation, otalgia, hearing loss, and vertigo. 11 When the trans-tympanic pressure gradient exceeds 100 to 500 mm Hg (4.3-17.4 feet of salt water), TM rupture may occur with a resultant vertigo and life-threatening disorientation. 11 The most common diving-related health issue is ME barotrauma. 11
Adequate ETD evaluation is currently lacking. Pneumatic otoscopy provides invaluable information on the resting position of the drum and possible content of the ME. 12 Otoscopy during a Valsalva maneuver can be performed as well. The nasal cavity and nasopharynx are examined for evidence of acute or chronic inflammation, masses or scars from previous surgeries. The ET orifice is examined in both its resting position and during efforts that activate the peri-tubal muscles, such as swallowing. 13 Tympanometry is the most commonly used ancillary test. Several other ET function tests are also available, among them, manometry, sonotubometry, and tests that measure the ability of the ET to respond to pressure change in an air chamber. Eustachian tube dysfunction questionnaire-7 (ETDQ-7) was developed in 2012 by McCoul et al. 14 Since then, it has become a widely accepted tool to assess ETD and its effects on the patients’ well-being.
Baro-challenge ETD (BC-ETD) is defined as a type of ETD, in which the inability to equalize ME pressure (resulting in aural fullness, popping, or discomfort/pain) occurs, or are initiated, under conditions of alteration to the ambient pressure. 15 Since patients with BC-ETD are typically asymptomatic once they return to ground level (although significant baro-challenge may cause temporary ME effusion or hemotympanum 15 ), in the clinic, the patient’s physical examination and ancillary testing maybe completely normal, leaving the history and ETDQ-7 as the only tools for diagnosis. As compared to air, pressure change as a function of vertical ascend/descend in water is 1000 times bigger; diving challenges ET function to the extreme. This may unmask ETD and expose the diver to barotrauma. Treatment of ETD of any severity in diving candidates is of fundamental importance. Until now, treatment options were limited to addressing risk factors. Placement of ventilation tubes is not compatible with diving. Balloon tuboplasty in free divers and spear fishermen was found to be effective. 16 To the best of our knowledge, this is the first report dedicated to the outcome balloon tuboplasty for ETD among SCUBA and closed-circuit rebreather (CCR) divers.
Materials and Methods
Patients
The study was approved by the institutional ethics committee of the Tel-Aviv “Sourasky” Medical Center, Israel. A retrospective analysis of medical records and clinical examinations was performed. The study participants included were adult divers treated between January 2017 and August 2019 with the diagnosis of ETD. The study included all divers presented to the authors with BC-ETD during the study period. Follow-up ranged from 2 years to 5 months.
Diagnostic Process
Medical history and findings on physical examination including pneumatic otoscopy, Valsalva maneuver under the otoscopic vision and nasal pharyngoscopy, as well as audiometry and tympanometry were conducted in all patients. A validated translated version of ETDQ-7 to Hebrew 17 was used before and 3 months after surgery. Other ancillary tests were performed as needed.
Surgical Intervention
Balloon dilation of the ET (BDET) was performed trans-nasally in all enrolled study participants. Balloon dilation of the ET was performed under general anesthesia by a single surgeon (O.H.), using the Spiggle & Theis (Spiggle & Theis Medizintechnik GmbH, Overath, Germany) 20 × 3 mm balloon system following the manufacturer’s recommendations. The balloon was inflated to a pressure of 10 bars maintained for 2 minutes. Tuboplasty was done under direct view with a rigid 30° endoscope through the nostril ipsilateral to the tube dilated. Preoperative assessment, intraoperative findings and technique, and postoperative outcomes were evaluated and analyzed.
Statistical Analysis
Categorical variables were described as frequency and continuous variables as average and range. The Student t test was used to evaluate differences between pre- and postoperative ETDQ-7H. Statistical significance was determined as P < .05. Statistical analysis was carried out using the SPSS version 15.0 software (SPSS NC).
Results
Four male divers (5 ETs, 3 right and 2 left) were operated during the study period, 1 diver underwent BDET bilaterally, 18 months apart. Age ranged between 21 and 71 years. None had identifiable risk factors for ETD (obstructive sleep apnea, sinusitis, gastroesophageal reflux disease, or smoking), a known allergy, or other symptoms suspicious for allergic background. Body mass index ranged between 21 and 30.5 kg/m2. One diver underwent adenoidectomy in childhood. Diving habits were different among the study population: 1 recreational diver, 2 professional divers (underwater construction and photography), and 1 combat navy diver using CCR system. All were divers with more than 5 years’ experience. The civilians had been diving at least for 20 years before developing difficulties with equalizing pressure. All patients had symptoms for more than 6 months and were treated with nasal steroids for at least 2 months with no symptomatic improvement prior to being offered an intervention. Demographics and general medical conditions are summarized in Table 1.
Demographics, Clinical Presentation, and Outcome of the Cohort.
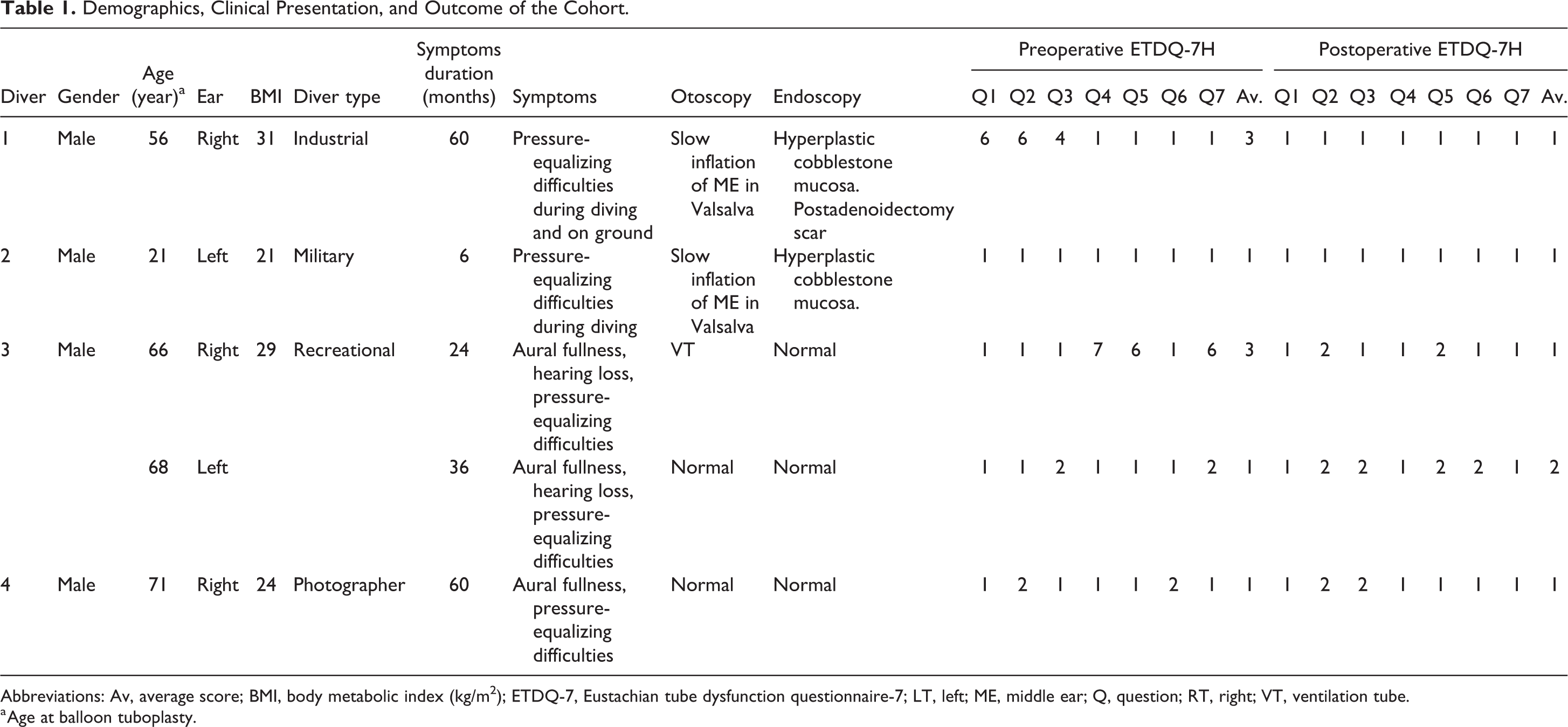
Abbreviations: Av, average score; BMI, body metabolic index (kg/m2); ETDQ-7, Eustachian tube dysfunction questionnaire-7; LT, left; ME, middle ear; Q, question; RT, right; VT, ventilation tube.
a Age at balloon tuboplasty.
Symptom duration ranged from 2 to 5 years and were restricted to diving in all patients except patient #1. None of the patients exhibited BC-ETD from his first diving (median 2 years from first diving). The most common symptom was pressure-equalizing difficulties during descent (4 divers, 5 ears) and ascent (2 divers, 3 ears, respectively), followed by aural fullness (2 divers, 3 ears) and hearing loss (1 diver, both ears).
All diagnostic procedures were performed in normal ambient air pressure of the outpatient facility. Otoscopy was normal in 1 diver (2 ears). Ventilation tube was present in 1 ear. In 2 divers (2 ears), otoscopy showed a slow and somewhat limited movement of the TM in Valsalva’s maneuver. Endoscopic examination was normal in 2 divers. Mildly hyperplastic cobblestone mucosa was seen in 2 divers, one of them with aconcomitant post adenoidectomy scar. Eustachian tube dysfunction questionnaire-7H results are summarized in Table 1 and were normal in 3 divers (3 ears). It was pathological (2.9 and 3.3) in 2 divers, one of them mildly symptomatic when with baro-challenge outside the water. All ears had tympanometry type A, excluding the ear with the ventilation tube, which is to be anticipated given the lack of symptoms outside the challenge associated with pressure change. Since ventilation tube insertion, this patient avoided diving.
No significant change was detected between the findings of preoperative flexible endoscopy, to the intraoperative rigid endoscopy. Averaged postoperative ETDQ-7 H scores were 1.2 points better than the preoperative score; the change was statistically significantly (P < .05). Pressure-equalizing sensation improved in all ears while diving. The 3 SCUBA divers resumed diving without any further difficulties. The navy diver utilizing CCR system reported an improved ET function, which cannot be reflected in lower EDTQ-7 score. This healthy young man’s symptoms were limited to the special circumstances related to combat diving, as reflected in his preintervention normal ETDQ-7 H scores. Given this floor effect, there was no room for questionnaire-related improvement. Despite the improvement, he was symptomatic while performing navy-specific diving with CCR and eventually had to be disqualified from his duties.
Discussion
Recreational and professional SCUBA diving is becoming increasingly popular. 9 Since traveling for diving is common, many otolaryngologists may need to treat patients with diving-related otological conditions, regardless of their location, as well as pre- and postdiving consultations with patients with known ETD. Eustachian tube function is critical for maintenance of adequate ME pressure during diving, since this is the only structure connecting the ME space to outside world via the pharynx. The normally closed ET can open actively with the action of peritubal muscles or passively by positive air pressure. Since even mild ETD can result in barotrauma in the challenging conditions of diving, it may become clinically significant, even if occult without the challenge of changes in ambient pressure.
A fundamental law of gas acting on potentially enclosed air in the ME cleft is Boyle law. This law states that gas volume changes inversely proportionally to the pressure exerted by the gas. During diving and descent from the surface (1 atmosphere, 760 Torr), the external ambient pressure increases. The increased ambient pressure compresses the air in the ME, in a rate of additional 760 Torr every 10 m of descent, unless the diver can equalize it through the ET. The greatest pressure difference per vertical descent distance occurs close to the surface. 18 On descent, ME equalization is an active process, as air must be pushed into the ME space.
When the difference between the ME and ambient pressures reaches 60 Torr, fullness and pain typically occur, and the ET may become blocked. With continued descent to 1.2 m without ME equalization, the differential increases to approximately 90 Torr. The ET then locks, and it can be difficult to open voluntarily. The ET locks as the result of mucosal congestion/edema and collapse of the walls of the ET due to the relative negative pressure in the lumen. The locking of the ET prevents pressure equalization until the diver reverses course and ascends. A forceful Valsalva maneuver at this stage can increase the pressure in the cerebrospinal fluid, and thus the inner ear, and worsen the pressure differential between the middle and inner ear spaces, potentially rupturing the round or oval windows. Continued descent without ME equalization will lead to ME effusion, hemorrhage, or TM rupture. 19 -21
Special consideration is needed in divers utilizing CCR. During World War II, oxygen rebreather technology was adapted so combat divers could operate in enemy harbors without being exposed by surface bubbles. Given the rapid absorption of oxygen, CCR diving has higher rates of barotrauma as compared to regular SCUBA diving. The profile of combat diving often calls for repeated descents and ascents, further straining the ET ability to ventilate the ME cleft. The extreme challenge for ET function posed by combat diving and given that the navy diver had no other symptoms the normal score of the ETDQ7 can be explained.
Last to be factored is the fact that divers have an independent risk factor for chronic sinusitis, 22,23 which is an independent risk factor by itself to ETD. 5
Baro-challenge ETD is defined as the inability to equalize ME pressure with changes in ambient pressure. 1 5 Eustachian tube function is normal in stable ambient conditions. In these circumstances, ET function test on the surface such as pneumatic otoscopy, movement of TM with Valsalva maneuver and tympanometry) are normal, making the diagnosis challenging. The diagnosis is mostly based on patient history, including events of actual barotrauma, and abnormal ETDQ-7 score related to diving. Technical difficulties prevent proof of ETD underwater.
The ETDQ-7 scores should be analyzed with caution. The questionnaire was validated among healthy volunteers and ETD-confirmed patients, but divers were not included in the original paper. Validation of ETDQ-7 for BC-ETD awaits further study. The score is most useful to assess changes with time or intervention.
Since BC-ETD is difficult to diagnose on the surface, clinical and radiological pre-diving parameters were defined in order to verify fitness to dive. 24,25 Tympanic membrane movement during Valsalva maneuver as well as others may test ET function in the office. The mastoid air cells system volume is considered a good predictor of ET function in this setting. 26 It may be as large as 30 mL, 50 to 60 times larger than the ME itself, 27 serving as a buffer to the ME. However, having a larger than average ME cleft air–cell system does not prevent diving-related BC-ETD.
Our small cohort included 3 divers (4 ears) with symptoms limited to diving-related BC-ETD. Only 1 patient had some symptoms of ETD without diving. Preoperative ETDQ-7 scores were normal in 2 patients and pathological in the other 2. Postoperatively, ETDQ-7 score was within normal limits in the 6-month follow-up. Commonly used tests such as tympanometry may not capture this type of pathology that is limited to change in ambient pressure. Tests such as response to changes in ambient pressure (hyperbaric chamber, bluestone 9 step test) 28 were not used for this cohort although they may have some value. 29 Potentially ET manometry 30 may have diagnostic value but to the best of our knowledge it has not been validated for diving-related ETD. However, no test is considered diagnostic in these circumstances. 29 The 3 SCUBA divers resumed uninterfered diving. Although ET function in Navy diver using CCR system improved following balloon dilation and his ETDQ-7 scores normalized, he was unable to resume his former activities.
Given these results and the fact that ventilation tube insertion is incompatible with diving, for divers failing conservative treatment, BDET can be a good option. An effort to identify and reverse risk factors for ETD (ie, smoking, sinusitis) and a trail of nasal steroid and decongestants is probably a necessary step before offering a patient BDET. 31 Further investigation is necessary to establish the role of balloon Eustachian tuboplasty in BC-ETD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.