
Abstract
Meningoencephalocele is an abnormal skull base protrusion of fluid, brain tissue, and meninges that can lead to nasal obstruction, meningitis, and Cerebrospinal Fluid (CSF) rhinorrhea. This condition can be managed operatively through an open craniotomy or a less invasive endoscopic approach. Here, we report a case of an 18-month-old female who presented with a meningoencephalocele that was part of the Sakoda complex, a rare neurosurgical phenomenon consisting of meningoencephalocele, agenesis of the corpus callosum, and cleft lip/palate. The patient was initially treated with the endoscopic transsphenoidal approach with subsequent open craniotomy.
Introduction
A meningoencephalocele is a rare anomalous pouch filled with fluid, brain tissue, and meninges that herniate through a skull base defect and presents congenitally or post-traumatically. Rarely, this condition can present as a part of the Sakoda complex, a rare combination of congenital defects including corpus callosum agenesis, cleft lip/palate, optic disc dysplasia, cortical dysgenesis, and anterior skull base encephaloceles. 1 Typically, meningoencephaloceles that protrude through bony defects in the cribriform plate, sphenoid sinus, or ethmoid sinus can be treated with the endoscopic transsphenoidal approach by otolaryngologists and neurosurgeons. We now report a case of an 18-month-old female who presented with a Sakoda complex meningoencephalocele and attempted endoscopic resection that ultimately required an open craniotomy.
Case Report
An 18-month-old female presented to the anterior skull base otolaryngology team with seizures, possibly related to her meningoencephalocele. The patient also had a cleft lip/palate and optic dysplasia, a presentation typically associated with the Sakoda complex, requiring surgical intervention with neurosurgery.
On MRI, the meningoencephalocele, an external ventricular herniation of neural tissues, measured over 8 cm in length and 7 cm in width, with a 5 cm skull base defect (Figure 1). The patient’s hard palate was absent and replaced with the pulsation of the meningoencephalocele; thus, neurosurgery consulted the otolaryngology service for resection of the meningoencephalocele and repair of the skull base defect via an endoscopic approach.
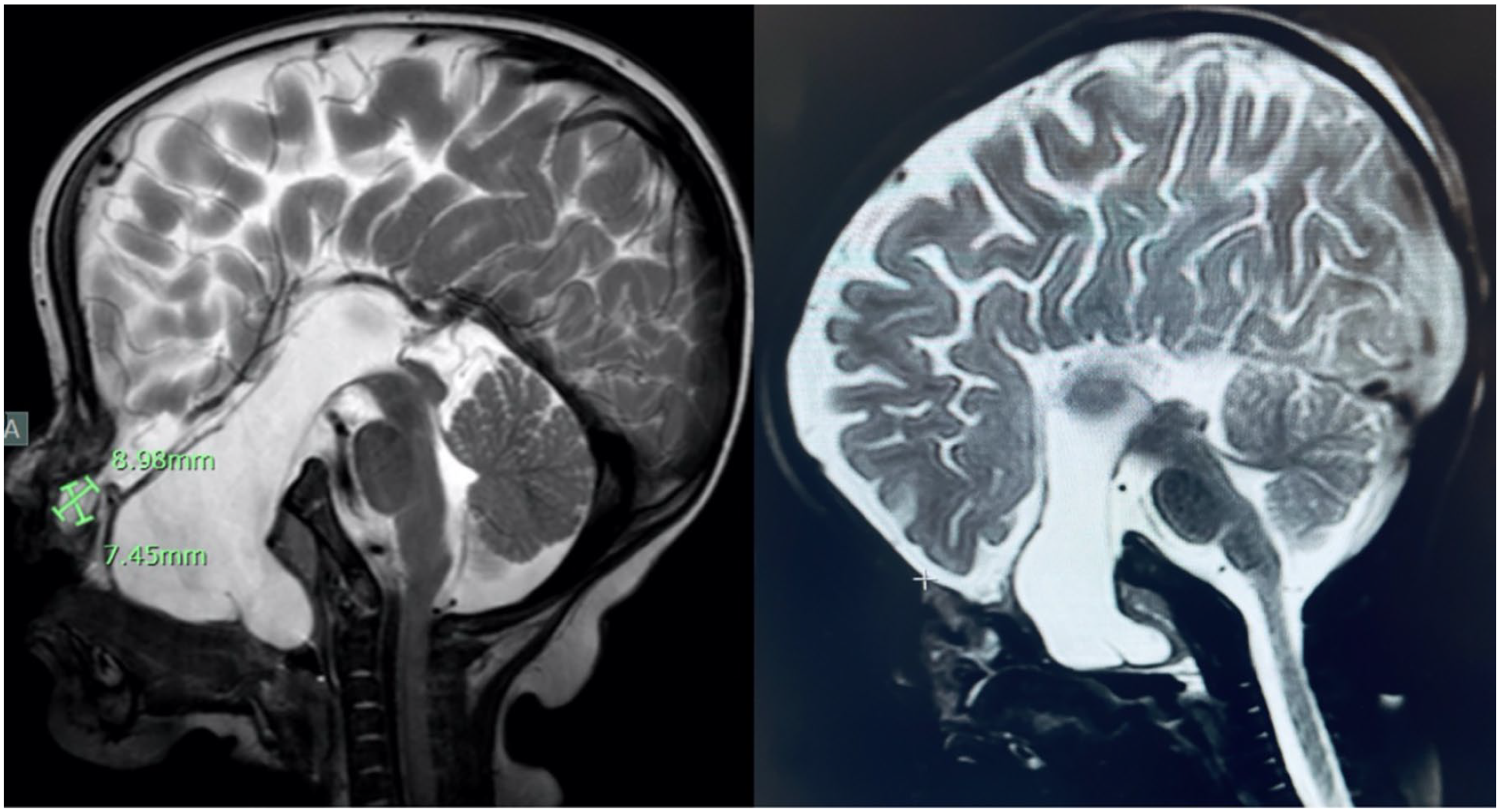
MRI of the meningoencephalocele at the skull base.
The meningoencephalocele was mobilized from the remnant of the hard palate and the premaxilla and pushed toward the skull base. The defect was covered with DuraGen, a collagen-based dural graft (Integra Life Sciences, Princeton, NJ, USA), and bilateral nasoseptal pedicled flaps. A foley catheter was then placed with a sedation protocol to bolster the area until scarring formed.
Oral maxillofacial surgery was consulted for the creation of an obturator to serve as a longer temporary measure to replace the foley catheter and fortify the skull base until permanent scar tissue formed. However, the obturator was not able to be created. Lack of more durable support for the repair of the skull base and inadequately developed scar may have contributed to the downward displacement of the meningoencephalocele after the removal of the Foley catheter. Given the displacement, the patient required an open bilateral frontal craniotomy with resection of the meningoencephalocele and placement of a resorbable plate to cover the skull base defect. A pericranial flap with DuraGen was used to reinforce the separation of the nasopharynx and oropharynx from the intracranial cavity.
Discussion
Meningoencephalocele is a rare congenital condition with an incidence of 1 in 5000 live births with the typical presentation of headaches, seizures, nasal obstruction, meningitis, and CSF rhinorrhea, sometimes associated with the rare Sakoda complex.1,2 Depending on the location of the meningoencephalocele, it can be visualized via sonography and classified as occipital, frontonasal, or basal, with different surgical approaches for each classification.3,4 The occipital meningoencephalocele is at the posterior fontanel, the frontonasal herniation is between the frontal and nasal bones and the basal protrusion is internally located along the skull base.
Characteristically, if meningoencephaloceles present with CSF leaks, they should be emergently managed to reduce the incidence of meningitis and seizures. 5 The mainstay operative management of meningoencephaloceles includes an open craniotomy with a pericranial flap or an alternative approach using a nasal septal flap via an endoscopic endonasal method. 5
Although open craniotomy is the traditional management of this condition, it is associated with over a 20% complication rate to the anterior skull base, including CSF leak, meningitis, intracranial hemorrhage, and pneumocephalus. 4 In adults, an endoscopic endonasal approach has been widely adopted, with successful closure rates of over 90%. Yet, in children, there has been a concern with the procedure’s feasibility due to the compact anatomy. 4 A study conducted by Thompson et al found that 14 of their patients, ages 2 months to 22 years, had successful endoscopic endonasal repair of the meningoencephaloceles with minimal complications, 1 patient developing a CSF leak, and 1 developing meningitis. 4 Accordingly, a study by Rawal et al. found that an endoscopic method had an 11.3% complication rate, with the most common manifestation being meningitis in 3% of their patients. 5 Yet, the researchers still believe that an endoscopic endonasal approach is an excellent method that provides a less invasive solution and can be considered a primary treatment approach.
For large skull base defects, the NSF has been a well-established method for covering the skull base area in adults. However, in the pediatric population, the small area of the nasal septum can pose a limitation to the repair. In a study by Shah et al, 6 pediatric patients who underwent endoscopic endonasal approaches to cover skull base defects with NSF were investigated. 6 The researchers observed that patients under 14 years of age experienced inadequate coverage of the defect and had subsequent CSF leaks. While patients over 14 years of age showed adequate coverage, as the septum in this age group is similar to that of adults.6,7 The researchers propose that the reduced effectiveness in the younger population is specifically due to larger defects compared to the flap size in anterior approaches reaching the cribriform plate.6,8
In contrast, Ghosh et al examined 16 pediatric patients with NSF reconstruction of skull base defects and found that all of their pediatric patients, regardless of age, had an equivalent success rate with the sufficient size of the NSF.7,9 One patient developed a CSF leak, but it was determined to be due to a secondary cause unrelated to the flap. 9 Similarly, Nation et al conducted a study of 8 pediatric patients under 6 years of age and found that using an NSF for the intraoperative repair of high-flow CSF leaks demonstrated adequate coverage of the defects with no postoperative CSF leaks. 10 Thus, these studies support the usage of the NSF in the pediatric population, stressing the importance of accurate preoperative measurements of the anterior skull base, surgical corridor, and nasal septal length to ensure proper coverage of the defect.
Conclusion
Congenital meningoencephalocele of the anterior skull base is a condition that typically requires early repair through an open craniotomy or a less invasive endoscopic approach. The endoscopic approach is increasingly adopted in the pediatric population due to its minimally invasive nature and lower complication rate. However, this technique may not always be possible if the anatomy of the area is too compact. Therefore, treating meningoencephaloceles or the skull base defect requires understanding the etiology, position, and reconstruction options before committing to an operative technique.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Submission Statement
This article is original and has not been submitted elsewhere in part or whole.