
Abstract
Objective:
Nasal septal perforation (NSP) repair is challenging surgery considered in patients with symptomatic NSP intractable to conservative treatments. This study aimed to assess the success rate and identify factors affecting the surgical outcome of NSP by analyzing consecutive series of NSP repairs by a single surgeon.
Methods:
We enrolled 84 patients diagnosed with NSP and who underwent surgical repair of NSP by a single surgeon (Y.J.J.) between November 2007 and July 2022. Medical records were retrospectively reviewed regarding variables involving preoperative symptoms, rhinologic history, etiology, surgical techniques, and the outcome of surgery. In addition, features of NSP were objectively evaluated using computed tomography scans.
Results:
The overall success rate of NSP repair was 64.3% (54 of 84). Nasal obstruction (79.8%), crusting (34.5%), and epistaxis (27.4%) were frequent preoperative symptoms. Iatrogenic injury from previous nasal surgery (70.2%) was the most common cause. The average size of NSP on preoperative CT was 9.53 ± 6.68 mm. Patients with incomplete NSP closure had significantly larger perforations (12.21 ± 7.92 mm) than those with successful closure (8.04 ± 5.41 mm) preoperatively (P = .005). Patients with smoking history (OR = 2.971, 95% CI 1.170-7.548, P = .020) and NSP repair with combined rhinoplasty (OR = 3.811, 95% CI 1.401-10.370, P = .007) were more likely to experience incomplete closure. Patients whose perforations were reinforced with interposition graft were more likely to result in successful repair (OR = 6.752, 95% CI 2.496-18.262, P < .001). The bilaterality of mucosal flap coverage, surgical approach, types of mucosal flap and interposition graft, perforation shape, mucosal thickness around perforation, and distance from the nasal floor were not significantly related to the surgical outcome.
Conclusions:
Significant factors affecting the outcome of NSP repair were patient’s smoking status, combined rhinoplasty, application of interposition graft, and perforation size.
Introduction
Nasal septal perforation (NSP) is an anatomical defect in any portion of the nasal septum along with bilateral septal mucosa. 1 Its causes can be classified as iatrogenic from nasal surgeries, trauma, inflammatory, infectious, neoplastic, and caustic. 2 Conservative management for symptomatic patients focuses on the restoration of nasal hygiene including nasal irrigation with normal saline, ointment application, or temporary closure by nasal septal button,3,4 but if symptoms persist and the defect worsens, surgical repair of NSP is inevitable.5-8
The goals of the elective surgical repair of NSP are to provide the most tension-free closure as much as possible using vascularized mucosal flaps and to restore normal nasal function.9,10 Successful repair of NSP is difficult and challenging, even for experienced rhinology surgeons. Various surgical techniques have been introduced in the literature over the years, but the treatment for NSP is yet to be standardized and the reported success rate of the closure varies from 52% to 100% depending on the surgeons.4,5,11,12 According to previous studies, the size of NSP, bilaterality of flap coverage, and interposition graft materials have been suggested as possible determinants for surgical outcomes.3,4,12-15 However, most of the previous studies are collective case series performed by multiple surgeons, and comprehensive analysis on the influence of variables during the surgical processes involving surgeon’s factors, patient’s factors, surgical techniques, and NSP status lacks.
As a tertiary care center performing NSP repair, we got impression during the surgical procedures that there might be other possible factors related to the surgical outcome. For example, revision cases which already had failed from primary surgical treatment or cases with combined rhinoplasty seemed to have lower complete closure rate. Moreover, status of NSP such as perforation shape, mucosal thickness around the perforation, and perforation’s distance from the nasal floor seemed to be related to the successful closure of NSP. We presumed that vertical dominant perforation, perforation with thin circumferential mucosa (especially posterior portion’s mucosa), or perforation close to the nasal floor are more difficult to repair. Therefore, we considered that it is meaningful to comprehensively analyze previously reported factors and our newly suggested factors altogether. In the present study, we aimed to (1) review the success rate of NSP repair in our institution performed by a single surgeon (Y.J.J.) over 15 years and (2) elucidate significant factors affecting the outcome of NSP repair with our consecutive cases.
Materials and Methods
Study Population
In this study, we enrolled patients who underwent surgical repair of NSP regardless of conservative treatments between November 2007 and July 2022 at Asan Medical Center (AMC). We retrospectively analyzed their medical records. All patients underwent detailed history taking, serologic test, endoscopic examination. Computed tomography (CT) scan was performed to patients who had signs of combined septal deviation, external nose deviation, sinusitis, or mucosal problems for comprehensive preoperative evaluation of the paranasal sinuses and nasal cavity. Conservative treatment involving normal saline irrigation and ointment application was maintained for at least 3 months before the decision of the surgical intervention.
We identified 131 patients diagnosed with NSP. Of them, 47 patients were excluded based on the exclusion criteria: (1) no history of preoperative CT evaluation; (2) lack of postoperative outpatient follow-up; and (3) inadequate information about the surgical procedures in the operation record. Finally, 84 patients with NSP were included in the analysis; their demographic and clinical characteristics are listed in Table 1.
Patient Characteristics and Univariate Analysis of Variables.
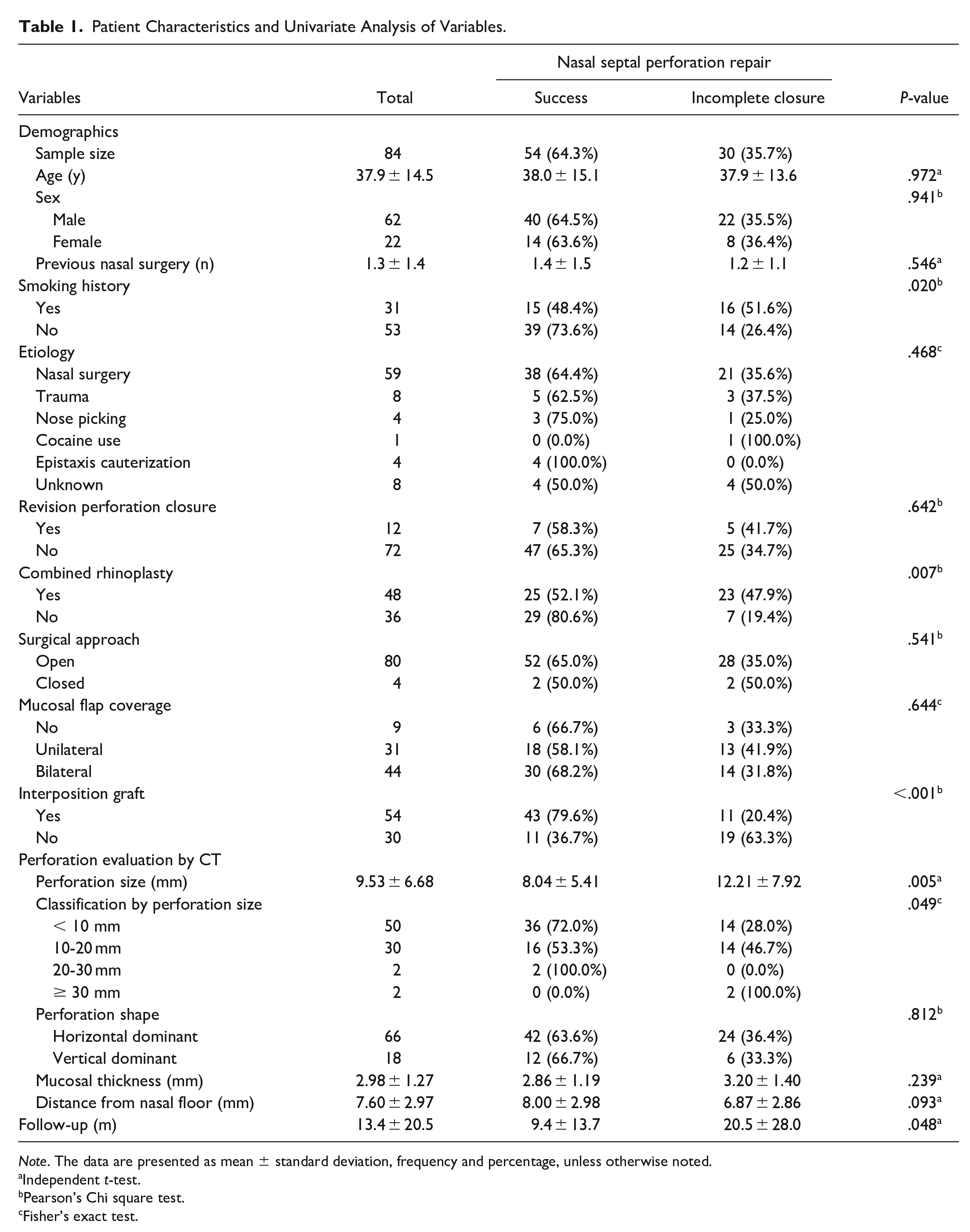
Note. The data are presented as mean ± standard deviation, frequency and percentage, unless otherwise noted.
Independent t-test.
Pearson’s Chi square test
Fisher’s exact test.
This study was approved by the Institutional Review Board of AMC (IRB no.: 2022-0258) and performed in accordance with the tenets of the Declaration of Helsinki. The IRB waived the requirement for informed consent considering the low risk associated with a retrospective review of data.
Variables
The preoperative variables included age, sex, history of previous nasal surgery, smoking status, etiology of NSP at diagnosis, and preoperative symptoms. The intra- and postoperative variables included the surgical approach, use of mucosal flap coverage or interposition graft, types of mucosal flap technique or interposition graft, postoperative symptomatic changes, and follow-up period. Surgical methods were decided by the author (Y.J.J.) and tailored to each patient based on preoperative evaluation of NSP considering various factors such as size and location of NSP, status of nasal mucosa around NSP, and existence of septal deviation or external nose deviation. NSP was objectively evaluated through preoperative CT scan by measuring the size of the perforation, mucosal thickness around the perforation, and distance from the nasal floor.
Parameters in CT analysis were manually measured by the author (H.A.J.) using the caliper tool of the DICOM viewer; this author was blinded to the medical history of the patients during the measurement. The horizontal length of a NSP was measured in axial images of CT (Figure 1A), and the vertical length of a NSP was measured in coronal images of CT (Figure 1B). Subsequently, the perforation size was defined as the longer dimension between 2 measured lengths. The shape of perforation was defined depending on which diameter was larger between horizontal and vertical lengths. Mucosal thickness around the NSP was measured at posterior mucosa within 5 mm of the perforation in axial images of CT (Figure 1C). Distance from the nasal floor was measured from the most inferior border of a perforation to the midpoint of the nasal floor in coronal images of CT to evaluate the height of NSP (Figure 1D).
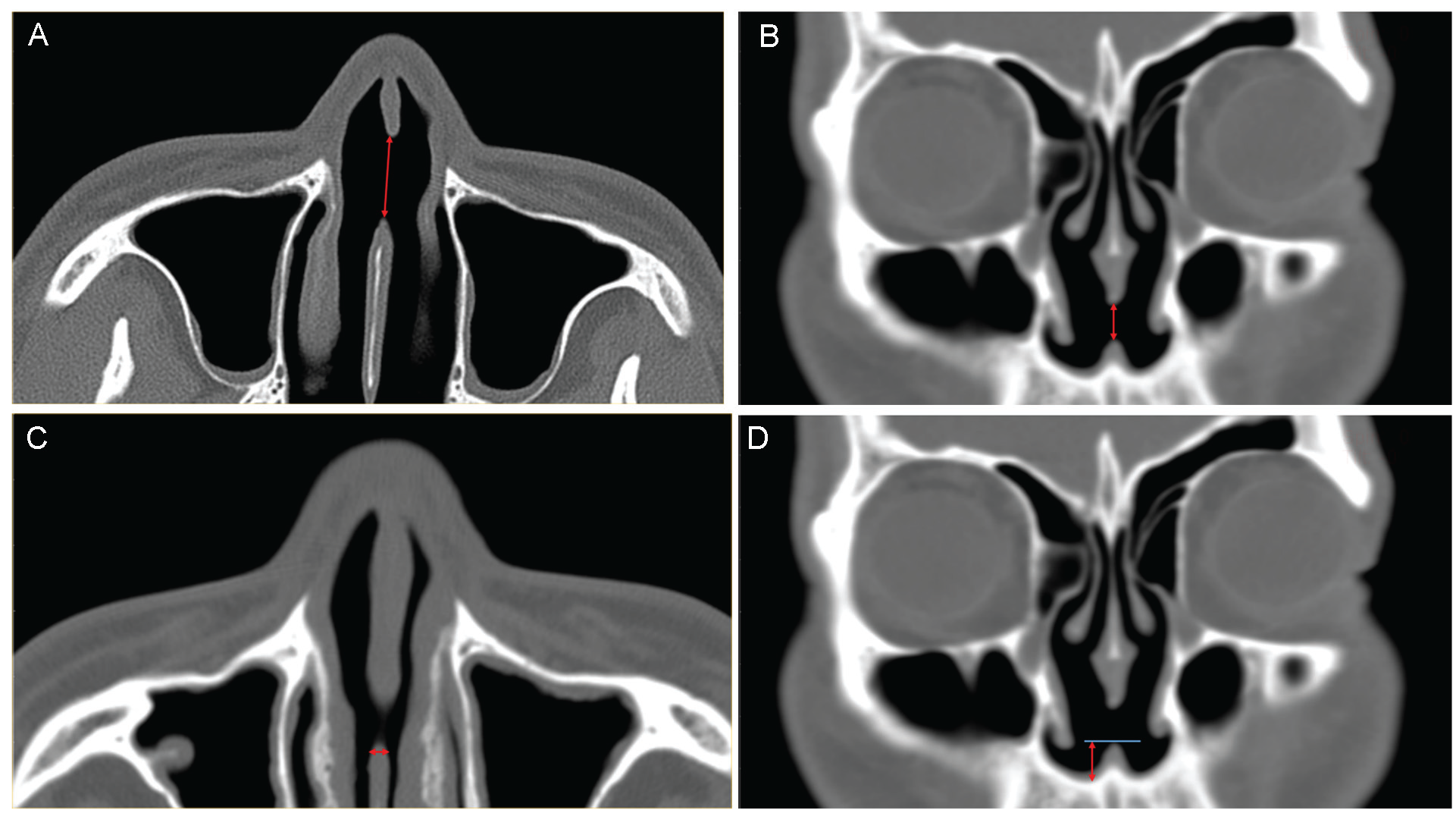
Parameters of nasal septal perforation (NSP) evaluated through preoperative computed tomography scan. (A) horizontal length of NSP in axial image. (B) vertical length of NSP in coronal image. (C) mucosal thickness at the posterior mucosa of NSP. (D) distance from the nasal floor to inferior border of NSP.
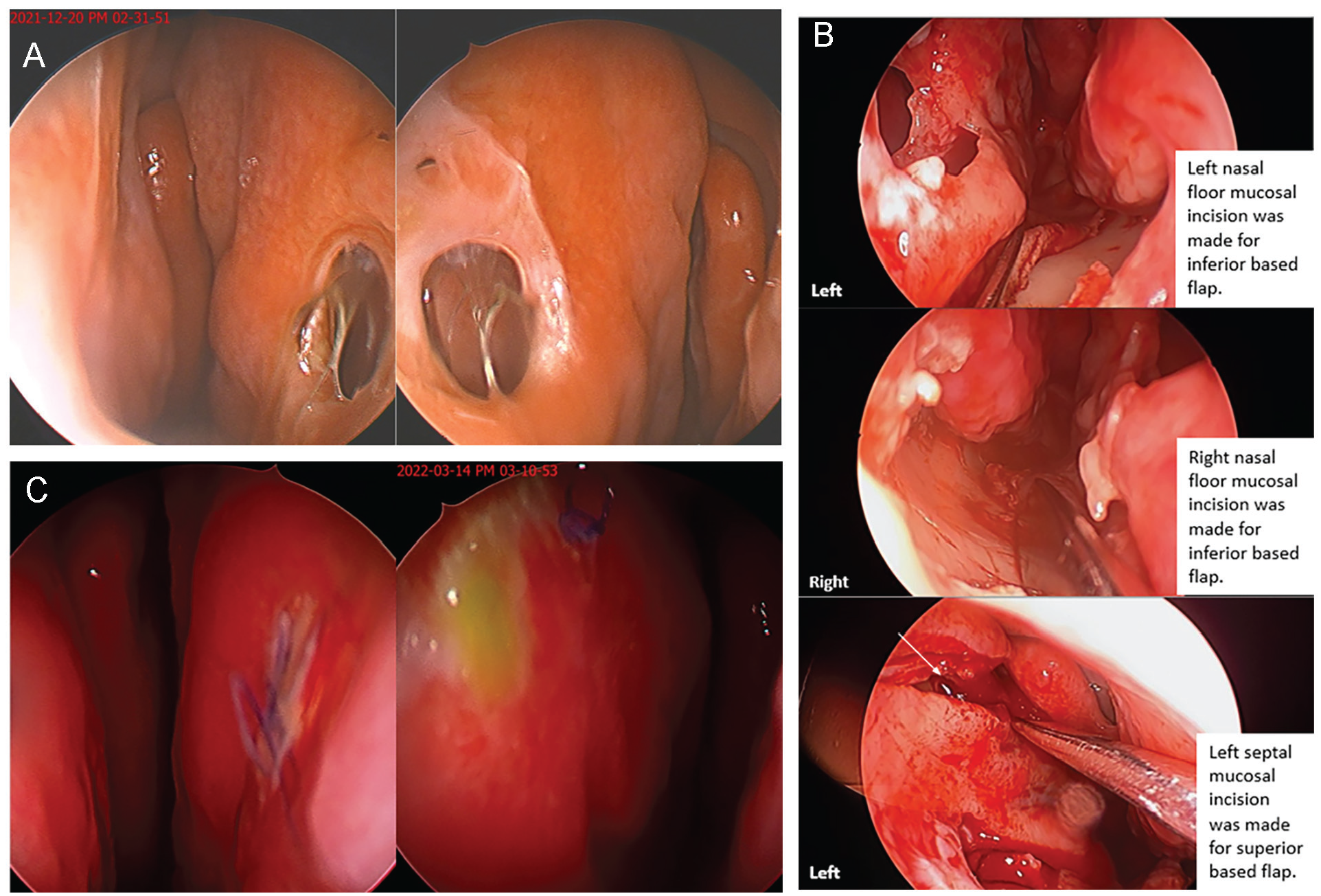
A case of NSP repair in a 43-year-old woman. A patient with history of rhinoplasty visited our clinic due to known NSP with symptoms of nasal obstruction, bloody crust, and whistling which was intractable to conservative treatment. (A) Preoperative endoscopic view of NSP. (B) Intraoperative endoscopic view of NSP repair. Bilateral mucosal flap was elevated including nasal floor mucosa. Left side perforation was closed using bipedicled advancement flaps (superior and inferior based flaps). Right side perforation was closed using inferior based unilateral advancement flap. (C) Postoperative endoscopic view with successful NSP repair.
The main outcome of the present study was the success of NSP closure evaluated during the outpatient follow-up visit. Operation sites were evaluated by nasal endoscopy at every outpatient visit to confirm incomplete NSP closure and subjective improvement of patient’s NSP related symptoms was assessed. The success rate of NSP repair at the last follow-up visit was primarily evaluated, and variables related to the success were statistically analyzed. Patients who underwent revision surgery due to incomplete NSP closure were also counted.
Statistical Analysis
Continuous variables were presented as mean or median with standard deviation (SD), while discrete variables were presented as frequency and percentage. The statistical analysis was performed using SPSS software version 24.0 (IBM Corp., Armonk, NY, USA). P value less than .05 was considered statistically significant.
Regarding univariates, relevance with the success of postoperative NSP repairs were analyzed using the independent t-test for continuous variables. Categorical variables were analyzed using Pearson’s Chi square and Fisher’s exact test. The model’s significance was reported as odds ratio (OR) with 95% confidence intervals (CI).
Results
We enrolled 84 patients with NSP (62 male [73.8%], 22 female [26.2%]; mean age, 37.9 ± 14.5 years; mean postoperative follow-up period, 13.4 ± 20.5 months). The main preoperative symptoms included nasal obstruction (79.8%), crusting (34.5%), epistaxis (27.4%), postnasal drip (20.2%), nasal pain (20.2%), whistling (19.0%), and parosmia (3.6%). Regarding the etiology of NSP, iatrogenic injury while undergoing a previous nasal surgery was the most common cause (70.2%). Other causes were nasal trauma (9.5%), cauterization of epistaxis (4.8%), nose picking habitus (4.8%), and cocaine use (1.2%). In 8 cases (9.5%), the etiologies remained unclear despite an effort to find out the cause. Among patients with previous nasal surgery experience, patients had mean of 1.3 ± 1.4 times of surgery including septoplasty, rhinoplasty, or turbinoplasty. Of the 84 cases, 12 cases (14.3%) were revision NSP repair patients who already had failed primary NSP repair from other institutions, and 48 cases (57.1%) underwent combined simultaneous rhinoplasty for the correction of the external nose and septal deviation, and augmentation.
Status of NSP was evaluated through preoperative CT scans, and the average size of the perforation was 9.53 ± 6.68 mm. Most of the patients (50 of 84, 59.5%) had perforations smaller than 10 mm, 30 patients (35.7%) had perforations between 10 and 20 mm, while 4 patients (4.8%) had large-sized perforations more than 20 mm. Most of perforations were horizontal dominant shape (66 of 84, 78.6%). The mean mucosal thickness which was measured at the posterior border of NSP was 2.98 ± 1.27 mm. The mean distance from the nasal floor to the NSP inferior border was 7.60 ± 2.97 mm.
In regard of the surgical technique, most of the cases (80 of 84, 95.2%) were repaired via the open approach. Depending on the size and location of the perforations, we used various mucosal flaps and interposition grafts, and these are demonstrated in Table 2 with the rate of successful NSP closure. The perforation was covered bilaterally with mucosal flaps for 44 patients (52.4%) and simply unilaterally in 31 patients (36.9%) expecting spontaneous mucosal healing of the uncovered side. The unipedicle advancement flap was the most repeatedly used (35 cases), followed by the bipedicle advancement flap (20 cases) and rotational flap (12 cases). Regarding interposition grafts, 54 of 84 cases used the interposition grafts during the repair. The most repeatedly used graft materials were septal bone or cartilage (18 cases) and fascia lata allograft (18 cases), followed by perichondrium (12 cases), skin graft (4 cases), and conchal cartilage (2 cases). A skin graft was placed at a unilateral mucosal defect that could not be fully closed with a mucosal flap advancement. The graft was designed to fit tightly into the defect, minimizing the amount of epithelial layer that was buried. There were no statistical differences in success rate of NSP repair among mucosal flaps (P = .102) and interposition graft types (P = .096). No intra-operative complications occurred in any cases.
Types of Mucosal Flap Technique and Interposition Graft Used in the Repair of Septal Perforation With the Rate of Successful Closure.
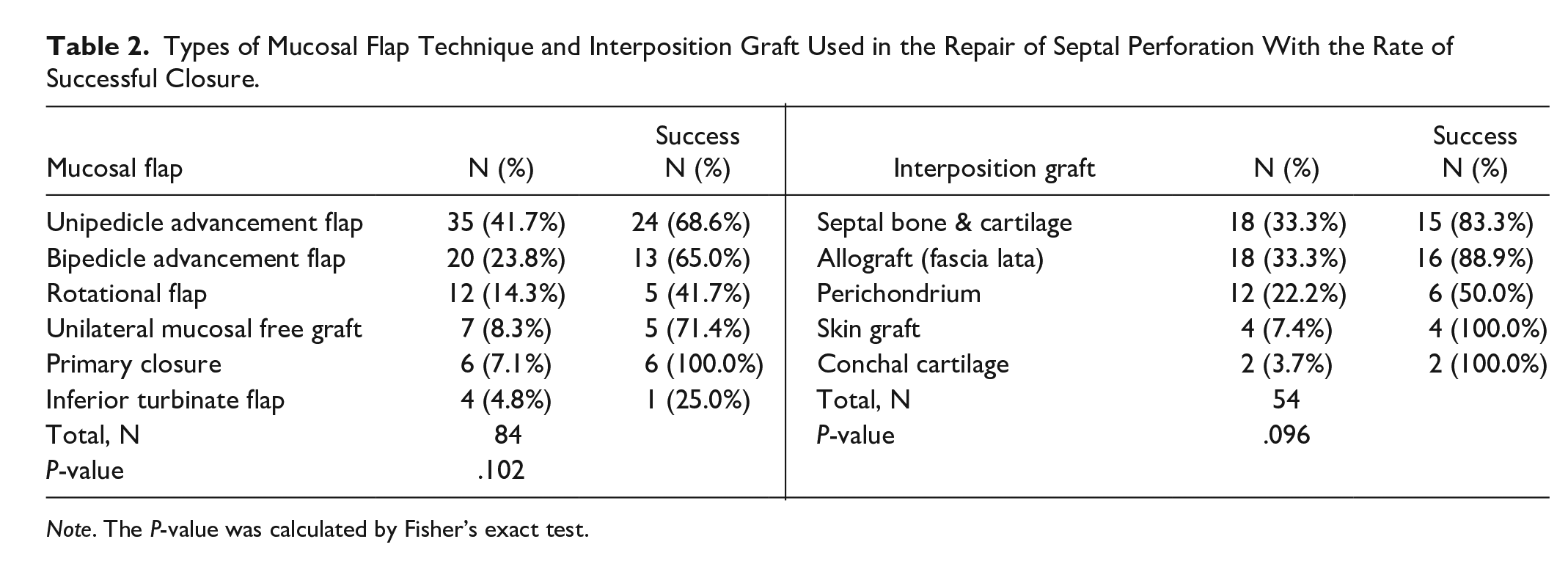
Note. The P-value was calculated by Fisher’s exact test.
The overall success rate of NSP repair for complete closure in AMC was 64.3% (54 of 84). All of the patients with successful NSP closure experienced resolution of NSP related symptoms such as epistaxis or crusting. Among 30 patients who experienced reperforation after the surgery, 5 patients decided and underwent revision NSP repair surgeries, but the perforations were finally not closed even after the revision surgery in 4 patients. Other patients with incomplete closure who did not undergo the revision surgery had gradual relief from previous chief nasal symptoms postoperatively or were lost to follow-up. Despite incomplete NSP closure, 53.3% (16 of 30) of patients reported subjective improvement of NSP related symptoms compared to the preoperative status with remnant pinpoint-sized perforation.
In univariate analysis to investigate significant variables related to the success of the perforation closure, smoking status (P = .020), combined rhinoplasty (P = .007), use of interposition graft (P < .001), and perforation size (P = .005) were statistically significant. There was a significant difference in the follow-up period between the success and reperforation groups (P = .048), and significantly long follow-up was required in patients with reperforation. Smokers were more likely to experience incomplete perforation closure after NSP repair than non-smoking patients (OR = 2.971, 95% CI 1.170-7.548, P = .020). NSP repair with combined rhinoplasty had higher reperforation rate than single NSP repair (OR = 3.811, 95% CI 1.401-10.370, P = .007). NSP repair with the use of interposition graft was more likely to result in successful repair (OR = 6.752, 95% CI 2.496-18.262, P < .001). Regarding perforation size, patients with incomplete closure had significantly larger perforations (12.21 ± 7.92 mm) than those with successful closure (8.04 ± 5.41 mm) preoperatively (P = .005).
Differently from our previous assumption, revision surgery was a statistically insignificant factor. Twelve revision repair cases had higher reperforation rate (41.7%) than primary cases (34.7%), but there was no significant difference (P = .642). Bilaterality of mucosal flap coverage, surgical approach, and parameters evaluated on CT involving perforation shape (horizontal or vertical dominant), mucosal thickness around the perforation and distance from the nasal floor were not statistically significant variables, either.
Discussion
Our study analyzed the results of NSP repair which were performed over 15 years by a single surgeon (Y.J.J.). In this study, the success rate of NSP repair was 64.3%. We demonstrated that patient’s smoking status can affect wound healing process and combined performance of rhinoplasty can increase the likelihood of incomplete perforation closure. In addition, small perforation and application of interposition graft were more likely to have good surgical prognosis. In analyzing our study’s NSP success rate, following points should be taken into account. As our center is a tertiary referral hospital, 14.3% of patients were revision cases who had already failed NSP repair from previous treatments at other institutions with difficult and complex status to be completely cured. Moreover, 40.5% of patients had perforations larger than 10 mm, and 57.1% of patients underwent rhinoplasty together to fulfill their esthetic desires.
Patients with smoking history showed significant high incomplete NSP closure rate in our study. Cetiner et al 16 demonstrated that both nasal recovery time and development of NSP were significantly greater in smokers than those in non-smokers after septoplasty. Cigarette smoke induces intimal fibrosis of vessel and especially nicotine causes vasoconstriction affecting microcirculation of mucosal flaps. The carbon monoxide in smoke leads to tissue hypoxia by decreasing the efficiency of dissociation of oxygen from hemoglobin. 17 Cilia of respiratory nasal mucosa is also negatively affected by exposure to smoke. 18 As these changes may considerably affect the healing process postoperatively and compromise nasal defense mechanisms, we suggest cautious and careful postoperative follow-up is required in smokers.
In addition, patients with combined rhinoplasty had significant higher reperforation rate than patients with NSP repair alone in this study. We thought that this may be due to conservative mucosal flap elevation to cover the perforation along with various grafting of cartilage and bone during rhinoplasty procedures. As aggressive mucosal flap elevation can be the source of retrograde infection to graft materials, there seems to be a tendency of modest dissection and this might affect success rate of NSP repair. Whether to perform 2-stage operation or not should be carefully discussed with patients preoperatively considering pros and cons.
Regarding interposition grafts which were another crucial factor in our study, several studies reported that grafts have certainly beneficial effect in NSP repair regardless of the type of materials.5,9,13,19 Using interposition grafts can help to avoid excessive tension and serve as a scaffold for mucosal migration and regeneration during the healing process. In addition, grafts serve as barriers between repaired flaps and prevent mucosal flaps from shrinkage. 11
Size of NSP which is an already well known factor was also statistically significant in our study. In a systematic review of NSP repair, the surgical success for large perforations (>2 cm) was approximately 78%, whereas small-to-moderate perforations were completely closed in about 93% of patients (P < .001). 4 The size of NSP is inversely proportional to the amount of mucosa available for perforation closure and relative size of NSP compared with the whole septum is thought to be more important than the absolute size.
Other factors of NSP status like perforation shape (horizontal or vertical dominant), posterior mucosal thickness around the perforation, or distance from the nasal floor measured through CT scans which we first assumed as possible important factors affecting surgical outcome were not statistically significant. In previous studies, the vertical height of a perforation has been envisioned to play a more important role in the surgical outcome than the horizontal length because a main tension between the nasal floor and the dorsum was found to be critical. 13 However, there was no significant outpowering between horizontal and vertical dimensions in our study. As most of the cases were repaired via open approach, we consider that it was possible to elevate and rotate enough mucosal flaps in vertical direction. We also analyzed mucosal thickness of NSP because we got an impression during the surgical procedures that mucosa around the perforation is usually not full-thickness mucosa and barely healed tissue without enough integration. Especially, posterior mucosa of the perforation seemed to be more vulnerable and insecure than anterior portion, and handling this portion is difficult but critical for the complete closure. Moreover, in case of NSP which locates close to the nasal floor, space for elevating enough mucosal flap inferior to the perforation is quite restricted and wider dissection of nasal floor is necessary. Mucosa of the nasal floor is usually thinner than septal mucosa, and mucosal tear during the dissection often occurred at angular transition portion which connects septal mucosa and nasal floor mucosa. For this reason, we considered distance from the nasal floor to NSP might be a potential factor affecting surgical outcome, but further analysis is required. Rather than the perforation’s circumferential mucosal thickness or location, adequate mobilization of vascularized mucosal flaps for tension-free closure and application of strong interposition graft which is sufficiently larger than the diameter of the perforation seem to be more crucial.
Our findings are noteworthy and may assist the decision-making process of NSP repair because we comprehensively analyzed various factors of surgical process altogether. Moreover, several perforation-related parameters were evaluated with accurate and objective measurement through patients’ preoperative CT scans, while most of the previous studies roughly measured the perforation size using a ruler during the operation. Traditional measurement of NSP through endoscopy or ruler is also good enough to measure the defect, but we wanted to propose new analysis through CT scan with less errors. This study also included cases of NSP repair with various surgical techniques and grafts, not only by a single uniform technique.
Still, there are some limitations in this study. Because of the retrospective design, there might be some biases in interpreting our results. Follow-up periods were different per patient and there was a significant difference in follow-up periods between the success and incomplete closure groups. Also, postoperative improvement of NSP related nasal discomfort was evaluated subjectively by patient’s reports. There may be unreported reperforation or complications which occurred after the last outpatient follow-up visit. Further studies with a larger population, multi-ethnic analysis, and long-term follow-up are needed in the future.
Conclusions
The overall success rate of NSP repair in AMC over 15 years was 64.3% for complete perforation closure. Significant factors affecting the outcome of NSP repair were patient’s smoking status, combined rhinoplasty, application of interposition graft, and perforation size. Preoperative analysis and consideration of these factors can help decision-making process of NSP repair.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.