
Abstract
Woakes’ syndrome, first reported by Edward Woakes in 1885, is an extremely rare, recurrent sinonasal polyposis leading to bone erosion of the sinus walls with consequent nasal pyramid deformity and facial disfigurement. We report a 66-year-old man who presented with severe nasal obstruction. His external nose was deformed and distended with complete obstruction of the bilateral nasal cavities by nasal polyps. The normal structure of the nose was disrupted. Thus, super-selective embolization was performed before surgery to minimize bleeding. The day after the embolization, polypectomy was performed with the navigation system. The progression was uneventful, and the patient was discharged on postoperative day 7. Pathological examination revealed inflammatory polyps with no eosinophil infiltration. Thus, we diagnosed it as Woakes’ syndrome. Although there have been few reports of Woakes’ syndrome in the past, these are the largest polyps reported to the best of our knowledge.
Introduction
Woakes’ syndrome, first reported by Woakes in 1885, 1 is an extremely rare, recurrent sinonasal polyposis leading to bone erosion of the sinus walls with consequent nasal pyramid deformity and facial disfigurement.
Woakes’ syndrome has four characteristics. 2 First, bilateral nasal polyps develop in the middle meatus during childhood. Second, it causes necrosing ethmoiditis. Third, the hypertrophic process is characterized by nasal pyramid deformation. Finally, treatement failure occurs with constant and rapid recurrence.
Only few cases of Woakes’ syndrome have been reported in the literature. Herein, we report a case of Woakes’ syndrome with a large nasal polyp.
Case Report
A 66-year-old man with severe nasal obstruction visited our department. Symptoms had begun with nasal polyp when he was 20 years old; however, it went untreated because he hated going to the hospital. The patient did not mention a similar family history of nasal polyposis. He had no other relevant history and aspirin intolerance.
On presentation, his external nose was deformed and distended with complete obstruction of the bilateral nasal cavities by nasal polyps. The polyps were large and protruded through the anterior nostrils (Figure 1a). They were red and bled easily when punctured using a needle. Moreover, anosmia was determined using intravenous olfaction test with Alinamin F. Computed tomography revealed complete obstruction of all paranasal sinuses with normal bony anatomy of the external nose (Figure 2). Moreover, bilateral conductive hearing loss due to otitis media with effusion was observed.

Patient’s facial appearance before and after surgery. (a) Before surgery. Large polyps protruding through the anterior nostrils and the mouth is open for breathing. (b) After surgery. He can breathe through his nose and is able to close his mouth.
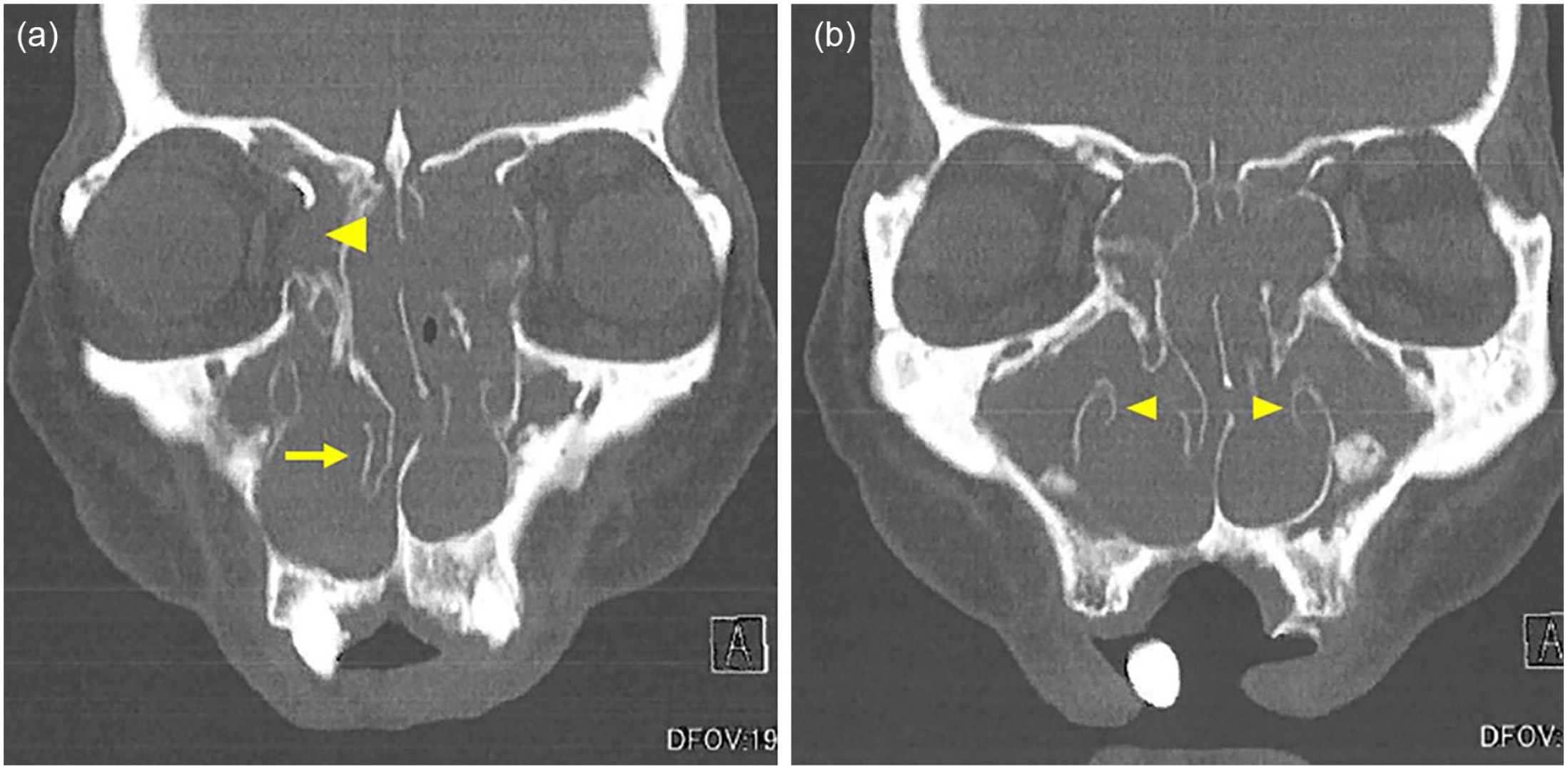
Computed tomography revealing polyp filling and disruption of normal structure. (a) The right infraorbital wall is missing (arrow head) and the right middle turbinate is thickened and shifted medially (arrow). (b) The bilateral inferior turbinates are externally compressed and atrophic (arrow head).
Oral steroids had no effect on polyp reduction. We planned surgery under general anesthesia for nasal polypectomy; however, super-selective embolization was performed before surgery to minimize bleeding. Angiography revealed that the polyps were slightly stained. Super-selective embolization was performed using a microcoil introduced into the distal branch of the maxillary artery. The day after the embolization, the polypectomy was performed under general anesthesia. The polyps were large in volume with abnormal structure of the nasal sinuses. The bilateral inferior turbinates were externally compressed and atrophic; middle turbinates showed polypoid degeneration, and the right infraorbital wall was missing. The posterior nostrils were obstructed by multiple polyps.
The surgery was completed without complications in 2 h and 55 min, with a blood loss of 300 mL. The nasal packing was removed on postoperative day 5, with no evidence of active bleeding. The progression was uneventful, and the patient was discharged on postoperative day 7. The nasal obstruction has improved since then (Figure 1b). During surgery, the right, left anterior, and posterior nasal polyps were submitted to pathology, and all were inflammatory polyps without eosinophil infiltration (Supplemental Figure 1).
Ethical approval was obtained from the Institutional Review Board Committee at Juntendo University Hospital Clinical Research and Trial Center before beginning the study (approval number: 2023-001). Written informed consent was obtained from the patient for the publication of this case report and accompanying images.
Discussion
Woakes’ syndrome is characterized by an external nasal deformity. When Woakes’ syndrome is suspected, a differentiation should be made between cancer or papilloma. Furthermore, Woakes’ syndrome should be considered as a differential diagnosis of eosinophilic chronic rhinosinusitis; however, eosinophil infiltration is not seen in Woakes’ syndrome as in the present case. The treatment is surgery, as the polyps do not shrink with steroids due to its different pathogenesis than that of eosinophilic sinusitis.
Normally, a few patients with nasal polyps develop nasal pyramid deformities. It remains unclear why some patients with nasal polyps develop deformation of the nasal pyramid, whereas most show deformity confined to the paranasal sinuses. In our case, the normal structure of the nose was disrupted; therefore, surgery was performed with caution.
Most cases of Woakes’ syndrome occur in children and young adults because of the plasticity of bony facial structures. 3 The precise etiology is unknown; however, heredity appears to be a potential contributing factor. 4 In contrast, in our patient, nasal polyp started in his 20s, and the actual treatment did not begin until he was 66 years old.
Of the few reports of Woakes’ syndrome, this is the largest polyps ever reported. The treatment of Woakes’ syndrome, in which normal structures are disrupted, should be performed carefully using a navigation system.
Supplemental Material
sj-jpg-1-ear-10.1177_01455613231186473 – Supplemental material for A Case of Woakes’ Syndrome With A Bilateral, Large Nasal Polyp
Supplemental material, sj-jpg-1-ear-10.1177_01455613231186473 for A Case of Woakes’ Syndrome With A Bilateral, Large Nasal Polyp by Shori Tajima, Katsuhisa Ikeda and Fumihiko Matsumoto in Ear, Nose & Throat Journal
Footnotes
Acknowledgements
We are grateful to H. Oishi and T.Fujii for performing super-selective embolization. We also thank T.Kanaya for consulting us to the present rare case. This work was supported by JSPS KAKENHI (Grant-in-Aid for Early-Career Scientists) Grant Number JP22K16934.
Author Contributions
S.T. wrote the paper with support from F.M. and K.I. All authors reviewed the manuscript.
Data Availability statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.