
Abstract
The prevalence of primary hyperparathyroidism (PHPT) is increasing as routine laboratory testing for calcium and parathyroid hormone becomes more prevalent due to heightened awareness of the disease. PHPT affects multiple organ systems including the cardiovascular system. This case report highlights a patient with first degree atrio-ventricular block pre-operatively that resolved after resection of her parathyroid adenoma. This case emphasizes the importance of treating asymptomatic hyperparathyroidism to optimize cardiac function.
Introduction
Primary hyperparathyroidism is a common condition, affecting approximately 1 in 500 women and 1 in 2000 men annually. 1 The measured prevalence of the disease has increased due to greater surveillance of calcium levels in the population and increased physician awareness of the condition. It is a disease process that affects multiple organ systems, including the bones, kidneys, gastrointestinal system, central nervous system, and the cardiovascular system. Its effects on the cardiovascular system are well known, but they often go unrecognized by the patient. We report a case in which a patient with first-degree atrio-ventricular block had immediate reversal of her arrhythmia and conversion to normal sinus rhythm intra-operatively after removal of her parathyroid adenoma.
Case Report
A 55-year-old female was noted by her primary care physician to have an elevated serum calcium level of 10.6 mg/dl. Subsequent work-up revealed an inappropriately elevated parathyroid hormone (PTH) level of 68 pg/ml, leading to a diagnosis of primary hyperparathyroidism. Pre-operative localization studies were performed, consisting of a nuclear medicine scan as well as a neck ultrasound. Both suggested the presence of a left parathyroid adenoma. The patient was counseled regarding the risks and benefits of parathyroid surgery, and she signed informed consent to undergo a minimally invasive parathyroidectomy.
Pre-operatively, the patient was noted to have first degree atrio-ventricular block, with the P-R interval on her ECG being delayed at 0.28 seconds. She was otherwise asymptomatic and did not have any complaints of chest pain nor shortness of breath. In the operating room, she was noted to have a 2 cm left inferior parathyroid adenoma which weighed 2.20 g. Pre-operative rapid PTH assay was performed and measured 93 pg/ml. The parathyroid adenoma was subsequently removed and a PTH assay was drawn 10 minutes after tumor removal. The patient’s PTH level had normalized at 32 pg/ml. Approximately 10 minutes after tumor removal, the anesthesiologist noted that the patient’s ECG rhythm had now converted to a normal sinus rhythm with normalization of the P-R interval to 0.16 seconds. The operation was completed and the patient was extubated and tolerated the procedure without complications (Figures 1 –4).
Histopathology
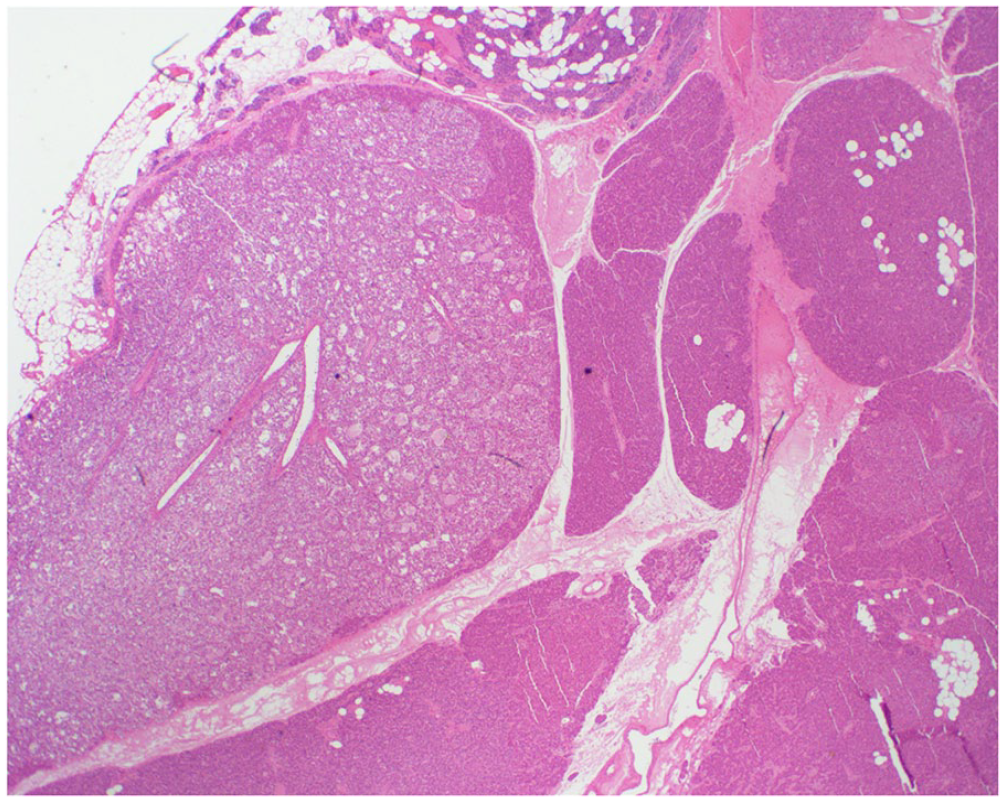
Low power (4X) showing compressed non-neoplastic parathyroid with abundant fat next to nodules of parathyroid adenoma showing a marked reduction in fat.
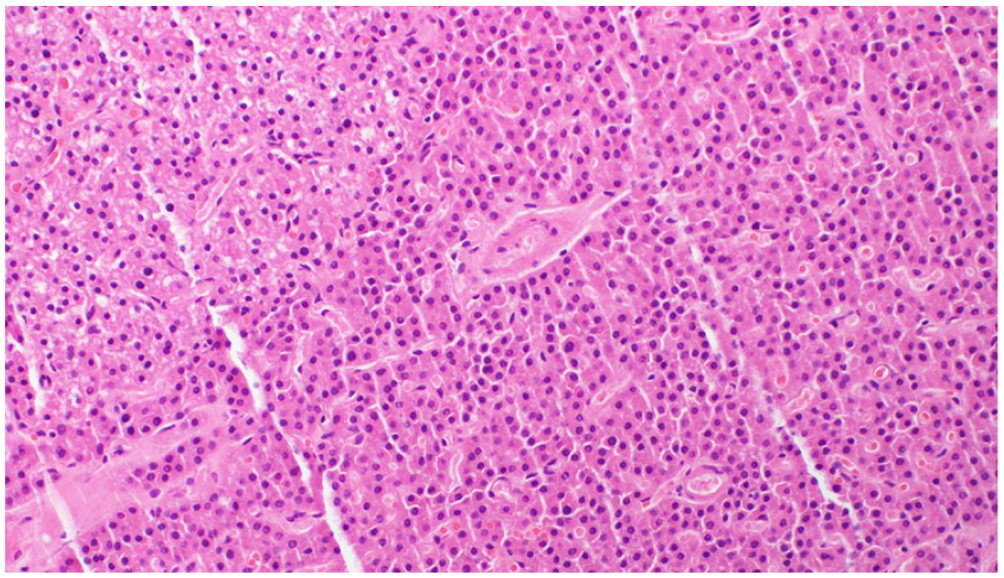
High power (40X) showing solid nests of cells as well as crowded small glandular structures. The cells are uniform with round nuclei and abundant eosinophilic cytoplasm, consistent with oncocytic cells.
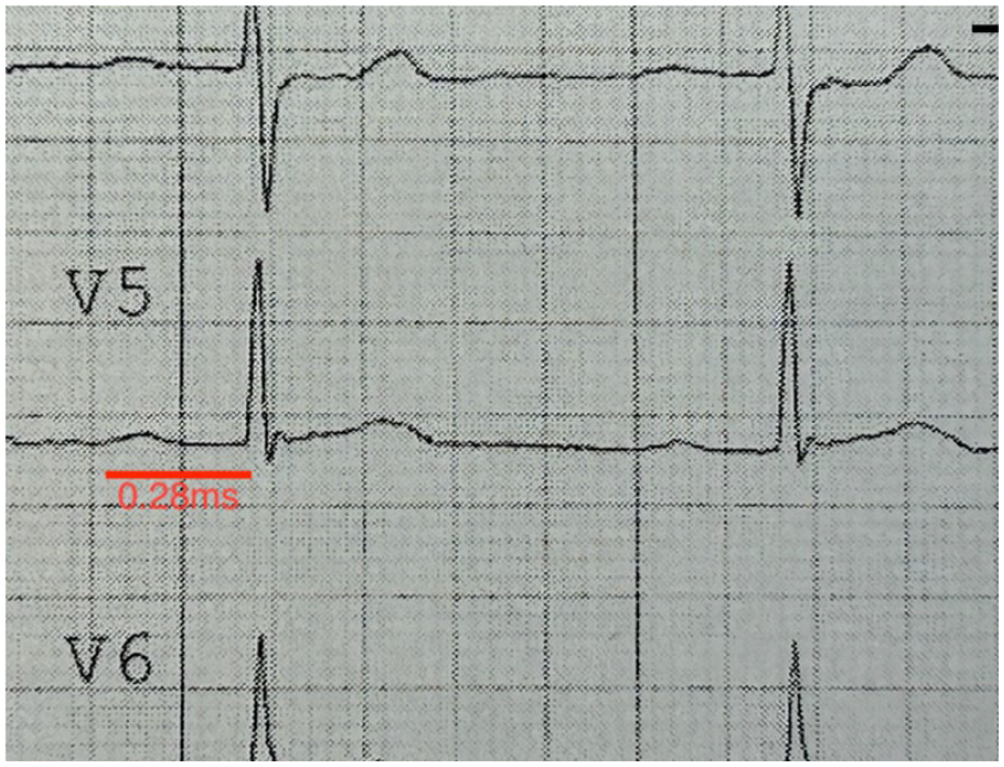
Patient’s pre-operative ECG, showing an elongated P-R interval of 0.28 ms, indicating first-degree atrio-ventricular block.
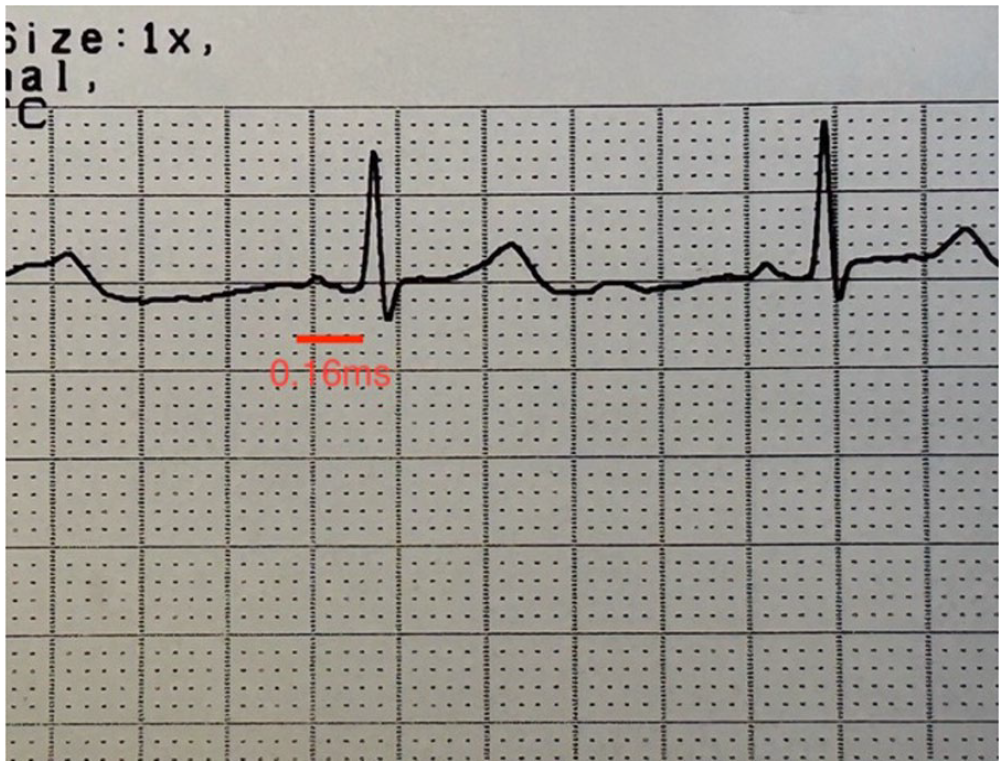
Patient’s intra-operative ECG rhythm strip. Change in cardiac rhythm was noted 10 minutes after parathyroid adenoma was removed. P-R interval had now normalized at 0.16 ms, indicating normal sinus rhythm with resolution of pre-operative atrio-ventricular block.
Discussion
Primary hyperparathyroidism is a common condition that has deleterious effects on multiple organ systems if left untreated. The majority of patients remain asymptomatic. The only cure for this condition remains surgical removal of the offending parathyroid adenoma(s), with the cure rate after initial surgery being greater than 95% in the hands of an experienced parathyroid surgeon. 2
Multiple studies have addressed the adverse effects of untreated primary hyperparathyroidism on the cardiovascular system. Some studies suggest that the disease left untreated leads to decreased life expectancy because of the development of cardiovascular problems such as hypertension, cardiac conduction abnormalities, coronary artery disease, and cardiac hypertrophy. 3 Importantly, there can be a potential reversal of the diseased cardiac state after successful parathyroidectomy, underscoring the importance of early detection of the disease and appropriate surgical removal of the parathyroid adenoma(s).4,5
Hypercalcemia is associated with increased contractility and irritability of the myocardium. Studies using rat cell myocardium have demonstrated a direct correlation between PTH and increased inotropy and chronotropy.6,7 The arrhythmogenic effect of high serum calcium has been attributed to early depolarizations, shortening of the effective refractory period, and possible reentry phenomenon.8,9 One proposition is that elevated PTH and increased intracellular calcium results in impaired mitochondrial function and oxidative stress, and ultimately cardiomyocyte necrosis, leading to the aforementioned cardiac electrochemical abnormalities. 10 Clinically, electrocardiographic changes include a prolonged P-R interval, a widened QRS complex, a shortened Q-T interval, and absent S-T segments. 11 As calcium concentrations increase, patients may develop bradyarrhythmias, bundle branch block, and atrio-ventricular block. Complete atrio-ventricular block has been seen with calcium concentrations up to 18 mg/dl and may proceed to asystole. 12
On a cardiac structural level, 2-dimensional echocardiography of those with symptomatic hyperparathyroidism demonstrate evidence of cardiac remodeling, such as greater left ventricular mass, interventricular septal thickness, and posterior wall thickness. Additionally, this was associated with diastolic dysfunction measured by tissue doppler. 13 After parathyroidectomy, there was improvement in the left ventricular mass, systolic and diastolic function, and vasodilation in this cohort. 13
The patient described above was asymptomatic and had mild hyperparathyroidism by biochemical criteria. However, pre-operatively she was found to have first-degree atrio-ventricular block. This condition promptly reverted after removal of her parathyroid adenoma. Since the half-life of PTH is approximately 5 minutes, the normalization of PTH and calcium may have corrected the increased myocardial contractility and irritability that likely caused her first-degree atrio-ventricular block. The immediate reversal of this patient’s arrhythmia after successful parathyroidectomy and normalization of PTH emphasizes the importance of treating asymptomatic hyperparathyroidism to optimize cardiac function.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: We have no conflicts of interest with other organizations or persons. Data is solely in the possession of Jesse W. Tan, MD.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this case report are available upon request. Requests for access to the data should be directed to Dr. Jesse Tan at
Ethical Statement and Consent Statement
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. Informed consent was obtained from all participants, and their privacy and confidentiality were strictly maintained. No conflicts of interest were identified for any of the authors.