
Abstract
Keywords
Introduction
Neoplasms arising from lateral skull base are mostly benign tumors such as paragangliomas, schwannomas, meningiomas, and so on, but their closeness to cranial nerves and vasculatures in lateral skull base usually leads to relevant morbidity. Due to the complex anatomy in lateral skull base area, gross total resection of these tumors was once a challenge as surgery itself could impact neural function. With better understanding of tumor nature and the appearance of high-resolution imaging technology, the treatment of benign lateral skull base neoplasia has developed over the last 50 years. More and more complicated surgeries were completed with reduced mortality. 1 Alongside survival, function and quality of life (QoL) are two significant aspects to assess the success of lateral skull base surgeries. 2 As health related-quality of life (HRQoL) has drawn more attention over the last decade, the goal of lateral skull base surgery, “complete tumor resection” was later combined with neurological function preservation. Surgical approaches were also tailored to pathology.
Objective examinations during postoperative follow-ups such as hearing data and tumor control could help surgeons to evaluate treatment approaches, but patient-reported mental, physical, and symptom-related QoL can better reveal the impact of surgery from their perspectives. Some studies in the literature have focused on QoL after skull base tumor resection,3,4 but few of them compared postoperative QoL with preoperative results. No studies have summarized the QoL after lateral skull base surgeries through infratemporal fossa approaches (IFAs), which are common approaches for lateral skull base surgery. IFAs enable the total resection of lateral skull base neoplasms. However, the involvement of nearby vital structures could cause potential postoperative complications and affect QoL. The present study aimed to assess patient-reported outcomes before and after curative surgery of benign skull base neoplasms through IFA. Two well-validated overall QoL instruments and a disease-specific QoL questionnaire were applied for comprehensive assessment of QoL.
Patients and Methods
Patient Population
A total of 47 patients were consecutively enrolled in this study from July 2015 to January 2020 at our hospital, and patients had to meet the following criteria: pathologically confirmed, previously untreated benign lateral skull base tumors undergoing radical resection through IFAs. The exclusion criteria were as follows: (i) loss during follow-up; (ii) presence of malignant tumors. Clinical information such as age, gender, treatment, and tumor pathology were obtained from the medical history of the participants. The adult comorbidity score was evaluated with the Adult Comorbidity Evaluation 27 index (a disease-specific comorbidity index), which is a validated tool for prognosis in patients with head and neck disease. 5 The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013) and approved by the Ethics Committee of Peking Union Medical College Hospital.
Surgical Procedures and Postoperative Patient Care
All patients in the study received curative surgery. Primary tumor resection was performed through IFA depending on the location and extent of the tumor. All surgeries were completed by the same surgical team to assure comparability. After surgery, these patients were placed with nasogastric tubes as temporary feeding tubes to avoid aspiration. During postoperative period, they were advised to swallow thick and pasty food at first, and then gradually tried and transferred to liquids. Patients who underwent temporomandibular joint (TMJ) dissection during surgery were instructed to avoid hard diet. During hospitalization, these patients were all able to take in enough calories and remove nasogastric tubes. After hospital discharge, patients were encouraged to visit rehabilitation doctors and psychologist if they needed certain assistance.
Patient Follow-up
After surgery, patients were evaluated every 3 months over the first 3 years and every 6 months thereafter by physical examination and CT/MRI scans. Patients were regarded as recurrence-free if tumor absence was recorded on the last visit. Recurrences were diagnosed by biopsy or CT/MRI.
Clinical Questionnaire
As the present study aimed to evaluate patients’ general QoL and symptoms related to head and neck tumor, 2 general HRQoL questionnaires, the Short Form 36 (SF-36) and World Health Organization Quality of Life–BREF (WHOQOL-BREF), as well as a disease-specific questionnaire, the University of Washington Head and Neck Quality of Life (UW-QOL), were applied. Patients in the study received postoperative QoL questionnaires at least half a year after surgery to guarantee full recovery. Patients finished all the questionnaires through online surveys.
The SF-36 is a validated instrument for measuring general health. It is easy to use, acceptable to patients, and proven to fulfill stringent criteria of reliability and validity. 6 The SF-36 questionnaire is composed of 36 items that assesses general QoL status during the past 4 weeks from 8 scales 6 : (1) physical functioning, (2) role limitations secondary to physical problems, (3) bodily pain, (4) general health and change in health, (5) vitality, (6) social functioning, (7) role limitations secondary to emotional problems, and (8) mental health. Scores of each scale were calculated and adapted to 0–100 scale according to corresponding responses. Higher scores indicate better QoL.
WHOQOL-BREF is the abbreviated version questionnaire of World Health Organization 100 item. It is a well-validated, self-administered questionnaire standardized in healthy and hospital-based population. WHOQOL-BREF domain scores demonstrated good discriminant validity, content validity, internal consistency, and test-retest reliability. 7 It is composed of 26 items evaluating 4 domains: (1) physical health, (2) psychological health, (3) social relationships, and (4) environment. Two more items involve general health and overall QoL. Data from each domain were acquired and transformed to score out of 100, with higher scores indicating better QoL.
UW-QOL is a well-validated tool widely used in head and neck cancer patients. 8 It has been tested for validity and reliability. It is also favored by patients as it is concise and easy to complete. The first part assesses functions during the past 7 days: pain, appearance, activity, recreation, swallowing, chewing, speech, shoulder, taste, saliva, mood, and anxiety. The score ranges from 0 to 100. The second part requires participants to pick the 3 most important domains during the last 7 days from the above ones. The third part comprises 3 items to evaluate HRQoL and general QoL which are measured from 0 to 100.
Statistical Analysis
Continuous variables were presented with means, medians, and interquartile ranges (IQRs); categorical variables were summarized with number of cases and percentages. Statistical analyses were performed with SPSS version 23.0 (IBM Corporation, Armonk, NY, USA). The Wilcoxon rank-sum test was applied to compare pre- and postoperative SF-36, WHOQOL-BREF, and UW-QOL scores. Variables affecting QoL were evaluated by linear regression. All statistical tests were 2-sided, and P threshold <.05 was considered statistically significant.
Results
Baseline Characteristics
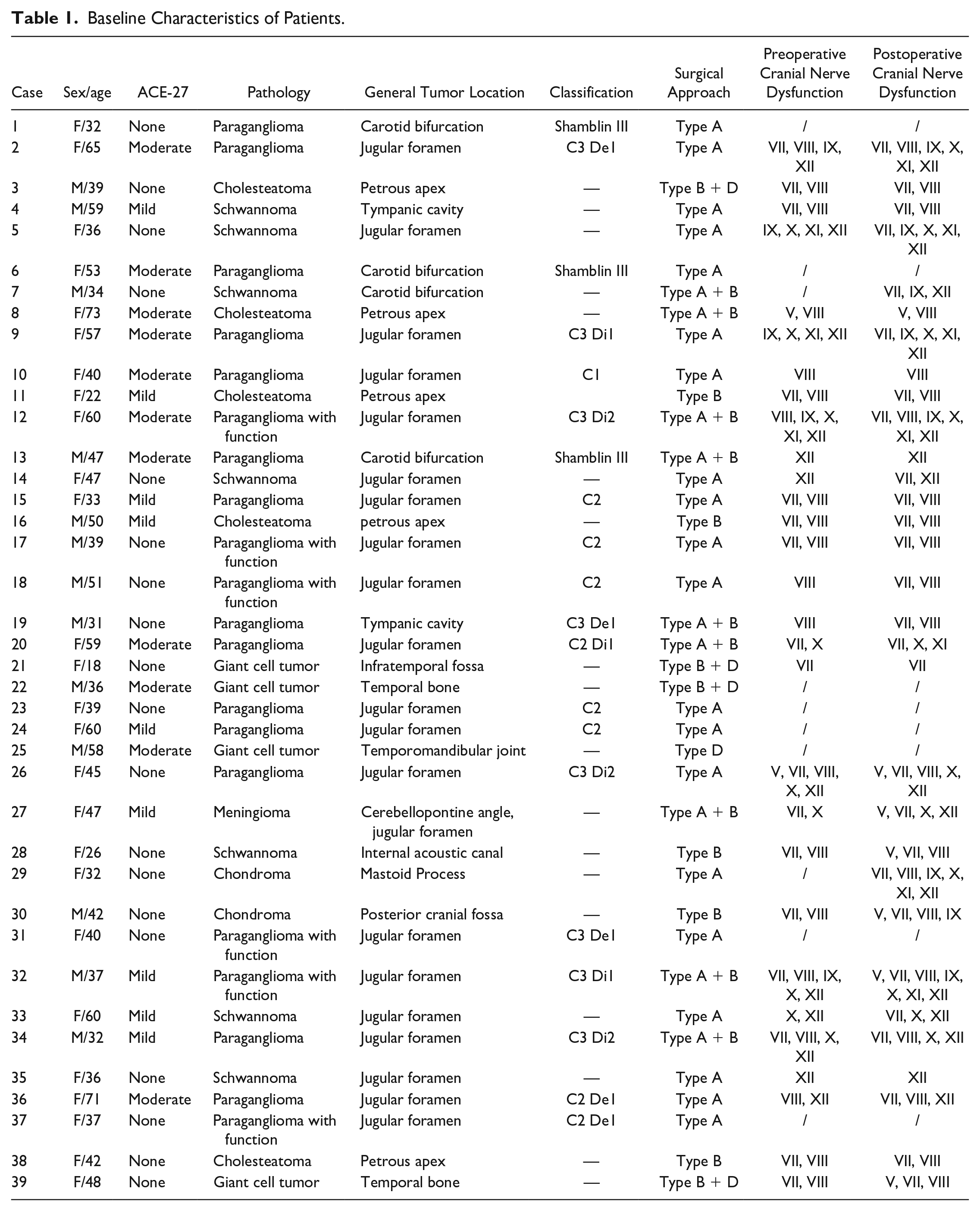
From July 2015 to January 2020, 47 patients were enrolled in this study. On the last visit, none of the participants experienced tumor residue or recurrence. Thirty-nine patients out of 47 patients (77%) in total completed all the questionnaires. Baseline characteristics of patients were shown in Table 1. Mean age was 44.4 ± 13.1 years. Most patients were between 30 and 50 years old (61.5%). The female to male ratio was 2:1 (26 females:13 males). Benign neoplasms of these patients were mostly paraganglioma (51.3%), and some of them had hormonal functions. Schwannoma, cholesteatoma, giant cell tumor, chondroma, and meningioma were also found. The most frequent IFA is type A (51.3%). Most patients (71.8%) had none to mild comorbidity score according to ACE-27. As is shown in Figure 1, patients in this study tended to have extended lateral skull base neoplasms that involved several areas such as internal carotid artery, jugular foramen, internal acoustic cavity, cochlear, etc. Most (74.4%) of the patients had cranial nerve dysfunction before surgery due to tumors.
Baseline Characteristics of Patients.
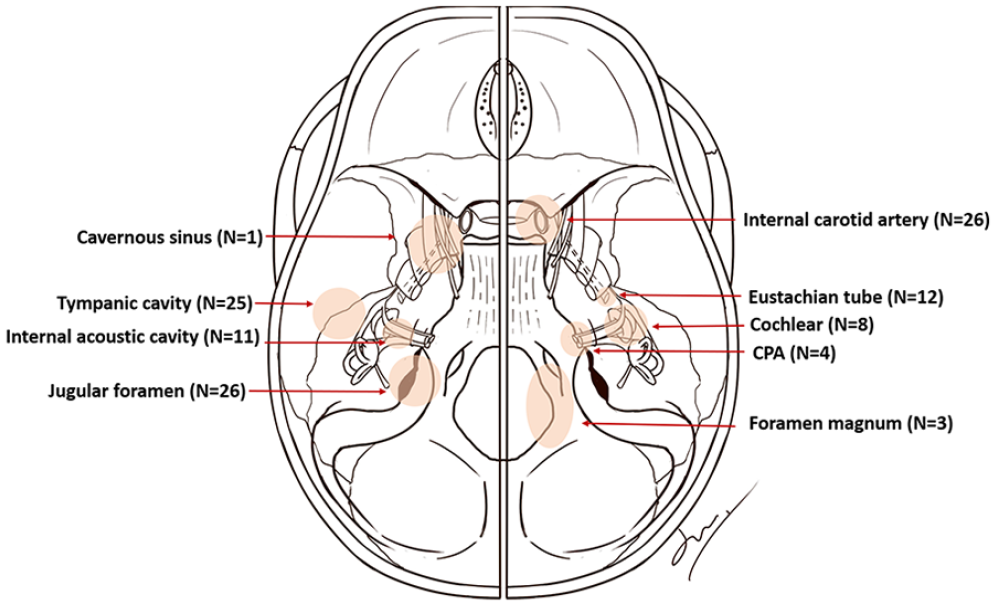
Areas of head and neck that were invaded by lateral skull base neoplasms in this study. CPA, cerebellopontine angle.
QoL Outcomes
Patients in this study reported changes in QoL when compared with preoperative results (Table 2). The QoL scores were significantly impaired in 3 out of the 25 subscales, and significantly improved in 2 subscales.
QoL Outcomes.
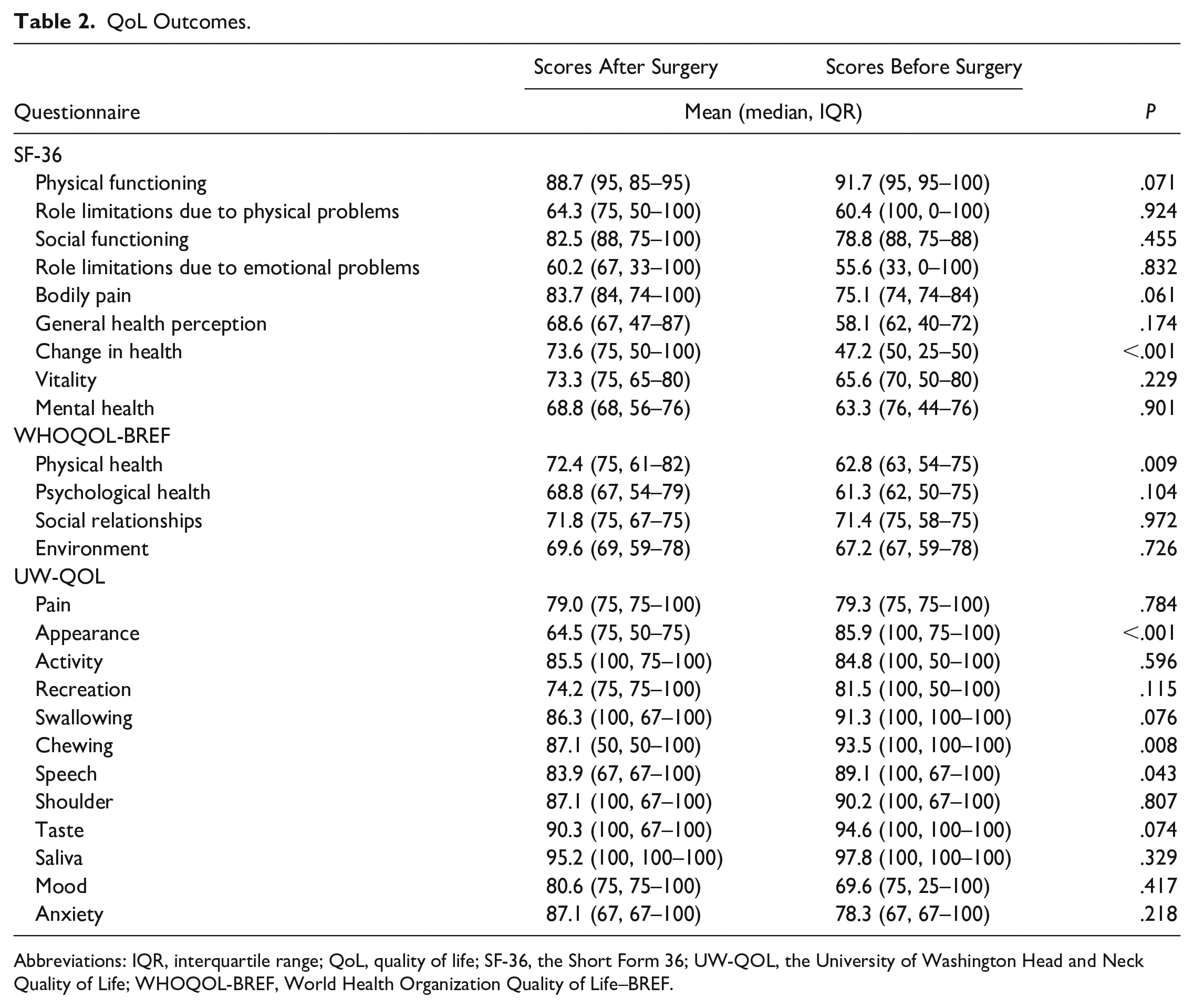
Abbreviations: IQR, interquartile range; QoL, quality of life; SF-36, the Short Form 36; UW-QOL, the University of Washington Head and Neck Quality of Life; WHOQOL-BREF, World Health Organization Quality of Life–BREF.
When studying in detail, patients in this study experienced problems in appearance, chewing, and speech after surgery according to UW-QOL questionnaire. Mood and anxiety tended to enhance after surgery according to their mean, but there are no significant differences. Subscales of SF-36 assessing change in health was significantly improved after surgery. “Change in health” asks patients to rate their health in general compared to 1 year ago. The significantly higher score after surgery implied that these patients tended to feel an improvement of general health compared to a year ago. WHOQOL-BREF showed a significant increase in physical health after surgery. Physical health domain of WHOQOL-BREF involves several aspects of life, including physical pain, medical treatment, energy, exercise, sleep, work, and daily living activities. Increased score in physical health indicated that patients benefited in the above areas of life after surgery. There are no significant differences in other domains of SF-36 and WHOQOL-BREF in Table 2, including role limitations secondary to physical problems, bodily pain, general health, vitality, social functioning, role limitations secondary to emotional problems, mental health, psychological health, etc.
In UW-QOL, patients were required to identify the 3 most important issues in the last 7 days from the 12 domains. All the 12 domains were selected by some patients as important issues that affect their lives. However, mood (n = 15, 41.7%), speech (n = 13, 36.1%), and appearance (n = 12, 33.3%) were most selected. Besides, swallowing (n = 11, 30.6%) and chewing (n = 11, 30.6%) were also selected as important issues.
Factors Influencing QoL
Age
Age was negatively associated with physical functioning and social functioning of SF-36 questionnaire (β = −.289, P = .012 and β = −.409, P = .013 respectively). Older patients tended to have lower scores assessing activity and swallowing of UW-QOL questionnaire (β = −.436, P = .008 and β = −.343, P = .04 respectively), as well as physical health of WHOQOL-BREF questionnaire (β = −.349, P = .037).
Gender
Women had significantly higher scores than men in appearance and mood of the UW-QOL questionnaire (β = .388, P = .019 and β = .45, P = .006 respectively). According to WHOQOL-BREF, women were more satisfied with their environments than men (β = .461, P = .005).
Comorbidity score
Patients with more comorbidity had lower scores assessing physical functioning and bodily pain of SF-36 questionnaire (β = −.482, P = .003 and β = −.346, P = .039 respectively). They also experienced more difficulty in swallowing and chewing (β = −.394, P = .012 and β = −.386, P = .002 respectively). Physical health score of WHO-QOL BREF among patients with more comorbidity tended to be lower (β = −.372, P = .026).
Multivariate Linear Regression Analysis
Since mood, speech, appearance as well as swallowing and chewing were selected by patients as important aspects in their lives, multivariate linear regression analysis of SF-36 and WHOQOL-BREF was carried out in a model including the following variates: age, gender, comorbidity score, mood, speech, appearance, swallowing, and chewing (Table 3). Age was an independent negative predictive factor of social functioning (β = −.499, P = .016). Female patients scored lower in physical functioning (β = −.374, P = .03) and validity (β = −.464, P = .032). Mood was positively associated with general health (β = .498, P = .011), mental health (β = .46, P = .034), and psychological health (β = .481, P = .013). Speech was positively associated with psychological health (β = .406, P = .007). Appearance could positively predict physical functioning (β = .537, P = .003). Swallowing positively affected physical functioning (β = .321, P = .049) and social functioning (β = .409, P = .031). Chewing was also positively associated with general health (β = .458, P = .016), role limitations due to emotional problems (β = .441, P = .035), and less bodily pain (β = .61, P = .001).
Multivariate Linear Regression Analysis.
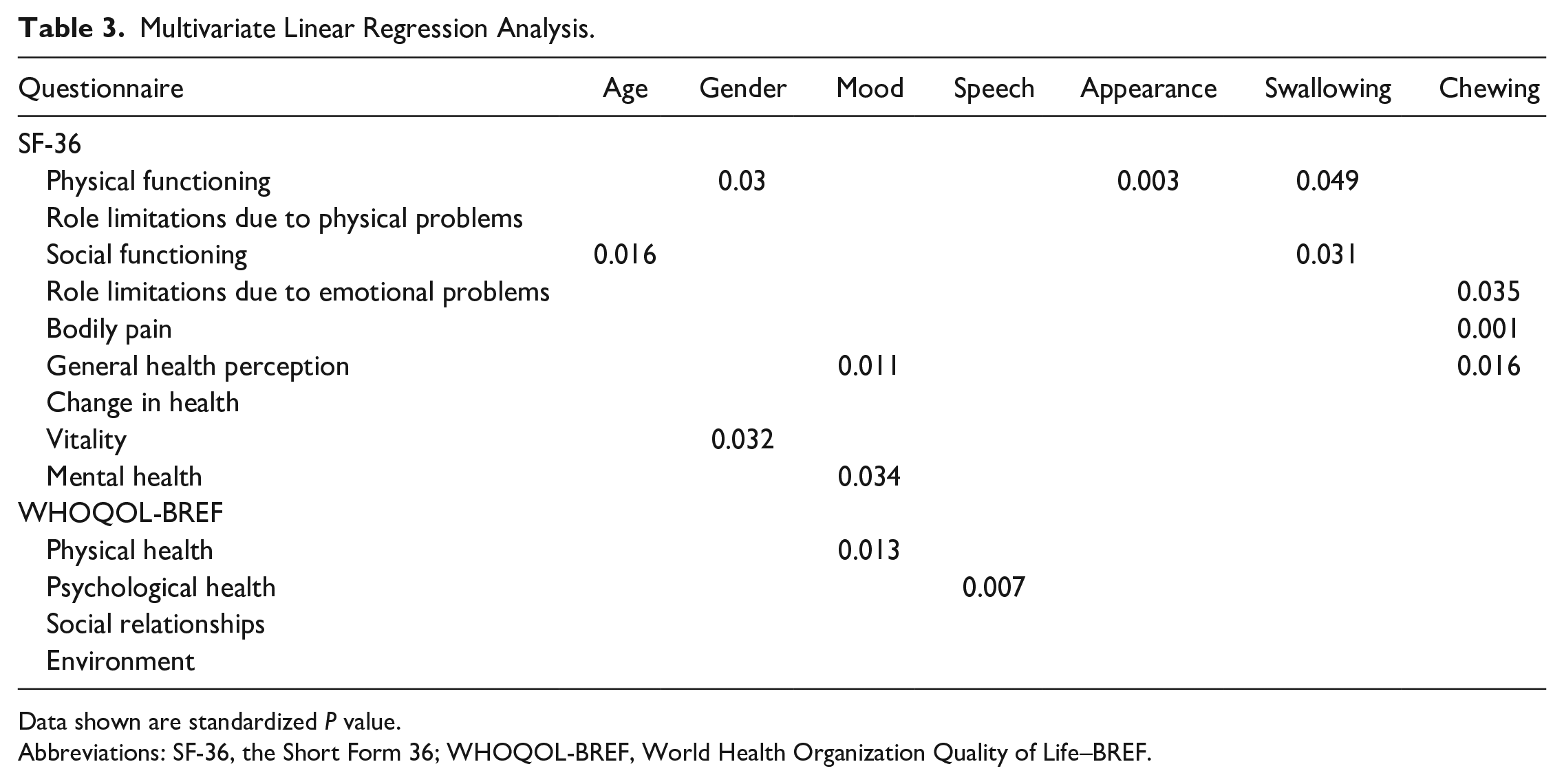
Data shown are standardized P value.
Abbreviations: SF-36, the Short Form 36; WHOQOL-BREF, World Health Organization Quality of Life–BREF.
Discussion
Although most lateral skull base tumors are benign and slow-growing, they could bring severe morbidities and even be fatal by aggressive and extended involvement of the skull base. 9 For instance, paraganglioma, the most frequent tumor in this study, is reported to have a median doubling rate of 4 years. 9 But tumor extension may lead to VII–XII cranial nerve malfunction. The natural history of lateral skull base tumor supports wait-and-see policy for small non-symptomatic tumors in older patients, but does not favor the management of young patients. A treatment is normally required for young patients. The ideal primary treatment of these tumors is surgery with the aim of total resection. With improvement of imaging technology and surgical approaches, patients’ QoL after skull base surgery have enhanced. 1 Diseases that were considered untreatable are now treated with multimodality therapy.
IFA became a common approach for lateral skull base surgery since its introduction by Fisch in 1979. 10 IFA was then categorized into type A–D. As a safe approach for lateral skull base surgeries, IFA supports surgical treatments of lateral skull base tumors, despite possible impact of appearance, voice, and chewing. Several studies have investigated the QoL of patients after lateral skull base surgery;3,4,11 however, to our knowledge, no studies focused specifically on QoL among patients after IFA. Therefore, the present study was conducted to explore QoL after lateral skull base surgeries through IFA. Additionally, most studies compared QoL of postoperative patients with healthy controls or patients with wait-and-see policy and concluded that QoL in patients were impaired after surgery. It should be noted that QoL is a complex evaluation and unique to an individual. In the present study, QoL of patients before surgery were recorded and used as controls so that impacts of confounding factors such as age, gender, and comorbidity score, were minimized.
Patient-reported QoL was chosen to assess IFA in this study instead of objective examinations, because it is not rare that patients are dissatisfied with outcomes which are outstanding for clinicians. 12 Objective examinations and other assessing tools established by health care providers usually focus on a few aspects of technical outcomes and could hardly treat patients as a whole body to evaluate effects of disease or treatment; therefore, patient-reported QoL has gained increasing attention in the past decades. Studies indeed uncovered that even benign head and neck tumors have significant impact on physical and psychological HRQoL, 13 reinforcing the importance of HRQoL results besides traditional examinations.
To give a full understanding of QoL after IFA, two widely used general assessment tools, SF-36 and WHO-QOL BREF were applied. As there is no questionnaire for lateral skull base disease, UW-QOL, a questionnaire evaluating pain, appearance, swallowing, chewing, speech, and other important domains of head and neck disease was also adopted to minimize the bias from a single method.
It is not surprising that patients in this study experienced some impacts on appearance after IFA. First, IFA involves extended skin incision from temporal region to neck which affects the appearance of patients to some extent. Second, facial nerve anterior transposition is routinely performed during IFA-A in order to get better exposure, which would impact facial nerve function after surgery. Although studies reported a good chance that facial nerve function would restore to H-B I–II level, 14 which was also observed in this study, it is predicable that there would be alteration in patients’ appearance. Third, temporalis muscle and abdominal fat are used to full the surgical cavity, which could not give a completely symmetrical appearance of the skull.
Score of chewing was also found to be impaired after surgery in this study. TMJ dissection in IFA-B could be the cause. TMJ dissection is commonly performed in IFA either for tumor exposure or due to tumor invasion. 15 Studies reported that TMJ dissection could impact mandibular movement and reduce the maximum opening of mouth, 16 thus increasing the difficulty of chewing certain foods after surgery.
Speech could be impacted if vagus nerve is cut during surgery. TMJ dissection mentioned above could also affect symmetry and vocal resonance of mouth, 16 which may contribute to lower score of speech after surgery.
Although some aspects of UW-QOL were impaired in patients, subdomains of SF-36 and WHOQOL-BREF were not significantly affected. Change in health was significantly improved in these patients, probably due to the thought that surgery had cured their diseases. When studying vestibular schwannomas, researchers reported a statistically significant better SF-36 mental score favoring patients undergoing gross total resection compared with less than total resection. 4 It was inferred that when patients knew they had tumor that could grow and cause other symptoms, this converted to significantly lower mental health scores of a general QoL questionnaire. The increasing tendency of mood and anxiety scores in our results added to this point of view. Besides, patients after IFA scored higher in several domains such as bodily pain, general health, vitality, and psychological health, although not statistically significant. These improvements may translate into a significantly higher score of physical health in postoperative patients.
Mood, appearance, and speech were chosen as most important aspects from postoperative patients, followed by swallowing and chewing. Our results mostly agree with other studies of head and neck disease,17,18 one exception being that appearance is not commonly voted as important in other studies, whereas in ours it was not the case, which could be explained by the relatively younger age of our patients (mean age 44.6).
Assessment of particular factors influencing QoL in these patients demonstrated expected associations of age and gender, as was shown by other studies, 3 except that women scored higher in appearance, mood, and environment in univariate analysis. Mood, speech, and appearance were independent predicative factors of QoL, which are in line with other studies of head and neck diseases.19,20 Swallowing and chewing were also found to have a positive association with QoL, adding to evidence of previous studies. 19
Since most patients undergoing IFA are middle-aged and are likely to live more than 20 years after surgery, it is significant to get a comprehensive understanding of their QoL after surgery. Our results showed that patients seemed to benefit regarding overall QoL after gross tumor resection from IFA, despite the impact of appearance, speech, and chewing.
The mean score of appearance before surgery was 85.9, as 11 out of 39 patients (28.2%) already suffered from facial paralysis before surgery. It dropped to 64.5 after surgery, between “minor change in appearance (75)” and “my appearance bothers me but I remain active (50).” These results indicated that the instant change of appearance and possible impact on chewing and speech are the price to pay for IFA to prevent further morbidities of lateral skull base tumors. As continued growth of tumors can also impact appearance, chewing, and speech of patients, let alone the psychological burden caused by tumors, it is important for patients to seek medical treatment despite potential postoperative morbidities.
As is shown in this study, patients experienced impacts in appearance, chewing, and speech after IFA. These 3 aspects were independently associated with general QoL. Thus, surgeons should balance the benefit and cost of lateral skull base surgeries for each patient and schedule a personalized treatment. Function preservation and restoration are significant during lateral skull base surgery under the premise of total resection of tumors. 15 New surgical approaches for restoration and non-surgical treatments for lateral skull base diseases are urgently needed. In this study, patients were encouraged to visit rehabilitation doctors for speech and language therapy or psychologist if they needed certain assistance; however, 38 out of 39 of the patients didn’t receive rehabilitation therapy either due to satisfaction with their current situations or financial reasons. In summary, postoperative QOL outcomes in present study basically displayed the results of recovery from surgeries without further rehabilitation or psychological assistance after hospital discharge. Certain rehabilitation and psychological services should also be enhanced in the future to improve postoperative QOL.
To our knowledge, our study was the first to comprehensively evaluate the change of QoL through IFA. However, there are several unavoidable limitations in this study. First, this is a study in a single institution which may lead to possible selection bias, and patients who are anxious about their diagnosis and disease-related symptoms are more likely to receive a complex surgery and thus enrolled in this study. Second, the relatively small sample size due to rarity of lateral skull base disease might bias our conclusions. Further studies with more patients are urged to confirm our conclusion.
Conclusion
In conclusion, our study demonstrated that patients diagnosed with benign lateral skull base neoplasms experienced impacts in appearance, chewing, and speech after surgery through IFA. However, there were no significant changes in other aspects of QoL such as mental health, social relationships, vitality, and so on. Besides, patients tended to feel an improvement of general health after surgery compared to a year ago. Physical health was also enhanced after surgery. Speech, appearance, swallowing, and chewing contributed independently to general QoL. Therefore, function preservation and restoration are significant during lateral skull base surgery.
Footnotes
Authors’ Contributions
GF provided the overall study design and cowrote the paper. SY designed the study, collected and analyzed data, and drafted the paper. HS was responsible for the data analysis with software and cowriting the manuscript. XT and YZ were responsible for patients’ follow-up, collecting related data, and cowriting the paper. ZG contributed to study design and cowriting the paper. GF prepared to take responsibility for the integrity of the content of the manuscript. All authors have read and approved the final version of the manuscript.
Data Availability
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from National Multi-disciplinary Diagnosis and Treatment Development Program for Major Disease Z155080000004, Beijing’s Science and Technology Planning Project Z191100007619040, National High Level Hospital Clinical Research Funding LY22B0950001017, and Precipitation of Scientific Research Funds from Peking Union Medical College Hospital ZC201901017.
Ethical Approval
The authors assert that all procedures contributing to this work comply with the ethical standards of Ethics Committee of Peking Union Medical College Hospital and with the Helsinki Declaration of 1975, as revised in 2013. The study was approved by the Ethics Committee of Peking Union Medical College Hospital, Beijing, China.