
Abstract

Significance Statement
This is a case of sialometaplasia with pseudoepitheliomatous hyperplasia presenting as a supraglottic mass. Minor salivary glands exist throughout the aerodigestive tract, and it is essential to differentiate benign metaplastic changes from malignancy, namely squamous cell and mucoepidermoid carcinomas. This requires thorough workup including history and physical exam, cross-sectional imaging, and in-depth pathologic evaluation with low-molecular weight keratin (eg, CK7), mucicarmine, myoepithelial (eg, SOX10), proliferation marker (eg, Ki-67), and tumor marker (eg, p53) stains. Because the lesion closely mimics malignancy, a definitive diagnosis is imperative to avoid unnecessary treatments.
A 51-year-old male with a past medical history significant for incarceration and prolonged tobacco use (30 pack years) presented with an incidental laryngeal mass discovered on a computed tomography (CT) scan of the cervical spine following an altercation. Upon questioning, the patient reported intermittent dysphonia, globus, and solid food dysphagia for 6 months. CT showed a 9 mm soft tissue prominence on the left vocal fold. He denied unilateral otalgia, unplanned weight loss, severe fatigue, loss of appetite, hemoptysis, and vocal trauma. Flexible laryngoscopy revealed a large cystic mass obscuring the left true vocal fold (Figure 1).
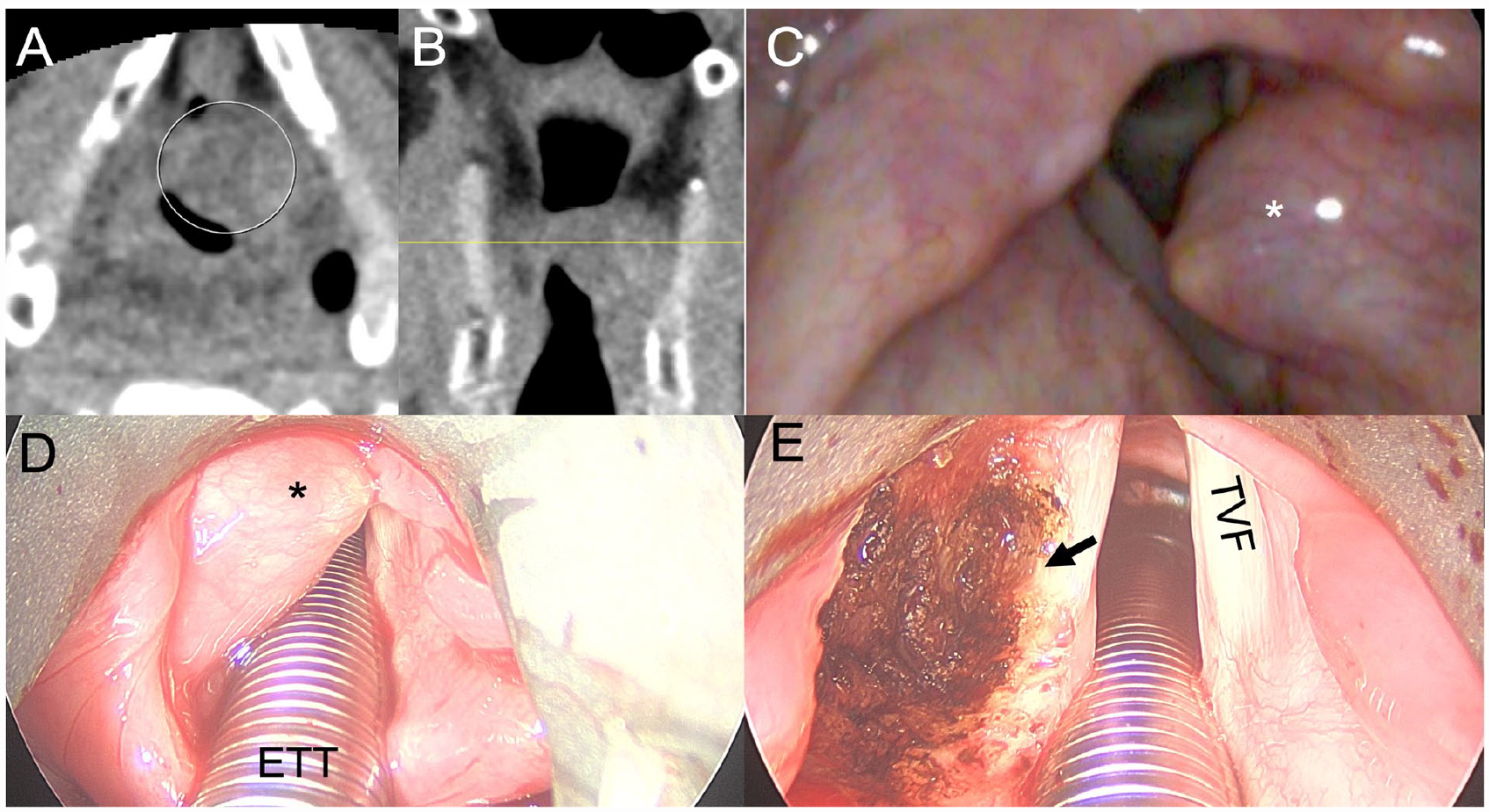
Computed tomography and endoscopic images of laryngeal mass. (A) Axial CT image of laryngeal mass (encircled). (B) Coronal image of laryngeal mass with localizer line. (C) Flexible laryngoscopy view of cystic mass (*) obscuring the left true vocal fold. (D) Operative view of left supraglottic mass (*) under direct laryngoscopy. (E) Resection bed (arrow) following carbon dioxide laser excision of supraglottic mass. ETT, endotracheal tube; TVF, true vocal fold.
The patient was taken for direct laryngoscopy with carbon dioxide laser excision of the lesion without complication. Pathology revealed a 1.5 cm squamous epithelium-lined cyst with closely associated circumscribed 7 mm focus of squamous proliferation with keratin pearls without evidence of invasion or cytologic atypia (Figure 2). Immunohistochemical staining revealed squamous nests (p40/CK7 positive) with surrounding myoepithelial layers (SOX10 positive). The lesion was Kp53 wild-type despite increased expression, with a Ki-67 proliferation rate up to 10%. Phosphatase and tensin homolog (PTEN) expression was retained. Mucicarmine stain highlighted scattered mucocytes (Figure 3). This constellation of features supported the diagnosis of sialometaplasia with pseudoepitheliomatous hyperplasia.
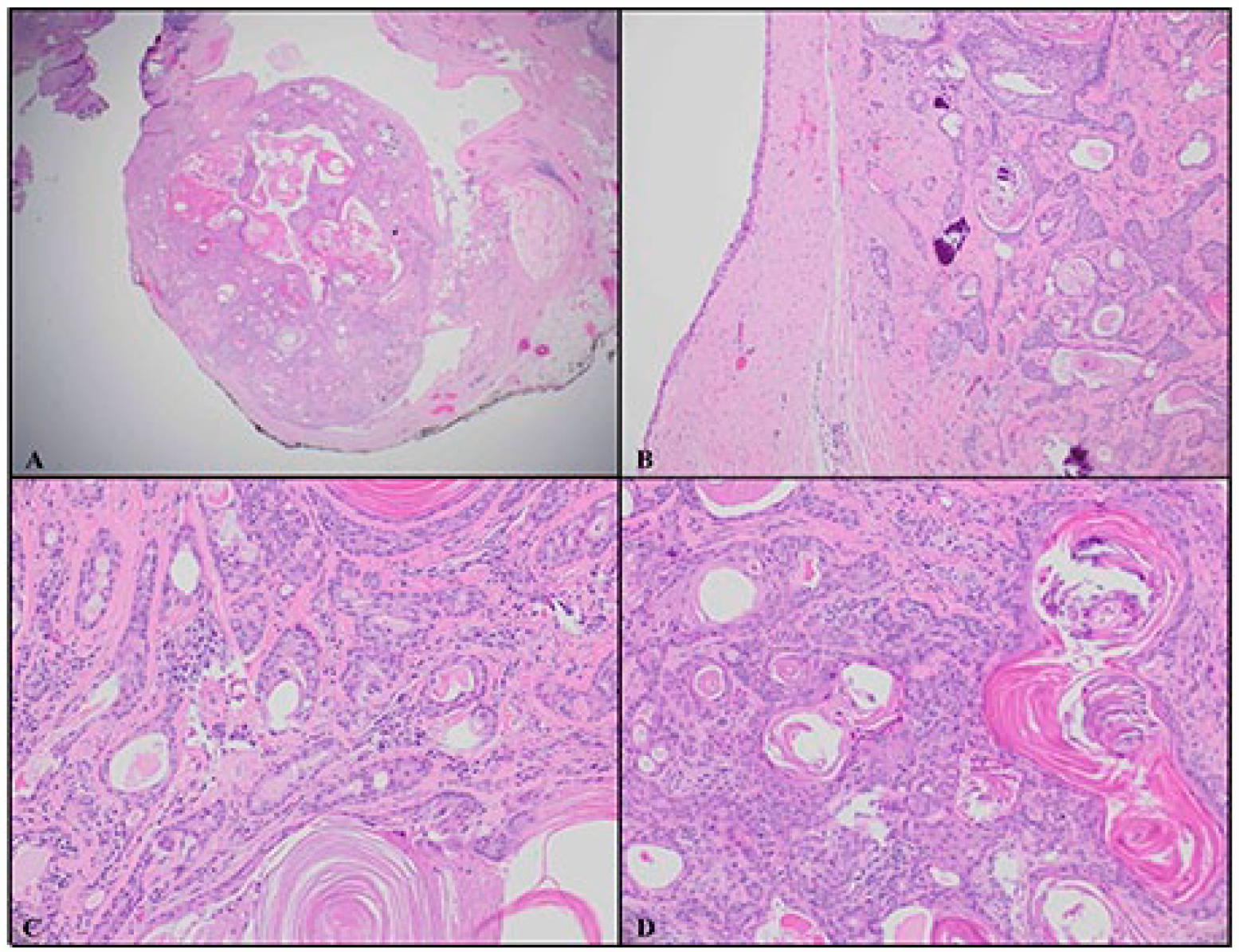
Histology of laryngeal mass with hematoxylin and eosin (HE) staining. (A) Well circumscribed squamous proliferation associated with the cyst (HE 2X). (B) Bland squamous proliferation associated with the squamous epithelium-lined cyst (HE 10X). (C) Some of the nests show luminal squamous metaplasia and abluminal myoepithelial layer (HE 20X). (D) Florid squamous hyperplasia in areas (HE 20X).
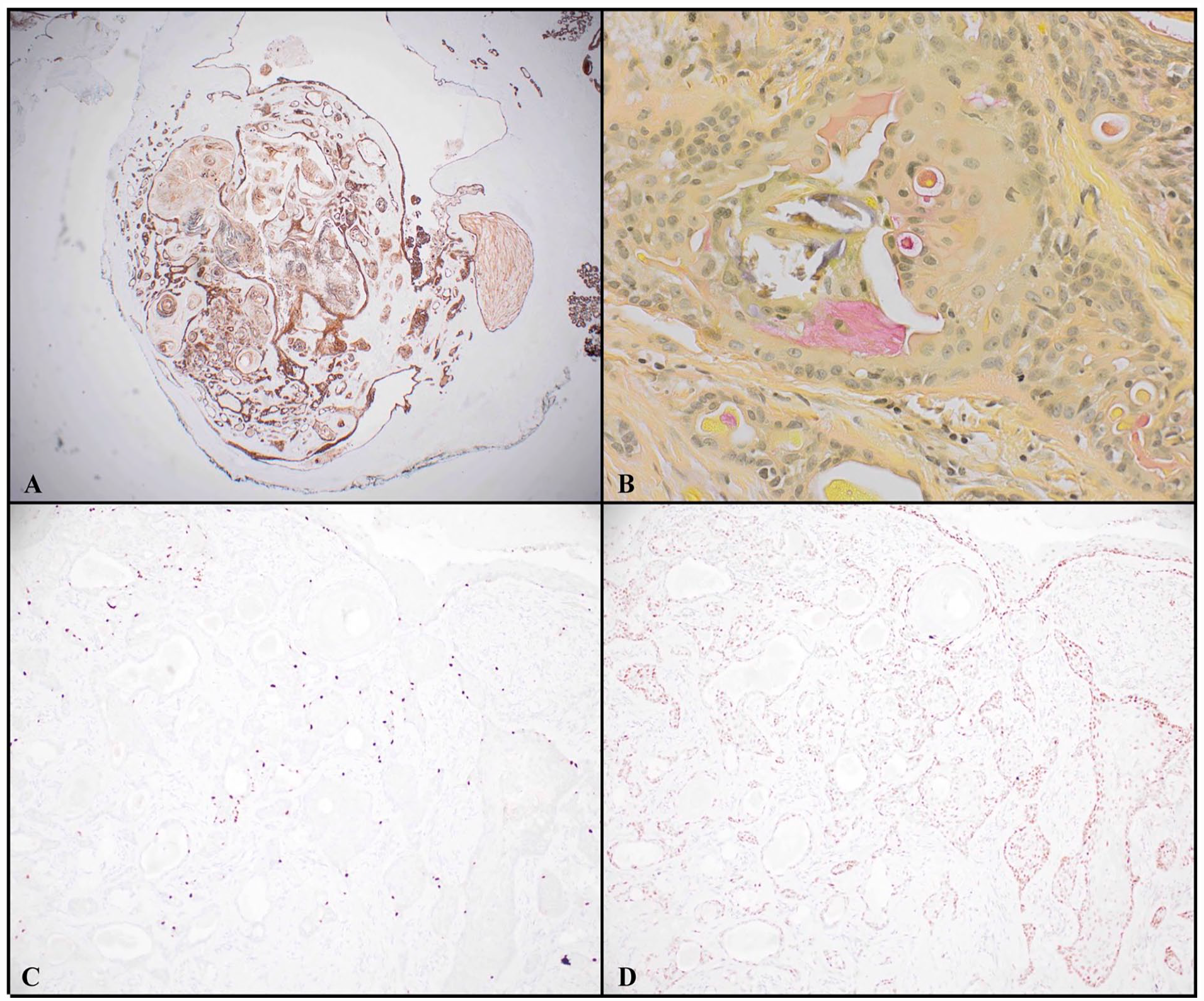
Immunohistochemical staining of laryngeal mass. (A) Squamous proliferative lesion positive for CK7 (2X). (B) Mucicarmine stain highlights scattered mucocytes (40X). (C) SOX10 labels myoepithelial cells at the periphery (10X). (D) Wild-type, slightly increased p53 expression (10X).
The upper aerodigestive tract contains several hundred minor salivary glands. 1 In contrast to major salivary glands, minor salivary glands are less likely to undergo neoplastic change, but lesions have an estimated 60% likelihood of malignancy. 2 -4 Though minor salivary gland malignancies comprise only 1% to 5% of laryngeal tumors, thorough evaluation is imperative due to their high morbidity and greater propensity for asymptomatic growth compared to glottic lesions. 1,5 -7 The most common histologic subtype in the upper aerodigestive tract is mucoepidermoid carcinoma. 7
The literature on sialometaplasia of the larynx is sparse and largely limited to the necrotizing variant, which is caused by tissue ischemia and is classically characterized by pain and ulceration. 1,8 -10 This case illustrates an uncommon, less obvious pathologic diagnosis where these metaplastic findings were discovered in light of minimal symptomology. As with this patient, history and physical exam may be unrevealing, but special attention should be paid to the endoscopic evaluation of the upper aerodigestive tract with low threshold for radiographic imaging. 11 Endoscopy may permit direct visualization of early stages of necrotizing sialometaplasia, like ulceration. Meticulous and thorough analysis by pathology and immunohistochemical staining are crucial for ruling out malignancy and establishing a benign diagnosis. A low mitotic index, no atypical mitoses, no cytologic atypia, and the circumscribed nature of the lesion are all reassuring characteristics that favor a benign process. Elevated or absent expression of the tumor suppressor gene p53 can be used as a general marker for potentially malignant versus benign disease. Mucicarmine staining can be used to highlight residual mucocytes of minor salivary glands. Squamous cell carcinoma would be negative or focally positive when staining for low-molecular weight keratin (eg, CK7). SOX10 staining labels peripheral myoepithelial cells, which would be negative in squamous cell carcinoma and mucoepidermoid carcinoma.
This case demonstrates laryngeal sialometaplasia with pseudoepitheliomatous hyperplasia in a rather asymptomatic individual with a laryngeal mass incidentally discovered radiographically. This case highlights this rare benign laryngeal finding and the importance of a thorough workup, as well as the critical importance of histopathology. While no further treatment was necessary for this individual, given the degree of proliferation, increased p53 expression, and positive margin status, the patient will be checked for surveillance at regular 3-month intervals for his first postoperative year. While necrotizing sialometaplasia is believed to be self-limited, this rarer non-necrotizing form is not well characterized; and thus continued monitoring is warranted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.