
Abstract

Significance Statement
When confronted with unilateral tonsillar enlargement in an adult, clinicians compulsively assume malignancy until proven otherwise. While lymphoproliferative malignancies are important diagnoses to consider, it should be highlighted that the differential also includes benign pathologies. Benign follicular hyperplasia with clonal B cells is a rare diagnosis characterized by clonal B cell expansion without histopathologic or molecular hallmarks of malignant lesions. Careful evaluation by hematopathology differentiates this entity from lymphoid malignancies and observation is the primary treatment.
A 67-year-old male presented to the emergency department for evaluation of sudden but resolved left-sided weakness concerning a stroke. During his emergency department workup, computed tomography (CT) imaging was obtained which demonstrated an incidental right tonsillar mass. His past medical history was notable for active smoking, chronic paranoid schizophrenia, gastroesophageal reflux, mild sleep apnea, and past opioid dependence. Stroke workup demonstrated a small right thalamic stroke, though no residual neurologic deficits were noted on examination. He was asymptomatic from the tonsillar lesion, without symptoms of airway obstruction, dysphagia, or dysphonia.
CT imaging of the neck demonstrated a 2.9 × 2.5 × 3.2 cm of soft tissue mass in the right oropharynx (Figure 1). The lesion appeared to originate from the right tonsillar fossa, crossed midline, and was abutting the soft palate. CT imaging of the chest was performed which demonstrated stable emphysema and small, subcentimeter pulmonary micronodules. These findings were concerning for a primary oropharyngeal or lymphoid malignancy. The patient was taken to the operating room for exam under anesthesia. A smooth, exophytic mass was seen arising from the right tonsil and a biopsy was obtained. After review of the preliminary pathology, secondary tonsillectomy was performed. Final histopathologic evaluation demonstrated tonsillar tissue with predominantly expanded lymphoid follicles positive for CD21 (Figure 2). Flow cytometry demonstrated a lambda light chain restricted monoclonal B cell population with increased CD19, CD20, and CD38 (Figure 3). No follicular lymphoma-associated patterns, such as BLC-2 overexpression, were detected. Fluorescence in situ hybridization studies did not demonstrate the canonical B cell lymphoma translocation t (14:18) or the BCL-6 gene rearrangement. Additionally, no follicular lymphoma-associated mutations such as BCL-2, KMT2D, TNFSF14, or EZH2 were detected by the lymphoid next-generation sequencing study panel. Final histopathologic diagnosis was benign follicular hyperplasia with clonal B cells. No further treatment was recommended after review by multidisciplinary tumor board, and the patient elected to proceed with routine observation and follow-up.
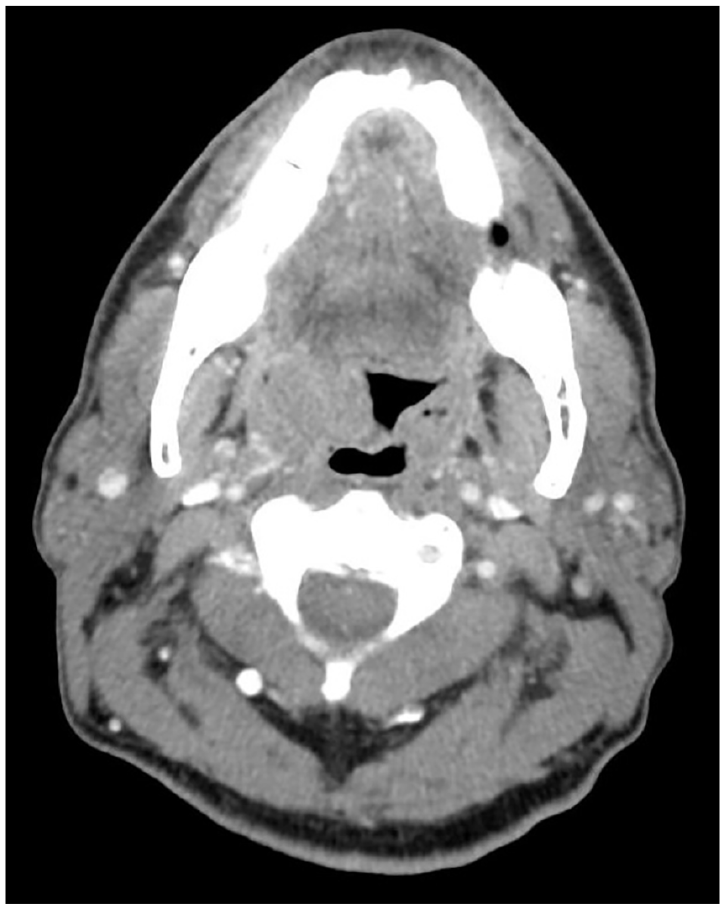
CT imaging of right tonsillar mass. Axial images demonstrating an exophytic right oropharyngeal mass that originates from the tonsillar fossa. CT, computed tomography.
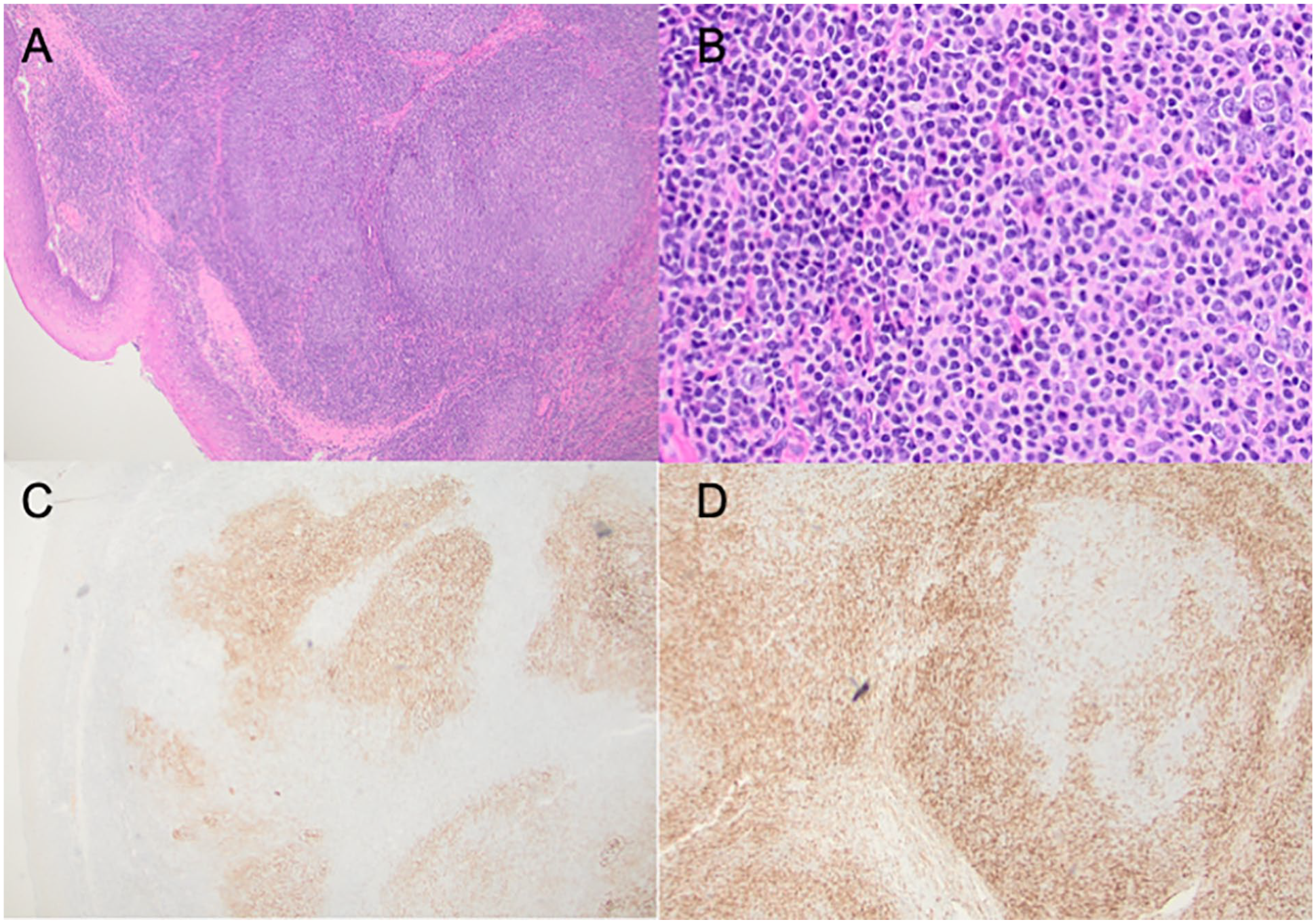
Florid follicular hyperplasia in a right tonsil mass. (A) Section shows large follicles with reactive-appearing morphologic features (H&E, ×10). (B) High-power view of a follicle with reactive-appearing features (H&E, ×20). (C) Reactive follicles contain dendritic cell meshworks as confirmed by immunohistochemical stain (CD21, ×10). (D) Follicular cells are negative for BCL-2 as confirmed by immunohistochemical stain (BCL-2, ×10). H&E, hematoxylin and eosin.
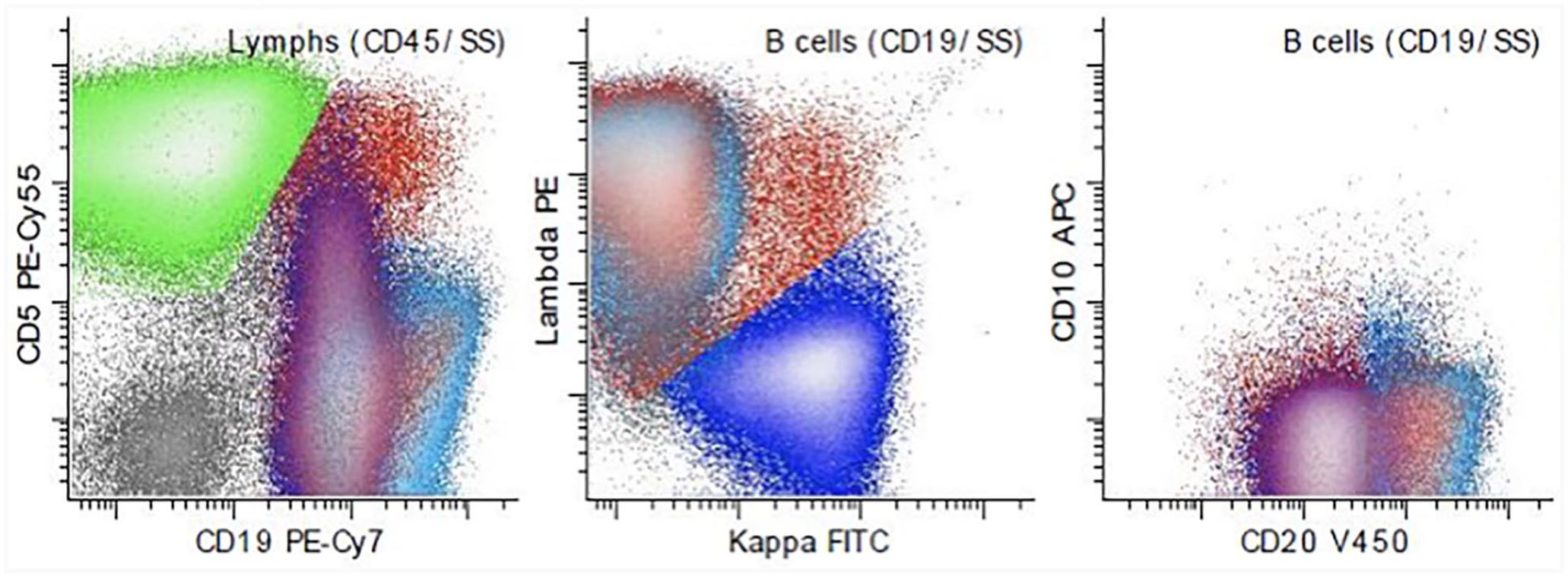
Clonal B cells identified by flow cytometry. Ten-color flow cytometric evaluation demonstrates an abnormal mature B cell population (blue-green) (representing 26.8% of the total white cells) showing abnormal expression of CD19 (increased, first dot plot from left), CD20 (increased, third dot plot from left), and lambda light chain restriction (second dot plot from left) without CD10 (third dot plot from left) or CD5 (first dot plot from left). Clonal B cell population is also confirmed by immunoglobulin H gene rearrangement polymerase chain reaction study (data not shown).
In this report, we document a rare case of follicular hyperplasia with clonal B cells that presented in the head and neck with unilateral tonsillar enlargement. The differential diagnosis for unilateral tonsillar enlargement is broad, however, suspicion should be raised for malignancy based on patient demographics and history. Lymphomas account for 5 to 15% of head and neck malignancies, while extranodal lymphomas make up <1% of all head and neck cancers. 1,2 Given the prevalence of lymphoid tissue in the head and neck, otolaryngologists need to assist patients and other healthcare providers in differentiating between benign and malignant lymphoid processes. The diagnosis of hematologic and lymphoid malignancies is complex, requiring not only tissue biopsy, but also partnership with an experienced hematopatholgist.
Historically, clonal B cell proliferation was viewed as a marker of malignancy in lymphoid proliferations, such as an enlarged palatine tonsil. 3 However, Kussick et al described multiple cases where clonal B cells populations were identified, but further histopathologic and molecular characterization failed to demonstrate evidence of neoplastic proliferation. Specifically, the absence of BCL-2 overexpression on histologic evaluation and lack of t (14;18) rearrangement in follow-up molecular studies argued against malignancy. Furthermore, in this case series (n = 6) with follow-up ranging from 13 to 56 months, none of the patients developed lymphoma. 4 Interestingly, 5 of the 6 patients in this study presented with head and neck lymphoid proliferations (1 tonsil, 3 cervical lymph nodes, and 1 intra-parotid node), with only 2 patients above the age of 18 years and the oldest case occurring in a 32-year-old patient. One additional study by Aisagbonhi et al incidentally noted 2 additional cases of pediatric tonsillar follicular hyperplasia with clonal B cells. 5
Despite the rarity of this diagnosis, differentiating follicular hyperplasia with clonal B cells from lymphoid malignancies such as follicular lymphoma remains a crucial diagnostic task for otolaryngologists when there is suspicion for a lymphoproliferative process. Follicular lymphoma is often treated with radiotherapy, immunotherapy, and chemotherapy, while follicular hyperplasia with clonal B cells is a benign condition without described cases of transformation to lymphoma, supporting observation as a reasonable treatment paradigm. 6 Given the potential for misdiagnosis and overtreatment, otolaryngologists should consider follicular hyperplasia with clonal B cells when presented with an atypical lymphoproliferative lesion and there should be a low threshold to consult an experienced hematopathologist.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was deemed exempt by the Institutional Review Board.