
Abstract
Introduction
Severe acute respiratory syndrome coronavirus 2 has spread globally to cause the coronavirus disease 2019 (COVID-19) pandemic, with over 239 million cases and approximately 4.88 million deaths, as of fall 2021. 1 The pandemic has drastically affected many aspects of everyday life and has led to significant modifications within the healthcare system. Otolaryngology, as a specialty, is no exception.
Over the course of the pandemic, literature has emerged highlighting the effects of COVID-19 on hospital systems, changes in specialty care, and residency training, among other outcomes. There are a number of articles describing the impact of COVID-19 surges on otolaryngology consultations and emergencies. Dharmarajan et al demonstrated that compared to pre-COVID-era, otolaryngology consultation rates at the University of Pittsburgh Medical Center during the first COVID-19 surge (March and April 2020) were decreased by 21.5%. 2 Based on the type of consultation, specific surge algorithms were created and followed to minimize the potential for COVID-19 exposure and maximize safe otolaryngology practices. 2 Several other groups reported a decrease in pediatric and adult otolaryngology emergency visits during the first wave of the pandemic.3,4 Shomoroney et al recently published otolaryngology consultation data for a large academic center in New York City. 5 The number of inpatient otolaryngology consultations initially decreased in March 2020, but quickly rebounded, while the reasons for consultation and interventions changed significantly. 5 Other studies reported the most common types of inpatient and outpatient otolaryngology consultations during the initial COVID-19 surge, and the methods of management with important safety considerations.6,7
Despite the flurry of useful information on practice patterns during the first surge of the pandemic, there is no literature to date examining the lasting effect on otolaryngology practice as the healthcare system navigates to a new steady state. Measuring practice patterns is critical to continue to uphold our clinical and academic mission. We aim to examine longitudinal inpatient otolaryngology consultation patterns at a large, urban, quaternary care referral center during COVID-19 surges and the lasting impact as vaccines became widely available and infection rates declined.
Patients and Methods
This study was approved by the Rush University Medical Center Institutional Review Board with waiver of informed consent (No. 21062104). A retrospective chart review was performed of all inpatient otolaryngology consultations at a single, urban, academic medical center from June 2019 to June 2021. Time frames were divided into pre-COVID-19 (Jun 2019-Feb 2020), Surge 1 (Mar 2020-May 2020), Surge 2 (Oct 2020-Jan 2021), and Post Surge (Mar 2021-Jun 2021). These time frames were delineated based on the number of COVID-19 hospitalizations and deaths reported by the City of Chicago (Figure 1). 8 Intervening transition months were intentionally excluded from the analysis to avoid confounding the surge trends. The electronic medical record (EMR) was queried for basic demographic and clinical information including age, sex, race, COVID-19 status at the time of consultation, reason for otolaryngology consultation, procedures performed, COVID testing information, length of stay, death during hospital stay, and follow-up clinic visit. If a patient had multiple consultations over the course of the same admission, only the first consultation within the specified time frame was included. Patients were only excluded if the otolaryngology consultation was filed in error or fell outside of the study time period.
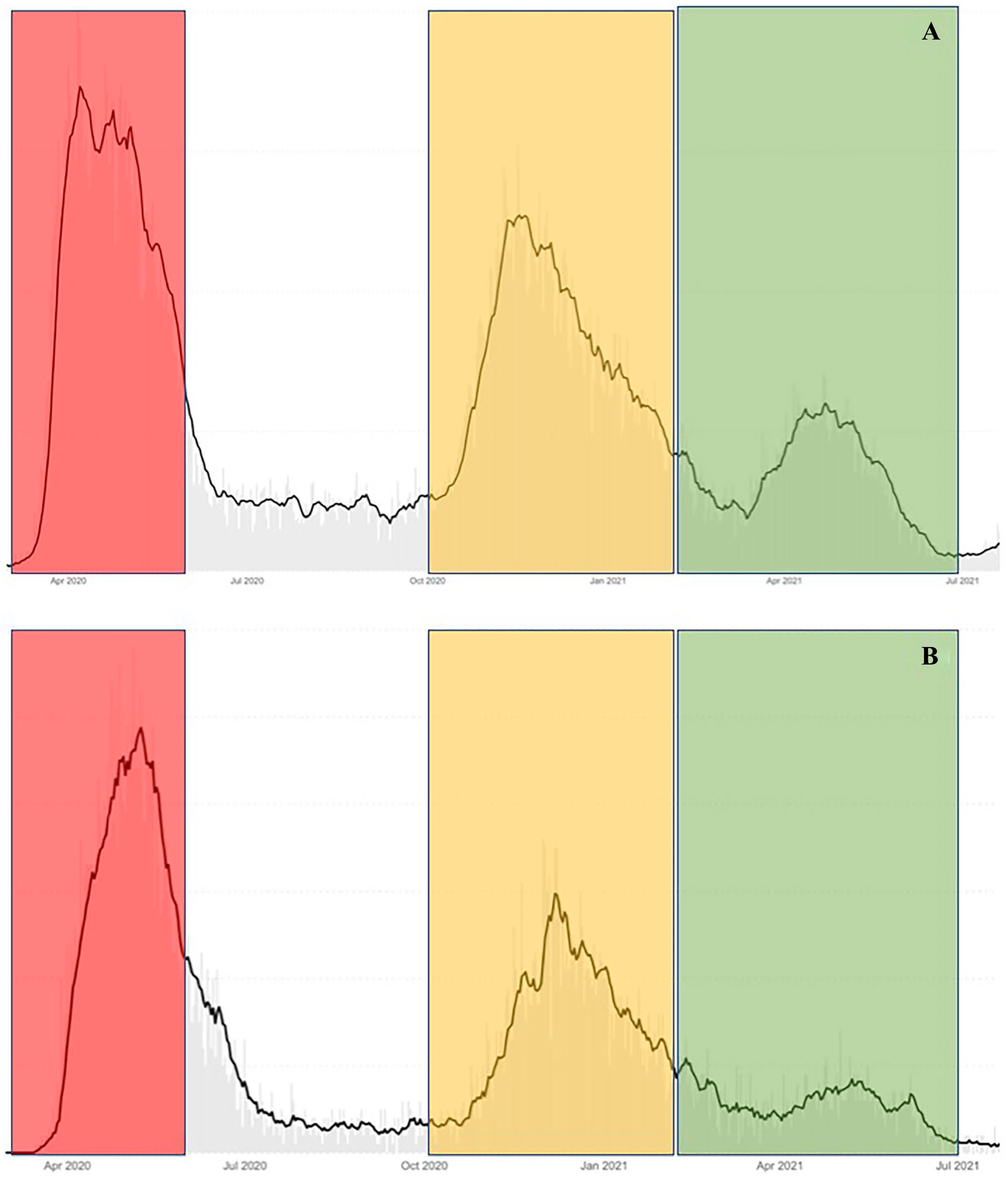
Coronavirus disease 2019 (COVID-19) hospitalizations (A) and deaths (B) in Chicago, IL from Chicago.gov. Red time frame indicates “Surge 1.” Orange indicates “Surge 2.” Green indicates “Post Surge.”
The primary outcome of the study was consultation volume (as number of consultations per day) during each time frame, and the secondary outcomes were reason for consultation and COVID testing status across time periods during the pandemic.
Continuous variables including age and number of consultations per month were analyzed via student’s t-test for statistical significance. Categorical variables were analyzed via chi-square analysis. These include the percentage of pediatric patients, sex, race, consultation reason, and type of COVID-19 test. Results were considered significant at P values less than .05. All statistical analysis was performed using SPSS statistics (IBM Corp, Armonk, NY, USA).
Results
A total of 897 patients underwent an inpatient otolaryngology consultation across all 4 time periods (Table 1). There were 459 individual patient consultations in the 9 pre-COVID months, 79 consultations in the 3 months of Surge 1, 164 consultations in the 4 months of Surge 2, and 195 otolaryngology consultations in the 4 months of Post Surge. There was no significant difference in average age, number of pediatric patients (age <18 years old), or sex between the time periods (Table 1). There were differences in the racial composition of the patients seen between Surge 1, Surge 2, and Post Surge compared to pre-COVID values (Table 1). A higher percentage of patients self-described as Hispanic in Surge 1 (P = .03 vs pre-COVID), while the number of Hispanic patients in Post Surge was decreased compared to pre-COVID characteristics (P = .01). There were also significant differences in patients who refused to disclose their race or identified as “Other” race for all 3 time periods, but otherwise demographic trends were expectedly consistent.
Characteristics of Inpatient Otolaryngology Consultations by Time Period.
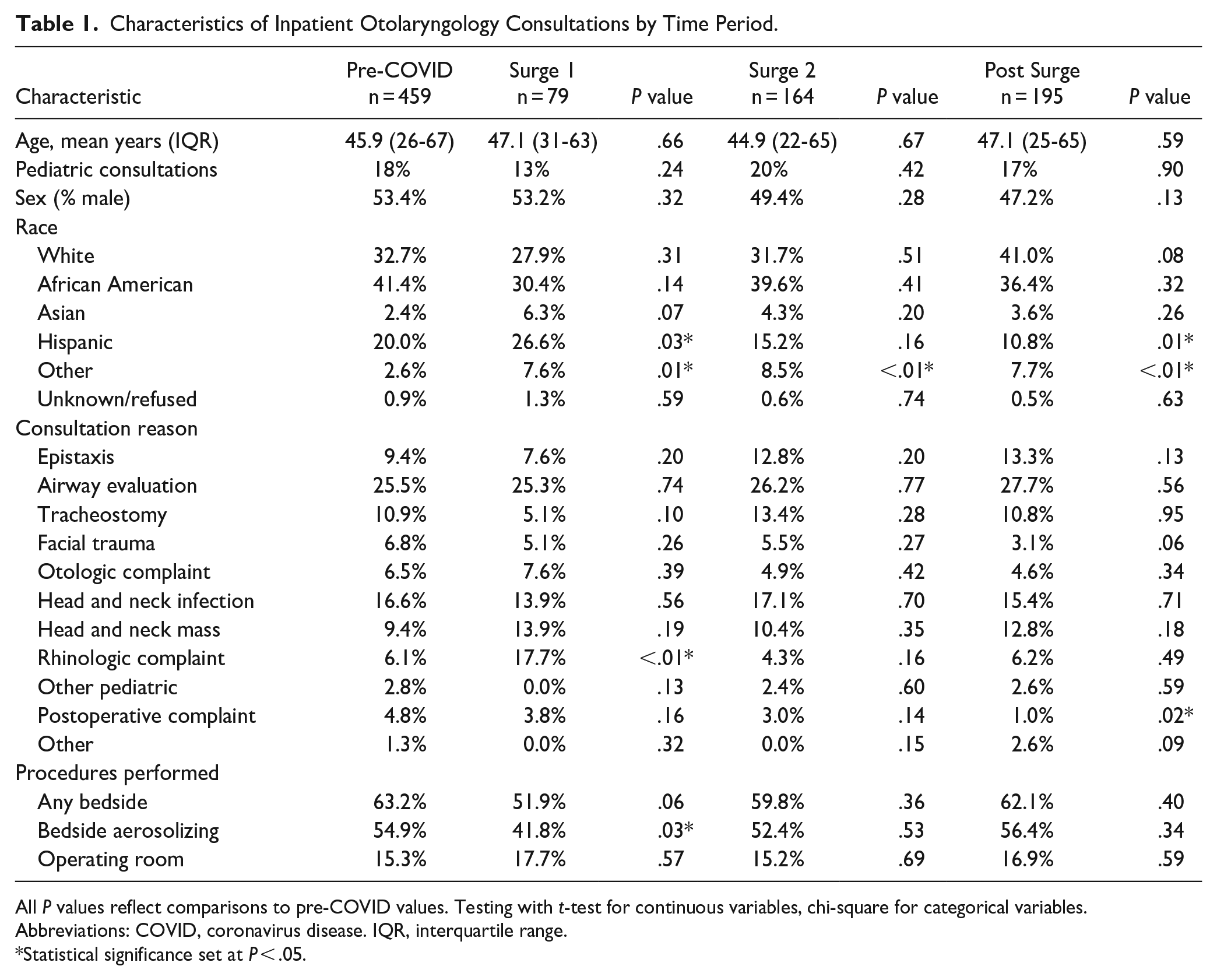
All P values reflect comparisons to pre-COVID values. Testing with t-test for continuous variables, chi-square for categorical variables.
Abbreviations: COVID, coronavirus disease. IQR, interquartile range.
Statistical significance set at P < .05.
The average number of otolaryngology inpatient consultations per day in the pre-COVID time frame was 1.67 ± 0.24. This dropped acutely to 0.86 ± 0.33 consultations per day during Surge 1 (P < .01). The consultation volume did not differ significantly from pre-COVID levels during Surge 2 (1.33 ± 0.35, P = .06) or Post Surge (1.60 ± 0.20, P = .62) (Figure 2). The inpatient consultation volume was restored to pre-COVID levels by Post Surge of the pandemic.

Average inpatient otolaryngology consultations per day by time period. * There were significantly fewer consults in Surge 1 than pre-COVID (P < .01). COVID, coronavirus disease.
Reason for consultation and procedure trends were also studied (Table 1). There were only a few significant trends in consultation reason. Rhinologic consultations increased during Surge 1 and postoperative concerns decreased in frequency in Post Surge. There were some notable procedural trends. There was an initial decrease in bedside aerosolizing procedures in Surge 1 (41.8% vs 54.9%, P = .03) but this trend did not continue, and aerosolizing procedures for inpatient consultations recovered to pre-COVID norms in Post Surge.
There were also several COVID testing trends in this cohort; 30% of consultations in Surge 1 did not have COVID testing results. This number decreased in Surge 2 and Post Surge, although the difference did not reach statistical significance (Table 2). Additionally, there was an increase in the number of Rapid Antigen Screenings in Post Surge compared to Surge 1 (20.1% vs 7.6%, P = .04). Institutional guidelines also changed over time. 8 During the first and second surges pre-procedure “double testing” was required for any patient undergoing an aerosolizing procedure. When this mandate was lifted, there was a predictable decrease in double testing in Post Surge (0.0% vs 3.8% in Surge 1, P = .04).
COVID Testing Trends Across Time Periods During the COVID-19 Pandemic.
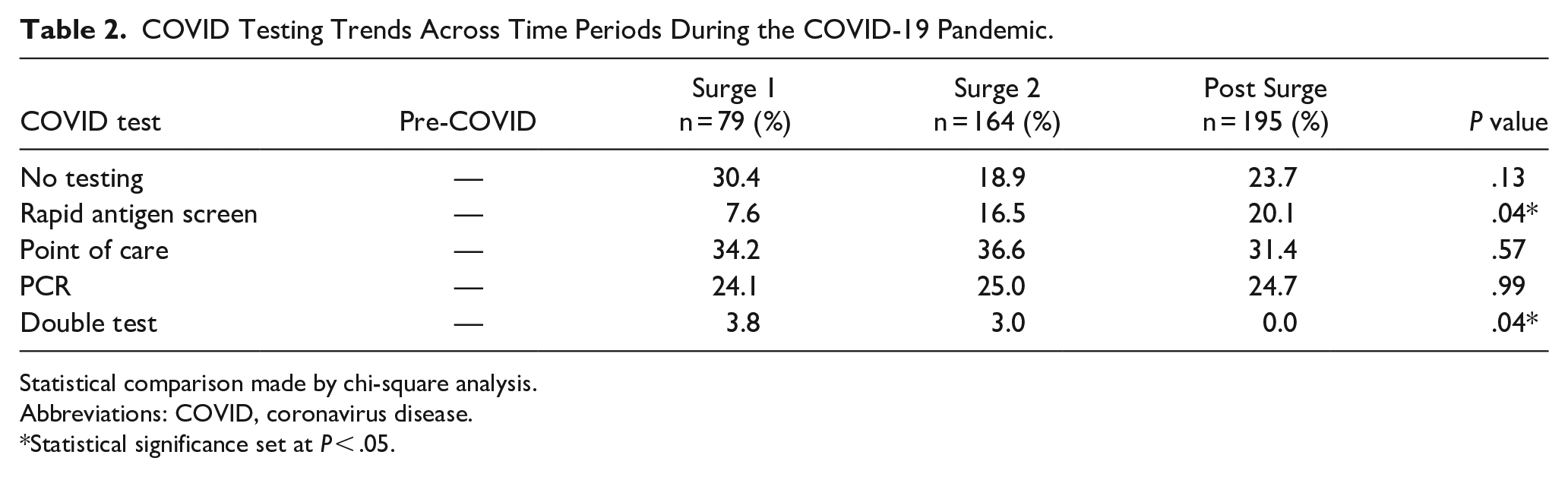
Statistical comparison made by chi-square analysis.
Abbreviations: COVID, coronavirus disease.
Statistical significance set at P < .05.
Lastly, the effect of COVID vaccines was studied. Consultations per day for all months during the pandemic (including interim months not included in the above analysis) stratified by availability of vaccines are reported in Figure 3. There was a significantly higher consultation volume during the vaccine era (1.46 ± 0.38) versus prior to vaccines (1.07 ± 0.26) (P = .027).
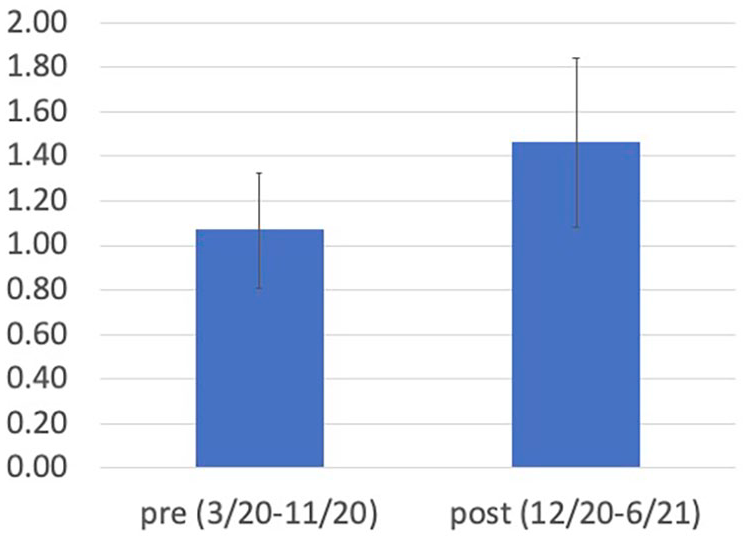
Vaccine impact on otolaryngology consultations. Y axis indicates consultations per day.
Discussion
Inpatient otolaryngology consultation trends in multiple pandemic phases provide useful information for preparation and response to future external stoppages in workflow. In accordance with the data from Dharmarajan et al from University of Pittsburgh 2 and Shomorony et al at Cornell Medical Center in New York 5 , this study identified an acute (nearly 50%) decline in inpatient consultation volumes at this institution during the first COVID-19 surge in Chicago, IL, USA (March 2020-May 2020). The reason for this decline is likely multifactorial. Most notably, fear of viral exposure deterred patients from seeking care. Social distancing and mask mandates prompted a decrease in behaviors which contribute to facial trauma and contagious spread of head and neck infections. Delays in cancer care are well documented.9 -11 Less obvious factors likely played a role as well. Job loss and economic burden prompted many patients to avoid medical care to save money. 11 Additionally, provider consultation and referral behaviors were adjusted both intentionally and unintentionally. In the earliest days of the Surge 1, testing availability and personal protective equipment (PPE) were limited and uncertain.12,13 To ensure provider safety, the otolaryngology department deprioritized performance of aerosolizing procedures on untested patients in both the inpatient and outpatient settings. Consultations for airway evaluation were likely deferred in non-emergent cases. Consulting providers during this phase may have also avoided involving a specialist to reduce patient and staff exposure. Phadke et al found an acute decrease in all specialist consultations in March 2020 in Massachusetts, and a drastic increase in proportion of virtual consultations. 14 While outpatient virtual consultations were quickly adapted by our department, inpatient virtual consultations were more difficult to implement, although this may have stymied some of the acute decline in Surge 1 inpatient volume.
While patients in each time frame were largely similar in demographic characteristics, there was an increase in the proportion of Hispanic patients evaluated during Surge 1. Multiple studies have demonstrated racial disparities in COVID-19 incidence and outcomes.15,16 The variation in the Hispanic population in this study may reflect larger hospital trends at the height of the pandemic.
Like Dharmarajan, we found no major changes versus pre-COVID norms in reasons for consultation during the first surge. 2 Shomorony et al reported an increase in tracheostomy consultations during this period, due to high volumes of patients with COVID-related respiratory failure. 5 However, at our institution, tracheostomies for patients with COVID-19 were performed as both as open (by otolaryngology) and percutaneous closed circuit (by general surgery and pulmonology/critical care), and thus despite a significant influx in patients with COVID-19 hospitalized at our institution, the otolaryngology service did not see a large influx in tracheostomy requests. The relative increase in rhinology consultations was largely due to tumors and complicated infections of the paranasal sinuses and anterior skull base. This may have been secondary to busier intensive care units creating a larger pool of patients with rhinologic symptoms susceptible to progressive infections. This could also have been due to being a large referral center for rhinologic emergencies and advanced pathology, our center received an influx of transfers from outside medical centers that were overwhelmed by COVID-19 and lacked the resources to manage advanced rhinologic pathology, such as tumors or progressive infections. Hyposmia and other COVID-related rhinologic symptoms are more frequently evaluated on an outpatient basis rather than by inpatient consultation and did not contribute to this bump in rhinologic complaints.
Interestingly, the decline in consultation volumes seen in Surge 1 was not replicated in Surge 2. There are a number of likely contributing factors. The number of local cases and deaths was not as drastically high in Surge 2 in comparison to Surge 1 (Figure 1). Also, increased testing and PPE availability likely helped dispel patient and provider fears.17 -19 Overall, 30% of consultations had no testing results during Surge 1, while this number decreased to 18% in Surge 2. General fear of the unknown also was less of a contributing factor during Surge 2. Mixed media messaging and a lack of reliable information during Surge 1 intensified fear of exposure among patients and providers, but the explosion of research and spread of public knowledge likely helped to dampen the fear of avoidance during later surges. 19 “Pandemic fatigue” is also contributory.18,20 After the early surge, it became increasingly burdensome to maintain strict behavioral change for the long term. Lifting of mandates resulted in a return to previously normal activities among both patients and providers stimulating a trend toward pre-COVID consultation patterns.
Lastly, 2 of the vaccinations approved for use in the United States became available at our institution during Surge 2. The Food & Drug Administration issued an Emergency Use Authorization (EUA) for the 2-dose Pfizer/BioNTech vaccination on December 11, 2020 and an EUA for the 2-dose Moderna vaccination on December 18, 2020. The single-dose Johnson & Johnson vaccination was approved at a later time (February 27, 2021). 19 Introduction of vaccines helped to protect individuals from serious complications, lift social distancing regulations, and prompt a return to pre-pandemic behaviors. Vaccines likely played a role in returning inpatient otolaryngology patterns to pre-COVID norms, although it is difficult to determine how much of the effect is directly attributed to vaccines, since volumes began to trend upward prior to vaccine introduction as discussed above.
Overall, by Post Surge, inpatient consultations and procedures mirrored pre-COVID patterns. The only variation in Post Surge consultations was a decrease in postoperative complaints, defined as any patient presenting for a concern stemming from a recent otolaryngology procedure, except for a complaint of epistaxis which was classified separately. This may be due to a decrease in surgical volumes during the preceding surges, or could alternatively be a result of sampling error in a small group. The most common postoperative complaints across all time periods were surgical site hemorrhage, possible infection, respiratory concerns, and dysphagia. The authors hypothesized that lasting effects of the pandemic would result in narrowed breadth or lower volumes of inpatient consultations, but are relieved to see such a rapid return to pre-COVID norms even as the pandemic continues. A busy inpatient consultation service is important to the department’s academic mission in patient care and particularly resident education. 21 Although this study looked specifically at inpatient consultations, trends in outpatient otolaryngology likely mirror those observed here. 22 While post-initial surge outpatient otolaryngology data are not yet readily available, Zhao et al characterized a slower recovery for outpatient in person services in stroke and neurology patients versus inpatient services. 23 This may be in-part due to a prioritization of telemedicine and patients continuing to utilize outpatient virtual care services. 23
There are a number of limitations to this study, which bear noting. As a retrospective chart review, the data are limited to the information reported in the EMR. Although hospital policy dictates an electronic consultation, data could be missed for consultation requests which were placed only by phone without an associated order in EMR. This policy; however, did not change over the time frame studied and is unlikely to impact the reported trends. Further, reallocation of nurses, advanced practice providers, and other stuff to the busiest units (intensive care units, medical floors) during peak months may have impacted existing resources and consultation patterns. In addition, the COVID-19 time periods selected for this study were based specifically on COVID-19 cases in Chicago and may vary if compared to other locations and infection burden. Consultation patterns demonstrate some seasonal variation, which is difficult to control in the setting of surge timing. The pre-COVID period was extended across multiple seasons to attempt to account for seasonal variation. Also, although there were a large number of patients captured, the possibility of sampling error, particularly in small subgroups exists. Lastly, these results reflect an individual institutional experience. As demonstrated by the March 2020 data from Pittsburgh 2 and New York City 5 , there is a significant geographic and institutional variation in pandemic practice patterns. The authors hope that this data supporting a strong recovery for inpatient otolaryngology volumes at our institution are replicated at other centers in the United States as the inpatient medical landscape recovers.
Conclusions
There were no lasting deleterious effects in breadth or volume of inpatient otolaryngology consultations at an urban, academic institution in Post Surge (March 2021-June 2021) of the COVID-19 pandemic compared to Surge 1 and 2 time frames. Initial nadirs in consult volumes and bedside aerosolizing procedures during Surge 1 recovered to near pre-COVID levels despite ongoing infections and hospitalizations. Surge 2 did not replicate the loss in volume seen during Surge 1. Factors which contributed to rapid recovery of inpatient services included increased testing availability, security of PPE resources, vaccination, “pandemic fatigue,” relaxation of behavioral mandates, and expanded public knowledge resulting in less fear of viral exposure.
Footnotes
Acknowledgements
The authors would like to acknowledge the Rush University Medical Center otolaryngology physicians, residents, and staff for their unwavering dedication to patient care in the midst of unprecedented circumstance.
Authors’ Note
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Rush University Medical Center Institutional Review Board, Chicago, IL (No. 21062104).
Statement of Informed Consent
Informed consent for patient information to be published in this article was not obtained because this study was granted an exemption by the Rush University Medical Center Institutional Review Board, Chicago, IL (No. 21062104) due to this study being declared secondary research for which consent is not required due to the information regarding human subjects being de-identified, the subjects were not contacted, and the subjects were not re-identified.
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the Rush University Medical Center Institutional Review Board (No. 21062104) approved protocols.