
Abstract
Introduction
Otolaryngologists were among the physicians with the highest risk of exposure to SARS-CoV-2, and more than half of them reported anxiety and distress during the pandemic. Consequences of this experience on retirement plans among otolaryngologists are unknown. This study aimed to describe the effect of the pandemic on retirement plans among otolaryngologists.
Methods
A cross-sectional survey assessed retirement plans of physicians in the Canadian Society of Otolaryngology-Head and Neck Surgery (CSOHNS) between May and June 2023. Participants were recruited through CSOHNS membership lists. Respondents shared demographic information and rated 4 pandemic-related factors and 13 independent factors on a 5-point Likert scale from least important to most important in influencing retirement.
Results
Eighty-two members responded, of which 20 (24.4%) were females. All female participants were 65 or younger, whereas 25 (40.3%) males were 65 or older. Half of the participants were in academic practice; 39% reported no change to their anticipated retirement date prior to the pandemic, whereas 25% reported either earlier or later dates. A greater proportion of female otolaryngologists reported earlier dates of retirement than originally planned compared with males (40% vs 19.3%). The factors most commonly rated as “important” were the desire for time with loved ones (mean: 3.82, SD: 1.179), the desire to improve their quality of life (mean: 3.65, SD: 1.344), and increased workload (mean: 3.26, SD: 1.210). Significant differences were observed between genders and age groups (≤55 years vs >55 years) regarding increased workload, desire for improved quality of life, personal and loved ones’ health concerns, pandemic-related concerns, psychological/emotional issues, and burnout (P < .05).
Conclusions
Pandemic-related factors play a limited role in retirement decisions made by otolaryngologists. More females reported earlier retirement dates after the pandemic, which may further exacerbate preexisting gender inequalities in the otolaryngology workforce.

Introduction
The COVID-19 pandemic exerted a significant toll on health care professionals globally, leading to increased stress and worsened mental and physical health among physicians. The feeling of emotional, mental, and exhaustion due to personal distress and a strenuous environment, known as burnout, was exacerbated in otolaryngology where physicians were regularly exposed to respiratory secretions.1-3 Worsened emotional health among otolaryngologists was also concurrent with increased rates of insomnia and alcohol consumption.4,5
While the immediate negative effects of the pandemic on otolaryngologists are well-documented, no prior reports examine the long-term consequences among physicians who were at high-risk of exposure to SARS-CoV-2. Namely, among these repercussions is the decision to retire from practice. The primary objective of this study was to evaluate the factors impacting retirement plans among otolaryngologists after the pandemic.
Methods
Study Participants and Data Collection
IRB approval from the University of Buffalo Institutional Review Board (IRB: STUDY00007192) was obtained prior to the initiation of this cross-sectional study. An online survey was disseminated to members of the Canadian Society of Otolaryngology-Head and Neck Surgery (CSOHNS) from May to June of 2023. Demographic variables included age, gender, race, location of practice, subspecialty, and employment status.
Participants rated 17 factors on a 5-point Likert scale from least to most important in influencing their retirement decision. Thirteen factors were independent of the pandemic. These were as follows: planned retirement age, employer mandates, job-related challenges due to age, onerous workload, insurance complexities, continuing medical education (CME) requirements, seeking an improved quality of life, fostering family connections, addressing personal or family health matters, burnout, and career changes. The remaining 4 factors were pandemic related: new financial concerns, COVID-related personal or family health concerns, and pandemic-related psychological concerns. Participants were required to respond to all the questions to complete the survey.
Statistical Analysis
All statistical analysis was performed using SPSS (IBM Corp, Armonk, NY, USA). Demographic and categorical response variables were analyzed using nonparametric methods. To assess the relationship between Likert ratings and demographic characteristics, univariable and multivariable regression analysis was employed. The Mann-Whitney U test was used to determine whether there were differences in Likert ratings based on age, gender, and race of participants. P ≤ .05 was considered statistically significant.
Results
Eighty-two (14%) members responded. Participant demographics are displayed in Table 1. The majority of participants were older than 55 years (74.4%), Caucasian (74.4%), and married (84.1%). Participants were primarily located in Ontario (39%), although there was representation from all the Canadian provinces and the Canadian diaspora. Respondents represented all the subspecialties of otolaryngology, with the largest proportion being comprehensive otolaryngologists (45.1%). The majority of participants worked full time (72%) and engaged in teaching (59%).
Patient Demographics, N = 82.

Retirement decisions are shown in Table 2. Most participants planned for full (42.7%) or part-time retirement (36.6%) before the year 2031 (59.8%). Most participants reported no change to their retirement date after the pandemic (39.5%), with similar proportions reporting earlier (24.4%) or later (25.6%) retirement dates.
Retirement Decisions of Participants, N = 82.

Factors related to the pandemic were considered less influential on retirement decisions than non-pandemic-related factors (Figure 1). The top 5 factors influencing retirement plan were as follows: desire to spend more time with family and friends (mean: 3.82, SD: 1.179), desire to improve personal quality of life (mean: 3.65, SD: 1.344), increased workload (mean: 3.26, SD: 1.210), mental exhaustion or “burnout” (mean: 3.13, SD: 1.310), and age-related job challenges (mean: 2.83). Financial concerns and health concerns of a loved one were rated as the least important factors influencing retirement.

Likert scale results. Independent factors were more influential to retirement than pandemic-related factors. The mean of independent factor ratings was 2.39, compared with a mean of 1.41 for pandemic-related factors.
Significant gender and age-based differences were observed in the motivations driving retirement decisions (Table 2, Figure 2). Women placed higher importance on factors such as increased workload (P = .005), the aspiration to enhance their quality of life (P = .001), health concerns in oneself (P = .005), health concerns in a loved one (P = .003), and mental fatigue or burnout (P = .005). Among the pandemic-related factors, women rated mental health concerns stemming from the pandemic (P = .004), pandemic-related health concerns in oneself (P = .003), and health concerns of a loved one (P = .004) as significantly-more important to retirement than their male counterparts.
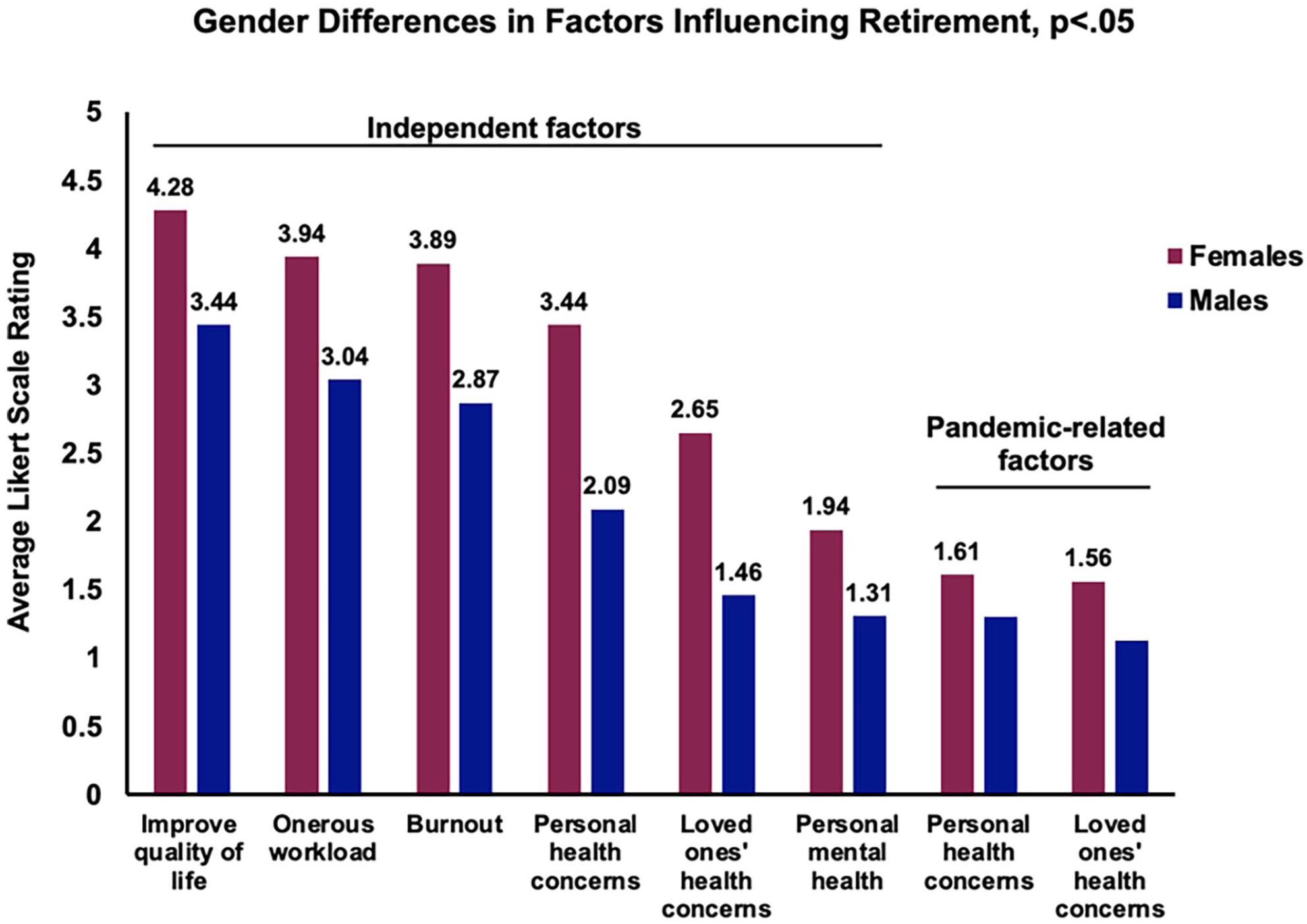
Gender differences in Likert scale results. Female otolaryngologists rated factors related to bettering one’s personal life, challenging workload, and health concerns as more important to retirement.
Factors that were significantly different among participants younger than 55 and 55 and older were increased workload (P = .002), burnout (P < .001), desire to spend time with loved ones (P = .001), the desire to improve quality of life (P = .007), and psychological/emotional issues from the pandemic (P < .006). Each of these factors was rated as more important for retirement among younger professionals than their older counterparts. No statistically-significant differences were found between races regarding reasons for retirement.
Discussion
To our knowledge, this is the first study exploring factors impacting retirement among otolaryngologists. A key finding is that 45% of our respondents plan to retire by the year 2030. However, given the low response rate of 14% and the potential for responder bias—particularly among older otolaryngologists and those in academic practice—this finding should be interpreted with caution. The most influential factors driving retirement plans pertained to workload, improving one’s quality of life, and spending time with loved ones. Despite the initial suspension of elective procedures with the onset of the pandemic, otolaryngologists faced an increased workload, significantly influencing the retirement considerations of some Canadian otolaryngologists based on our findings. An analysis of our open-ended responses from participants revealed that an increased workload during the pandemic was a common stressor, with respondents expressing difficulties meeting patients’ needs. 3 This suggests that, while pandemic-related factors were noted, they were not the primary drivers of retirement decisions compared with nonrelated factors such as personal well-being and family time. While the pandemic-specific factors such as direct exposure to COVID-19 or financial instability were not primary drivers of retirement, the pandemic may have indirectly contributed to burnout and workload issues, which were prominent concerns in our study population.
The growing impact of mental health issues on health care providers, particularly in influencing decisions related to retirement, is further underscored by our study. It is critical to note, however, that the mental health of physicians has been a critical concern even before the COVID-19 pandemic, with studies showing that over half of all physicians faced burnout and approximately 30% of surgeons suffered from depressive symptoms.6,7 These challenges are compounded by the high demands and stress of medical practice, often leading physicians to prioritize personal life quality and family time when considering retirement. 8 Recent findings have revealed a notable shift in the factors causing burnout, moving from work and academic pressures in 2018 to patient care and family responsibilities in 2020. 9 This shift mirrors the changes observed in our study and may reflect the broader transformation of health care work dynamics during this period. Supporting this, a national survey conducted during the pandemic highlighted that up to 60% of otolaryngologists reported stress, with 22% experiencing burnout. 4 Furthermore, a correlation between the pandemic’s intensity and mental health outcomes has been previously reported, finding that physicians in regions with over 20,000 COVID-19 cases or 1000 deaths reported increased symptoms of distress, underscoring the pandemic’s uneven impact on the mental well-being of health care providers. 4
Our study highlights gender disparities in retirement decisions among otolaryngologists, likely due to the heightened challenges female physicians encountered during the pandemic. It has been frequently shown that female health care workers experience higher levels of burnout, anxiety, and distress than their male counterparts.10-14 Poor mental health, in turn, has been linked to a higher rate of retirement in women, as well as a general increase in workforce exit. 15 Notably, studies have found chronic low work-related stress to be associated with poor health-related quality of life, advising that risk management should consider socio-demographic factors like gender, education, and age.16,18 Outside of work-related stressors, female physicians have devoted more time to home and family care activities than their male counterparts, a disparity that the pandemic further exacerbated by disrupting schedules, especially in managing child and family-related responsibilities.17,18 Moreover, late-career female faculty report unique factors influencing retirement decisions, such as health insurance, burnout, lack of career resources, and caregiving responsibilities, all contributing to a gender-based divergence in career trajectories. 19 Increased workload and burnout, traditionally-considered “non-pandemic” variables, may have been exacerbated by the shifting dynamics of patient care and additional responsibilities introduced during the pandemic, disproportionately impacting female physicians. These trends indicate that female gender is a significant predictor of stress levels among health care professionals, underscoring the need for targeted interventions to support female physicians’ well-being and career longevity. 20
To address the complexity of physician burnout, a blend of interventions is crucial. Enhancing communication, strengthening teamwork, and implementing participatory programs, complemented by psychological practices such as yoga, meditation, and mindfulness, have shown efficacy in mitigating burnout effectively. 21 Organizational strategies, particularly those that enhance leadership, autonomy, collegiality, and electronic health record (EMR) usability, are equally vital in diminishing burnout and augmenting professional fulfillment.22,23 Professional coaching has also demonstrated efficacy in reducing emotional exhaustion and fostering resilience and a better quality of life for physicians. 1 Among otolaryngologists specifically, simplifying administrative tasks, for example, by employing scribes and enhancing EMR features, can alleviate significant stressors, contributing to well-being and lessening burnout. 9 Thus, interventions need to be multifaceted, targeting the myriad causes of burnout with a range of therapeutic tools for a comprehensive, sustainable impact. 24 This approach underscores the collective endeavor required to support the well-being of physicians in a demanding health care environment.
Limitations
Our study faced several limitations. The low response rate raises the possibility of nonresponse bias, as nonresponding providers may not have experienced distress or burnout, thus opting not to participate. Our response rate of 14% is below the threshold suggested to minimize nonresponse bias, although it parallels previous surveys conducted through the CSOHNS.25,26 The overrepresentation of older otolaryngologists and those in academic practice limits the ability to generalize our findings to the broader population of Canadian otolaryngologists. Additionally, the lack of a pre-pandemic cohort means that it is unclear whether the reported symptoms represent preexisting mental health conditions or are newly developed. The cross-sectional nature of the survey further restricts our ability to make causal inferences. However, optional free-text survey responses indicate that numerous participants attribute their mental shifts to be unrelated to the COVID-19 pandemic. Lastly, while our survey captured a range of factors influencing retirement, the nuanced interplay between these factors and the pandemic’s impact requires more in-depth, longitudinal studies to fully understand their effects. These limitations, however, do not preclude the primary goal of our study, which was to evaluate retirement decisions among otolaryngologists after experiencing worsened mental and physical health during the pandemic.
Conclusions
In conclusion, our study provides an exploratory assessment of retirement plans among Canadian otolaryngologists in the aftermath of the COVID-19 pandemic. While pandemic-related factors appeared to play a limited role overall, individual considerations such as workload, burnout, and quality of life significantly influenced retirement decisions for some respondents. Gender disparities were evident, with female otolaryngologists more likely to report earlier retirement, highlighting the need for targeted support and interventions to address these challenges. Given the limitations of our study, our findings should be interpreted with caution, To address these disparities, future research should investigate the impact of possible wellness-oriented strategies such as reducing administrative burdens through hiring medical scribes and enhancing EMR systems, minimizing work-related activities outside of work hours, enhancing mental health and work-life balance support systems, and developing policies that address gender disparities. These measures should aim to support the well-being and career longevity of otolaryngologists, especially under the additional stressors introduced by the pandemic, and contribute to a more equitable and effective medical workforce.
Footnotes
Acknowledgements
None.
Author Contributions
All authors contributed to study conception and design. Material preparation and data collection were performed by Nick Sahlollbey, Arunima Vijay, and Michele Carr. All authors contributed to data analysis and interpretation, as well as the first draft of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study received IRB approval from the University at Buffalo Institutional Review Board (IRB: STUDY00007192), which was obtained prior to the initiation of this study.