
Abstract

Significance Statement
Sino-nasal malignant melanoma is a rare malignant tumor with a poor prognosis. Since clinical symptoms are nonspecific, the spread may be extensive at the time of diagnosis. Wide surgical resection, which is the first option in treatment, may not be possible due to delay in diagnosis. In typical malignant melanoma patients, MRI images are useful and robust in diagnosis. CT is useful in showing the destruction of adjacent bone structures.
A 60-year-old male patient was admitted to our center with obstruction in the left nasal cavity and occasional epistaxis which had worsened in the last 3 months. There was occasional accompanying headache. The patient had no known disease and had been smoking for about 30 years. On examination, there was a lobule contoured, black mass lesion filling the left nasal cavity. No significant lymphadenopathy was detected in the neck. Paranasal computed tomography (CT) without contrast was performed. The images showed a soft tissue dense mass lesion filling the left nasal cavity. There was significant destruction of the posterior wall of the frontal sinus and cribriform plate (Figure 1). Contrast-enhanced paranasal magnetic resonance imaging (MRI) was performed to clearly define the borders of the lesion. The lesion was approximately 6 cm × 5 cm × 4 cm in size with marked hyperintense areas on T1-weighted images and hypointense areas on T2-weighted images (Figure 2). It was diffusion restricted and markedly contrast enhanced. Increased dural thickness and contrast enhancement were detected in the neighborhood of the frontal bone, which showed destruction on CT. Histopathologic examination of the biopsy obtained from the mass revealed a diagnosis of malignant melanoma. Positron emission tomography (PET-CT) performed for possible metastasis showed no involvement other than the mass. The patient was considered inoperable and radiotherapy was planned.
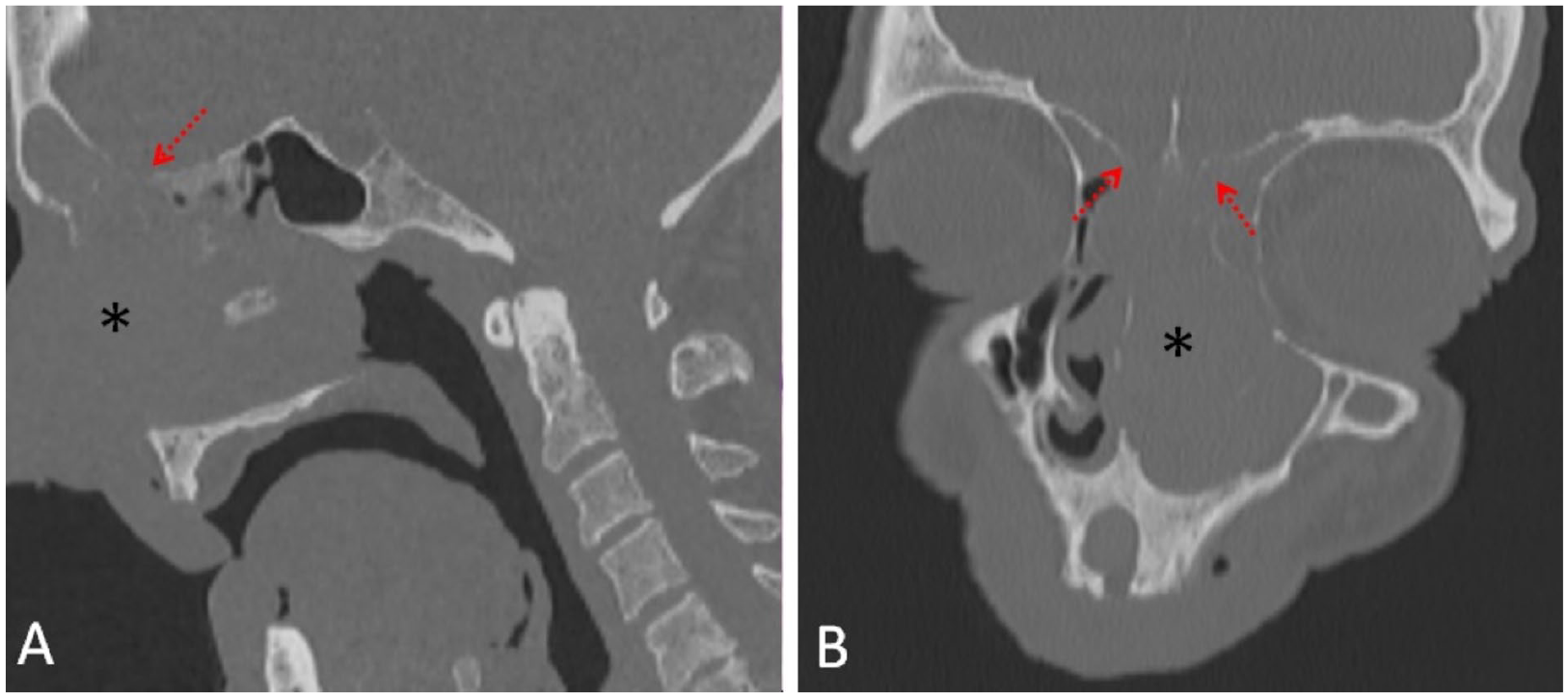
Sagittal (A) and coronal (B) non-contrast CT images show an expansile soft tissue dense mass lesion (asterisk) filling the left nasal cavity. The lesion shows marked destruction of the frontal bone (arrows).
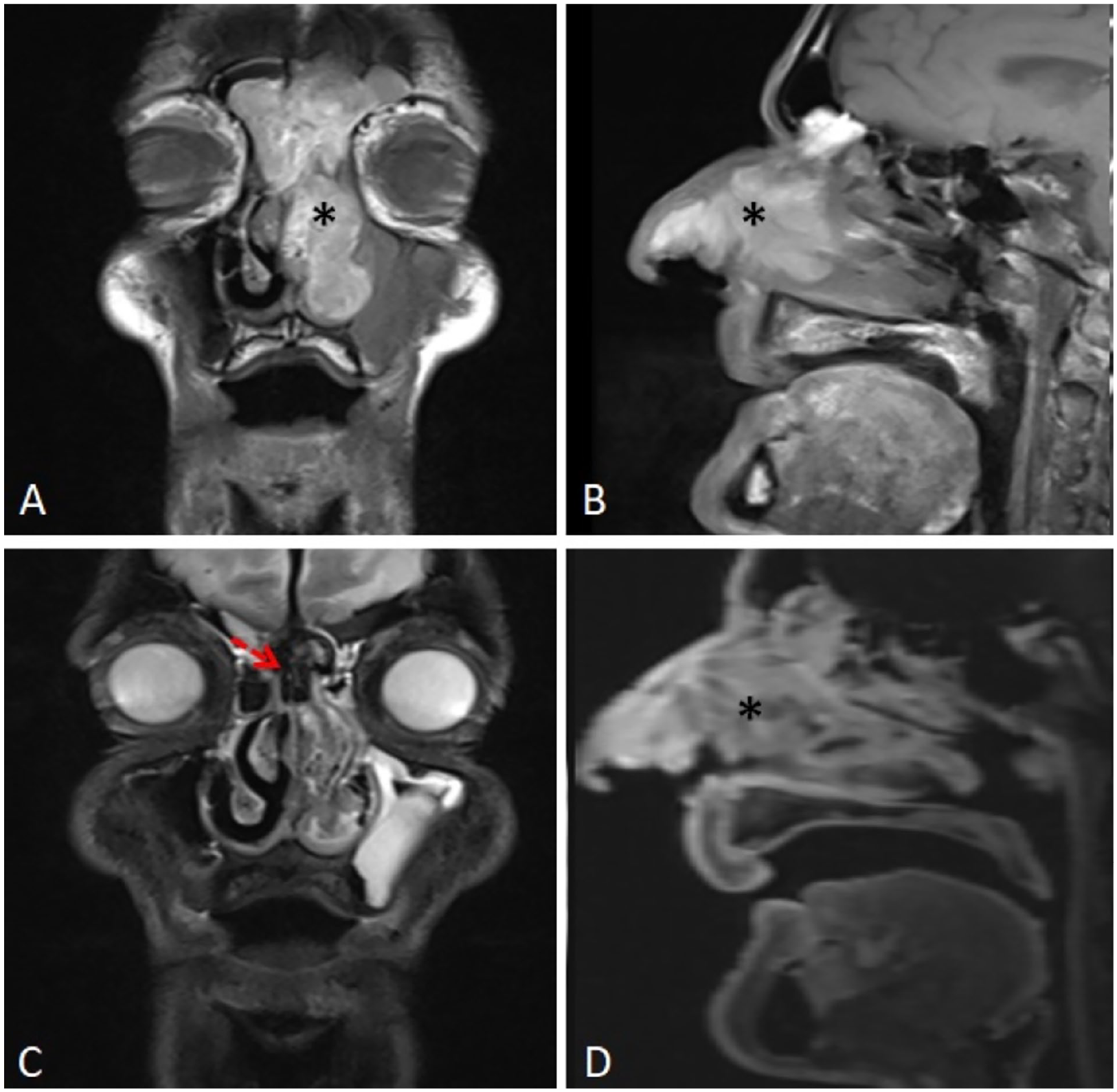
On T1-weighted coronal (A) and sagittal (B) images of malignant melanoma in the left nasal cavity, the mass lesion (asterisk) is markedly hyperintense. On the T2-weighted coronal section (C), hypointense areas within the lesion are prominent (arrow). Postcontrast substraction sagittal section (D) shows a prominent contrast enhancement of the mass lesion (asterisk).
Sino-nasal malignant melanoma is a rare malignancy with a worse prognosis. It constitutes approximately 1% of all malignant melanomas and 4% of head and neck malignant melanomas. 1,2 It occurs equally in men and women and the peak age is seventh decade. 3,4 Approximately 80% of sino-nasal melanomas originate from the nasal cavity, while the rest from the sinus. The frequency of localization in the nasal cavity respectively is the lateral nasal wall, middle and inferior turbinate, and nasal septum. 1 Exposure to sunlight, formaldehyde inhalation, and smoking are among the main risk factors. 5 Clinical symptoms are nonspecific such as nasal congestion, epistaxis, swelling of the nose, and a mass that may be pigmented. Since the symptoms are usually ignored, diplopia, epiphora, and ophthalmoplegia may be observed with the spread of the mass. 1,3 In many cases of malignant melanoma, MRI is helpful in diagnosis and shows typical features. Melanin and hemorrhage within the mass appear hyperintense on T1-weighted images and hypointense on T2-weighted images. This allows differential diagnosis with various solid lesions. 5 Although CT does not play a role in the differential diagnosis of the lesion, it is useful in demonstrating destruction and remodeling of adjacent bone structures. 4 Definitive diagnosis is made histopathologically. 3 The preferred method of treatment is surgical resection with wide margins. However, this is not always possible due to wide spread. Although they are resistant, radiotherapy is used in local recurrences, but it has no effect on survival. Chemotherapy can be used in metastatic cases and for palliative purposes. The prognosis in this condition is poor, with a 5-year survival rate of <40%. Local recurrence is common and metastases are frequently seen in the lung, liver, bone, and brain. 1,5
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.