
Abstract
Sialolithiasis is one of the most common diseases of salivary glands. More than 80% of the sialoliths occur in the submandibular gland. While most of the calculi are less than 10 mm in size, 7.6% are larger than 15 mm and are classified as giant sialoliths. We demonstrate a rare case of asymptomatic giant sialolith in the left Wharton’s duct with a total atrophy of the left submandibular salivary gland. A 48-year-old female patient presented with lumping sensation for 1 month. A left mouth floor mass was found accidentally during examination and was later revealed to be a painless sialolithiasis. Image study revealed a giant sialolith in the left Wharton’s duct with duct dilatation and left submandibular gland total atrophy. She underwent transoral sialolithotomy with removal of a huge stone, measuring 3.5 × 1.4 cm in size. Sialolithiasis usually presents with typical symptoms of the involved salivary gland, and the size of calculi is usually less than 20 mm. This is a rare case report of an asymptomatic giant sialolith in the Wharton’s duct, causing left submandibular salivary gland total atrophy, and its diagnosis and management.
Introduction
Sialolithiasis is one of the most common diseases of salivary glands and the most common cause of salivary swellings, obstructions, and infections. It affects 0.1% to 1.0% of the adult population around the world, typically between the ages of 30 and 60 years. 1 Males are affected twice as much as females, but children are rarely affected. 2 More than 80% of the sialoliths occur in the submandibular gland, 6% in the parotid gland, and 2% in the sublingual gland or minor salivary glands.3 -5 The size of the sialolith is variable. Most of the calculi (88%) are less than 10 mm in size, whereas only 7.6% are larger than 15 mm and classified as giant sialoliths. 6 They consist of mainly calcium phosphate with smaller amounts of hydroxyapatite, magnesium, potassium, and ammonia. Bacterial elements have not been identified at the core of a sialolith. 7
Case Report
A 48-year-old woman with underlying disease of iron-deficiency anemia presented at our clinic with lumping sensation for 1 month. Previously, she had underwent biopsy of a benign right tongue tumor at another hospital and visited our outpatient department for a second opinion on the therapeutic plan. On clinical examination, we accidentally found a painless solid mass of 3 × 2 cm in the left mouth floor (Figure 1). The oral mucosa with increased vascularity was otherwise normal in appearance. The texture of the mouth floor mass was indurated without tenderness. She denied oral pain, sore throat, odynophagia, and left upper neck swelling. She reported no past history of sialadenitis. Besides, the global sensation did not exacerbate while eating or drinking. A flexible nasopharyngoscopy was performed, revealing laryngopharyngeal reflux without visible mass in the pharynx or larynx. Computed tomography was arranged, considering the possibility of a left mouth floor tumor, which demonstrated a giant sialolith about 3.4 × 1.4 cm in the left Wharton’s duct with left submandibular duct dilatation and left submandibular gland total atrophy (Figure 2). The patient was admitted for surgical intervention. There was no leukocytosis from the blood test and all preoperative examinations were within normal limits. She underwent wide excision of right tongue tumor and transoral sialolithotomy under general anesthesia (Figures 3 and 4). The large stone was removed smoothly in a single piece, measuring 3.5 cm in length and 1.4cm in diameter (Figure 5). After the operation, the patient recovered well and was discharged 4 days later.
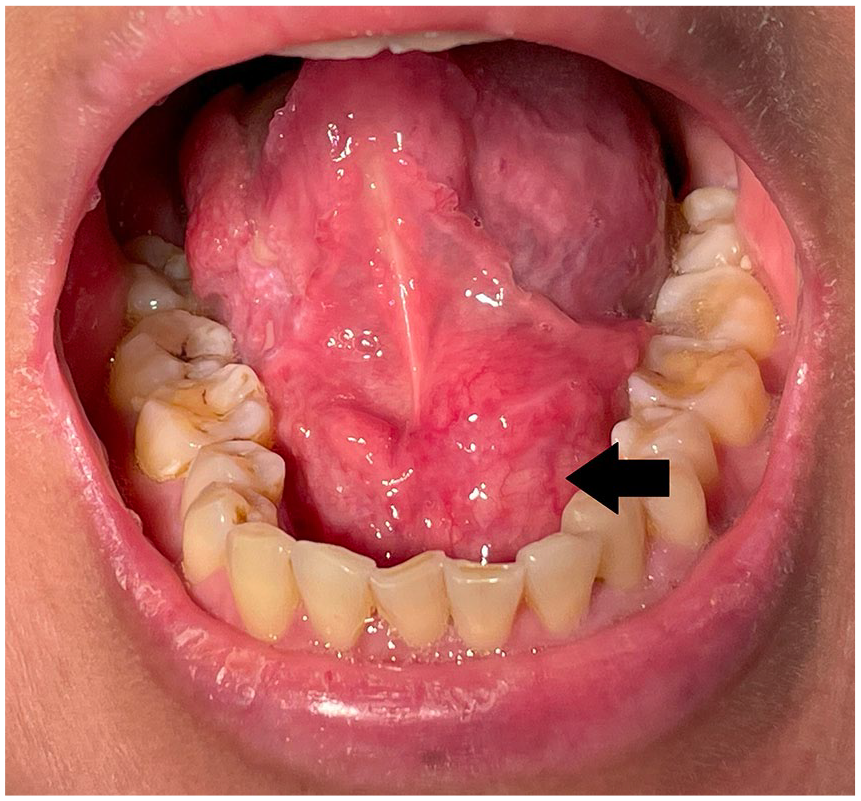
Left mouth floor sialolithiasis (arrow).
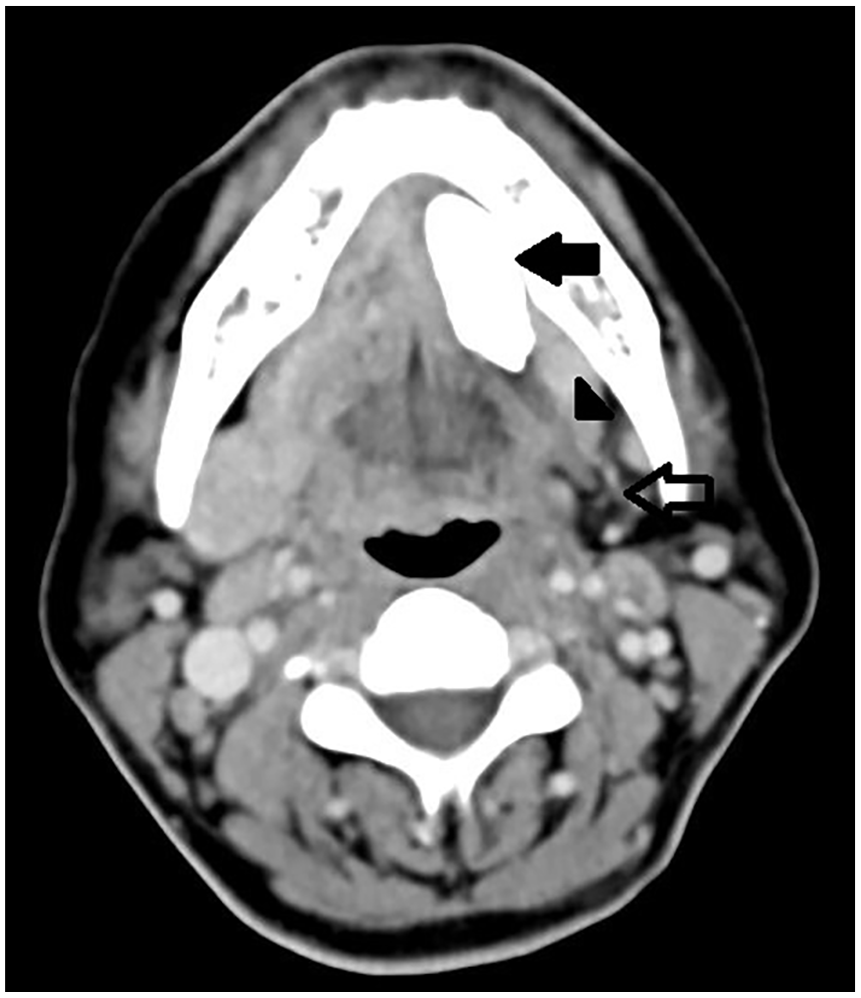
A giant calcification (arrow) deposit in left Wharton’s duct with left Wharton’s duct dilatation (arrow head). The patient’s left submandibular salivary gland had also atrophied (hollow arrow).

A huge sialolith was identified in the left Wharton’s duct during transoral sialolithotomy.
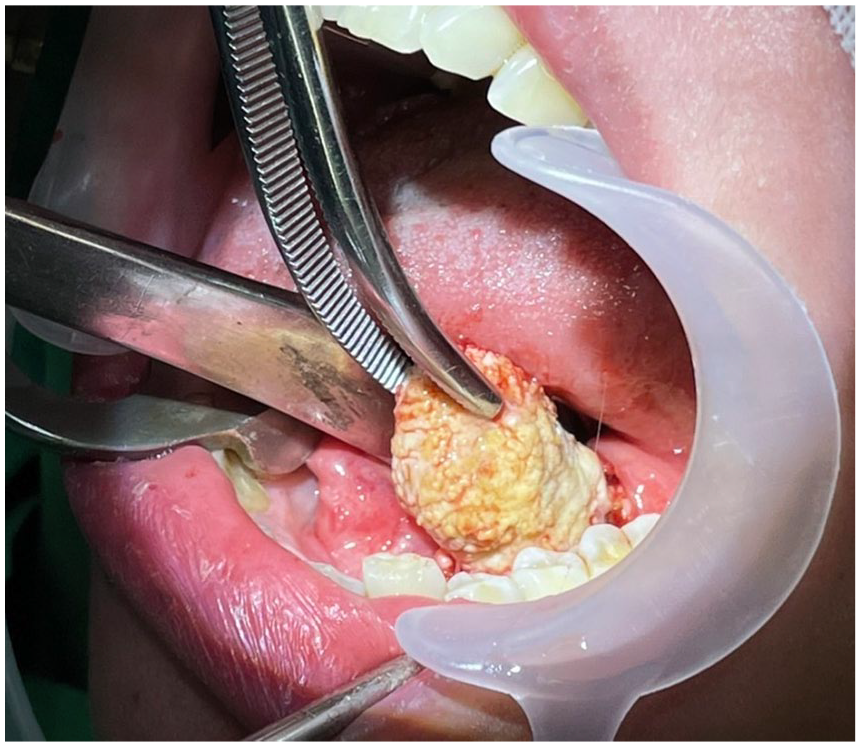
Transoral sialolithotomy was performed with smooth removal of giant stone.

A giant sialolith of submandibular salivary gland duct measuring 3.5 × 1.4 cm.
Discussion
The symptoms of sialolithiasis typically cause pain or swelling of the involved salivary gland and are usually associated with eating. These symptoms may vary from mild discomfort to severe pain and can be accompanied by neck swelling or trismus. In some cases, it can also be completely asymptomatic. The exact etiology and pathogenesis of sialolith are largely unknown. Genesis of calculi lies in the relative stagnation of calcium-rich saliva. They are thought to occur as a result of deposition of calcium salts around an initial organic nidus consisting of altered salivary mucins, bacteria, and desquamated epithelial cells.2,8 Presence of infection, inflammation, stasis of saliva, and physical trauma tends to be the epicenter for precipitation of mineral salts that consequently plays a role in pathogenesis of salivary gland calculi. 9 Salivary calculus is usually small and measures less than 15 mm. The mean size is reported as 6 to 9 mm according to previous literature. 6 The larger size that is bigger than 20 mm is extremely rare in the available literature. The treatment objective for salivary calculi is restoration of normal salivary secretion. If the salivary stone is small, conservative management may be attempted with local heat, massage, and sialogogues. 7 In addition, infection should be treated with antibiotics and analgesic agents. Simple sialolithotomy may be required in some cases. For giant sialoliths, transoral sialolithotomy with sialodochoplasty or sialadenectomy remains the mainstay of management. 10 In some cases, excision of the entire gland is required but had a risk of permanent or temporary marginal mandibular nerve palsy. 10 For our patient, we chose to perform transoral sialolithotomy, a minimally invasive procedure for giant sialolith removal, so as to avoid other associated complications.
Long-term obstruction of calculus in the absence of infection can lead to atrophy of the gland with resultant lack of secretory function and ultimately fibrosis. 11 In this case, with the finding of left submandibular atrophy, we suspected that the giant calculus had been present insidiously and must have grown gradually over a long period of time, causing asymptomatic chronic sialadenitis.
Conclusion
Sialolithiasis typically causes pain and swelling of the involved salivary gland, and the size of a calculus more than 20 mm is very unusual. There are various methods available for the management of salivary stones, depending on the gland affected and stone location.
Our case report demonstrates a rare asymptomatic giant sialolith in the left Wharton’s duct with left submandibular salivary gland total atrophy.
Footnotes
Data Availability Statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the institutional ethical review board of Far Eastern Memorial Hospital, New Taipei City, Taiwan.
Statement of Informed Consent
Verbal informed consent was obtained from the patient for their anonymized information to be published in this article.