
Abstract
Objectives:
Insertion of mold material into the middle ear is a complication of molding procedure for ear impression. These cases are referred to an ENT specialist. There is no standardized approach to this problem. Literature shows different clinical strategies. The aim of this study is to share our experience and to analyze the adverse outcome of different clinical approaches.
Methods:
A case series of six patients with molding material inside the middle ear after complicated molding procedure for swimming earplugs are described. Additionally, available literature was reviewed to analyze results of the clinical approach after iatrogenic molding procedures. Forty-nine ears were included.
Results:
In-office removal of the material is associated with a significant risk of adverse outcome if the eardrum cannot be examined. This also accounts for ossicular involvement.
Conclusions:
Temporal bone CT is advised in patients after complicated ear mold fitting if the tympanic membrane cannot be examined completely or the middle ear is involved. Blind removal should be avoided. Retroauricular transcanal tympanotomy or transmastoidal tympanotomy with facial recess approach is best practice in case the mold material has entered the middle ear. A clinical treatment algorithm is presented.
Keywords
Introduction
The use of customized swimming plugs is regularly advised to children and adults with ventilation tubes and tympanic membrane perforation to prevent middle ear infections in the Netherlands. 1 Hearing aid impressions are fabricated according to a similar procedure. The procedure is well described and has safety measures including minimum training requirements in order to protect the tympanic membrane and middle ear.2,3 In the Netherlands, hearing aid professionals are officially trained to fabricate these ear impressions.
Taking an ear impression seems relatively simple; however, when incorrectly executed it can have adverse consequences for the patient. Symptoms of otalgia, tinnitus, vertigo, and hearing loss due to the molding procedure are suggestive for iatrogenic damage.4-7 In ears with pre-existing tympanic membrane perforation or ventilation tubes, there is a higher risk of deposition of mold impression material in the middle ear. 4
Once referred, there are no guidelines on how to approach this complication. The literature shows different clinical strategies, varying from blind removal in the office to different surgical approaches. There are three papers on this topic with a literature overview of symptoms during or after the procedure, hearing outcome, surgical approach, and complications.5-7 Verdam et al suggest a useful flow chart for the clinical approach. It emphasizes on whether or not to perform CT imaging. 5
In this manuscript, the author’s clinical experience and approach is shared of six patients after iatrogenic damage due to the molding procedure for swimming plugs. The clinical approach of iatrogenic ear mold procedures in the ENT clinic of available literature was analyzed. Based on these data, a clinical algorithm is suggested for patients presenting in the ENT department after iatrogenic damage due to ear molding procedure.
Methods
Descriptive Analysis
A Medline literature search was performed for publications about impression material in the middle ear due to ear mold procedure and all were included for analysis. Parameters such as temporal bone CT, time to removal of foreign body removal/surgery, type of removal, ossicular chain involvement, revision surgery, and outcome were obtained. An adverse outcome was defined as a complicated course after removal of the silicone material of the middle ear, such as hearing loss, perilymph fistula, and persistent tympanic perforation.
Statistical Analysis
Statistical analysis using the Fisher exact test was performed to compare adverse outcomes of the following clinical parameters: blind removal in-office; surgical approach (transcanal versus tympanomastoidectomy); preoperative temporal bone CT present; perioperative ossicular involvement; and need of revision surgery. A P value <.05 was considered significant. Data were analyzed in Microsoft Excel.
The local medical ethical review board approved retrospective analysis of our case series.
Results
Case Series
Six patients were referred during the last 5 years to the Amsterdam academic medical center after traumatic ear mold impression procedure by hearing aid specialists.
All patients were treated with middle ear surgery by three different ear surgeons.
Case 1
A 14-year-old boy was referred 1 day after traumatic ear mold impression of his right ear. Silicone material had entered the middle ear cleft through a longstanding eardrum perforation (conductive hearing loss of 30 dB HL before incident). The patient endured pain and increased hearing loss (conductive hearing loss 45 dB HL). A CT scan confirmed soft tissue density in the middle ear cleft from the tympanic membrane reaching the promontory and the Eustachian tube. The stapes and mesotympanal parts of the malleus and incus seemed to be covered in silicone material. A combined approach tympanoplasty was performed under general anesthesia. After careful manipulation of the (purple) silicone material, the middle ear part could be removed in one part leaving the ossicular chain intact. The tympanic membrane perforation was closed using temporalis fascia. Three months after surgery a persistent inferoposterior perforation with remaining conductive hearing loss of 25 dB was measured. Revision surgery was performed 2 years later to close the tympanic membrane. The tympanic membrane was intact and hearing normalized.
Case 2
An eight-year-old girl was referred for silicone deposition in the middle ear at her right side. Tympanoplasty was aborted in the referring center, because the ossicular chain was covered by orange silicone material. Three months before visiting the ENT specialist, she had a silicone mold made for the right ear because of an eardrum perforation and her wish to swim. The molding of the silicons had been painful but she had not noticed any additional hearing loss, vertigo, or other complaints. Because of encasement of the ossicular chain, she was referred to our clinic. Pure tone audiometry (PTA) showed maximal conductive hearing loss with a Carhart notch (maximal sensorineural threshold of 20 dB at 2000 Hz).
On CT, soft tissue density was seen around the incus, part of the head of malleus, also reaching the oval window niche. The stapes could not be recognized. A combined-approach tympanoplasty was performed. The orange silicone material was removed in small parts until the landmarks could be visualized (Figure 1). The silicone material encased both the incus and stapes and extended to the protympanum. The incus, the capitulum, and the posterior crus of the stapes could not be preserved and were therefore removed. What remained was the fractured stapedial footplate with the anterior crus. No perilymph leakage was seen. No ossicular chain reconstruction was performed directly because of the higher risk of inner ear damage in case of the fractured footplate. The patient was advised to perform a chain reconstruction at a later stage. The tympanic membrane perforation was reconstructed with fascia temporalis. Initially no ossicular chain reconstruction was performed. Her hearing threshold after surgery showed a complete conductive hearing loss, for which she uses a BAHA softband©.
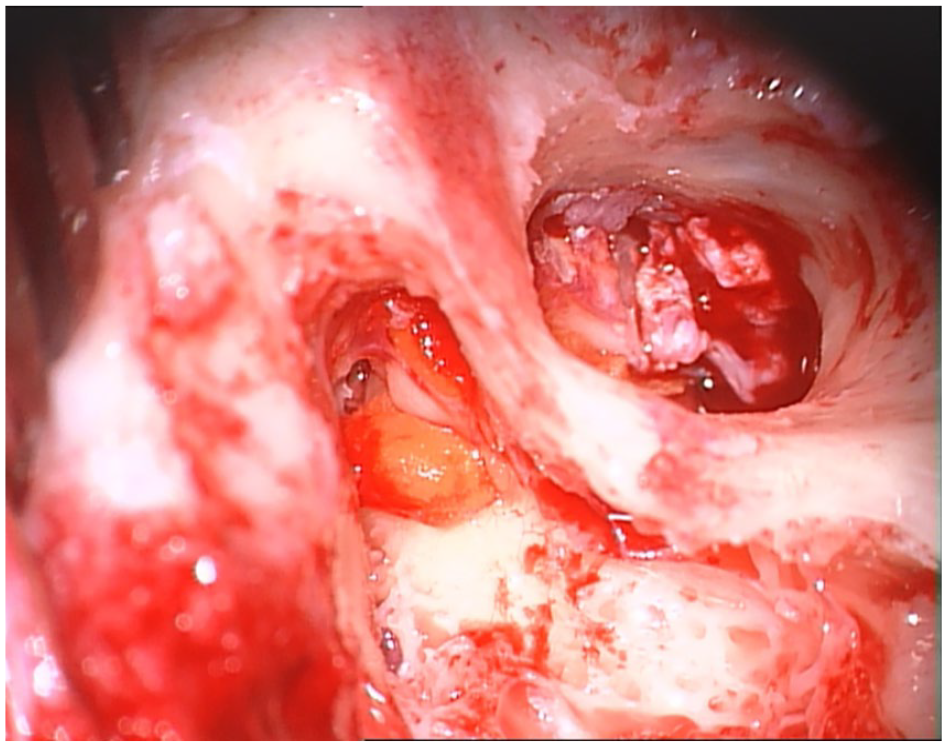
Intraoperative view of canal wall up approach of mold material in the middle ear, epitympanum, and antrum. A wide canal plasty has been performed for improved middle ear exposure. The chain is intact, however covered with material.
Case 3
A 5-year-old boy with a medical history of ventilation tubes because of longstanding otitis media with effusion was referred because of persisting conductive hearing loss of his right ear (30 dB HL) and myringitis granulomatosa. Radiologic imaging revealed opacification of the middle ear cleft. Combined-approach tympanoplasty was performed and blue silicone material and a ventilation tube were found medial and anterior of the ossicular chain reaching towards the Eustachian tube. The granulation tissue on the eardrum masked an anterior perforation. The ossicular chain was covered with granulation tissue. The stapedo-incudal joint was dislocated, the incus eroded. The material was removed, the incus was sacrificed, and a Dresden partial ossicular prosthesis was placed. The tympanic membrane perforation was left open after removal of granulation material because of his recent medical history of longstanding otitis media. Postoperative conductive hearing loss was 15 dB without clinical symptoms. A revision tympanoplasty could be considered in the future if needed. Retrospectively, 3 months prior to hospital presentation the patient had a painful ear mold impression procedure for swimming plugs.
Case 4
A 14-year-old boy presented at the clinic after silicone material had been accidentally introduced into the middle ear during mold impression of the left ear (through an existing tympanic perforation). He presented with otalgia and had maximal conductive hearing loss. CT imaging performed by the referring hospital showed an opacified middle ear cleft with soft tissue around the stapes and incus. Surgery was performed to remove the material.
A limited bony canalplasty was performed to access the hypotympanum. Silicone material was removed in parts from the incus, stapes, sinus tympani, and round window niche using a combination of knife, curette, and KTP laser. The ossicular chain remained intact. Minimal part of the silicone was left behind in the sinus tympani as the surgeon did not successfully remove it. Tympanic membrane reconstruction was performed with fascia temporalis. Postoperatively, the tympanic membrane remained intact and audiometry showed conductive hearing loss of 20 dB HL.
Case 5
Ear mold impressions for swimming (water protection) were made for a 9-year-old girl with ventilation tubes. The procedure was complicated by protrusion of silicone material in and around the ventilation tube of the left ear. The patient was referred to our center for advice. PTA showed 15 dB HL conductive hearing loss. CT imaging showed soft tissue in the mesotympanum and hypotympanum, the ossicular chain was not involved. Tympanoplasty was performed via transmeatal approach; the silicone material and ventilation tube were removed in 1 piece and the perforation was closed with Tutoplast© fascia temporalis. Postoperatively, the hearing normalized and the eardrum remained intact.
Case 6
A 39-year-old woman with pre-existing (congenital) nonserviceable hearing at the left side (along with tympanic membrane perforation and chronic otitis media) was referred to our clinic after iatrogenic ear mold impression for swimming protection. CT showed silicone material in the left external ear and middle ear; the incus was completely surrounded by the molding material. Given the pre-existent deafness and chronic otitis media, a subtotal petrosectomy was performed to treat the aural discharge. The postoperative course was uneventful.
Analyzed Data
Twenty-two publications were included for analysis.4-25 In total, 49 ears, including this study, were evaluated (Table 1). In the majority of the other studies, the ear impression was taken for hearing aids. In our patients, the ear mold material was silicone and was used for customized swimming plugs. In most case reports, the type of impression material was not mentioned.
Treatment Characteristics in Reviewed Cases: Type of Foreign Body Removal Approach, Temporal Bone CT, Type of Surgical Approach, Ossicular Involvement, and Revision Surgery.
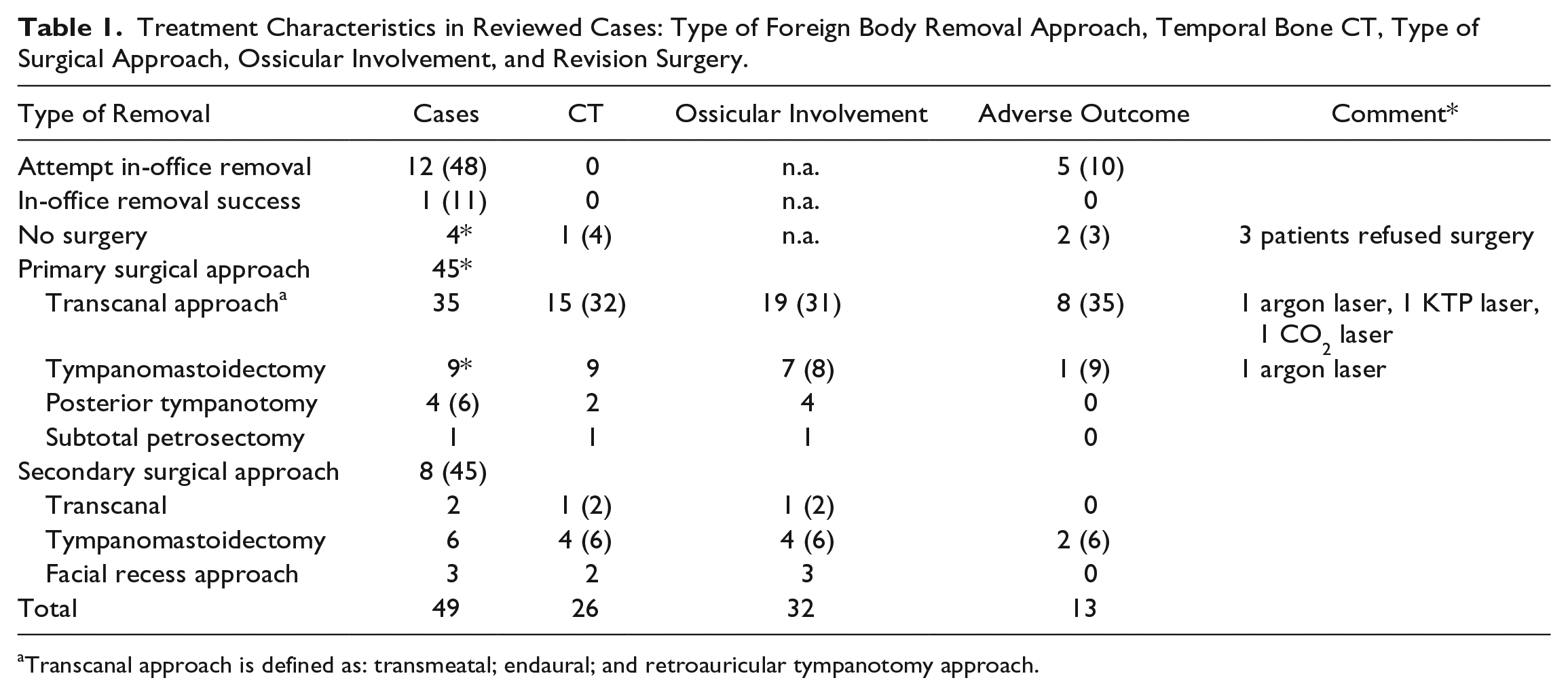
Transcanal approach is defined as: transmeatal; endaural; and retroauricular tympanotomy approach.
Time between removal of the foreign body in the middle ear and iatrogenic ear mold impression was widely spread from 1 day to 7 years. No follow-up period was defined and in most cases the exact follow-up period was not mentioned.
Thirteen patients had an adverse outcome: hearing loss; both conductive and sensorineural; stapes dislocation; perilymph fistula; severe vestibular complaints; or persistent tympanic membrane perforation.
The clinical approach of the 49 cases was evaluated. In-office removal attempts without CT mastoid were described in 12 patients. In only 1 casec was this attempt successful.
Surgical removal was advised in the other 11 patients. Three patients refused surgery. Follow-up was available for 10 out of 12 patients. Two cases ended with an adverse outcome.
Surgery was performed on 45 ears, of which 20% (9 ears) had an adverse outcome. Different approaches were described. Transcanal approach was defined as: transmeatal; endaural; and retroauricular transcanal approach. Transcanal approach was chosen in 35 cases, transmastoidal approach in 9 cases, and subtotal petrosectomy in 1 case. Preoperative CT imaging was performed in 25 of 45 cases (55%). In 19 of 31 transcanal cases and in 7 of 8 transmastoidal cases, there was ossicular involvement of the mold material. Revision surgery was performed in 7 cases after prior transcanal approach and in 1 case after transmastoidal approach.
Statistical Analysis
The Fisher exact test was performed to evaluate the risk of adverse outcome (persistent complications after treatment). In-office blind removal of the material is associated with a significant risk of adverse outcome (P =.03). This also accounts for ossicular involvement (P =.01).
Availability of preoperative temporal bone CT, type of surgical approach, and need for revision surgery were not correlated with an adverse outcome (P = .28, .34, and .15, respectively).
Discussion
Based on these data of 49 cases, blind removal of mold material (without CT imaging) should be avoided, because of the risk of additional damage. CT imaging of the temporal bone gives information about the extension of mold material. The authors do realize that there is probably a degree of publication bias. Also, cases from more than 30 years ago were included; today, better imaging is available and more accessible. Minor spill of mold material without involvement of the tympanic membrane will most probably lead to uneventful removal in outpatient setting. No significant difference in outcome was found between transcanal or transmastoidal approach. Because of the significant risk of complicated outcome in cases with ossicular chain involvement, we believe the best visualization of the chain is transmastoidal approach with the possibility of a facial recess approach. Below, a clinical approach is suggested for patients (Figure 2). The authors do realize that this algorithm is subject to local preferences and the surgeon’s experience.
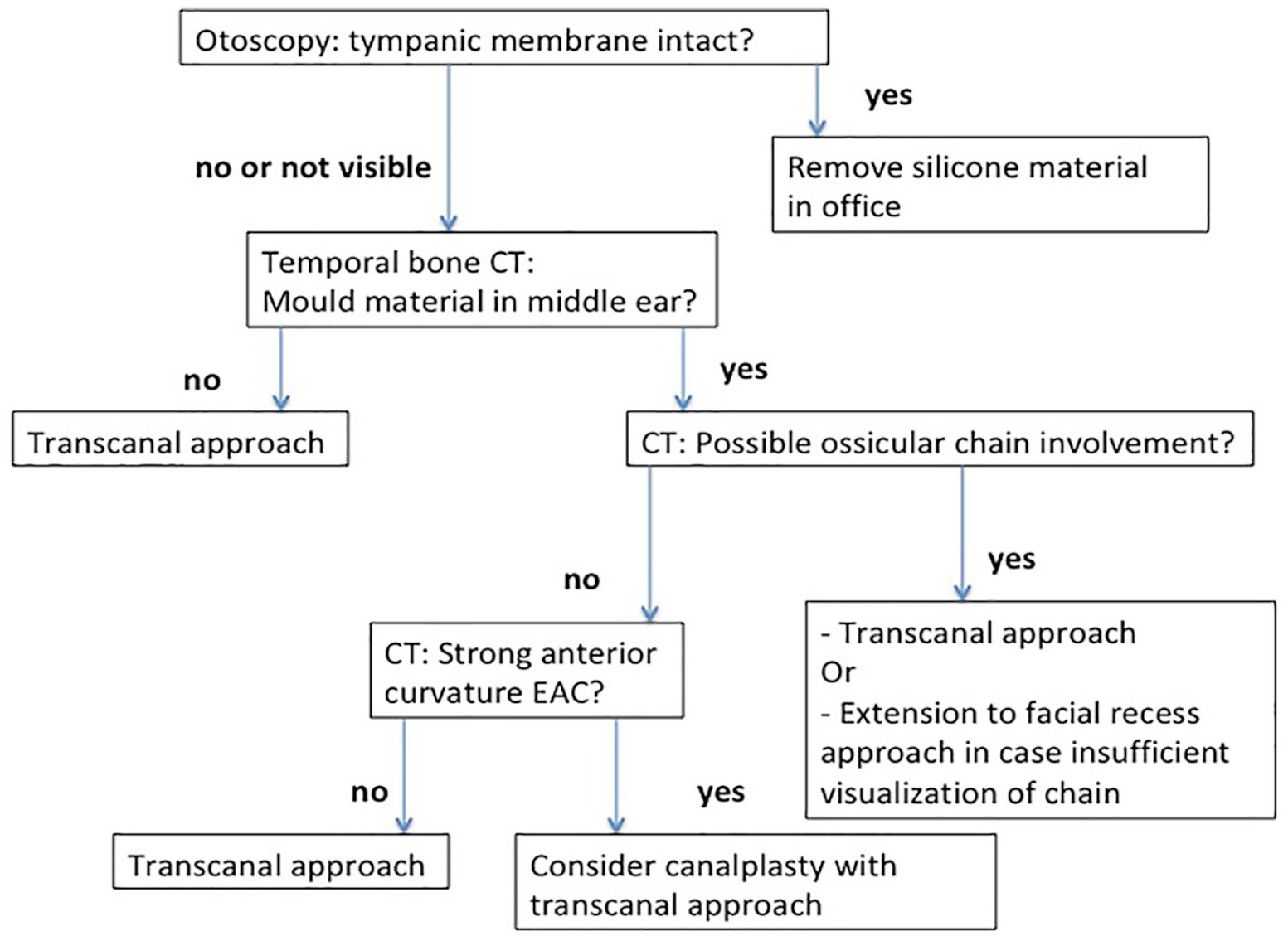
Flowchart of clinical approach of attending outpatient ENT patient with ear mold material left in the ear canal.
Canalplasty can be useful for optimal approach of the hypotympanum and in case, of a prominent anterior external wall. In 3 ears, laser dissection was used; this can be helpful when the material is situated around the ossicular chain. In the author’s opinion, canal wall down mastoidectomy should be avoided if possible. In specific cases, canal wall down mastoidectomy (consider direct canal wall reconstruction) or subtotal petrosectomy could be considered in patients with pre-existing ear problems, for example, chronic inflammation or functional deaf ears. Time of surgery after the iatrogenic mold impression fitting ranged from days to years. Foreign body in the middle ear could have clinical consequences as shown in the cases of Syms and Lee.10,18 In another case report, 8 a 70-year-old woman with impression material in the middle ear started to have complaints of dizziness and purulent otorrhoea 5 years after the impression taking. In Awan et al, silicone material in the middle ear that was unintentionally incompletely removed did not give clinical complaints and showed no tissue reaction or adhesion to surrounding structures over a period of 9 years. 14 In one of the cases in this study, the silicone impression material could incompletely be removed because of its location in a deep sinus tympani. In therapy decision making, it should be taken into consideration that foreign bodies in the middle ear could give long-term reactions.
In the Netherlands, all children achieve a swimming certificate during primary school and have weekly swimming lessons for at least 1 year. Many children with ventilation tubes are advised to use custom-made swimming plugs in order to reduce the amount of episodes of otorrhoea. However, the absolute reduction of episodes of otorrhoea as a result of the use of swimming plugs is low, according to a Cochrane review. 1 Taking into account the risks of ear mold fitting and the possible long-term consequences, the (standard) indication for swimming plugs should be reconsidered, and maybe even discouraged. At this point, the Dutch Otorhinolaryngological Society has a neutral position and states that doctors generally allow swimming with ventilation tubes without any protection; whereas doctors generally advise swimming under water with additional protection.
Conclusion
CT imaging of the temporal bone is advised in patients in the ENT clinic after complicated or painful molding procedure for ear impressions if the tympanic membrane cannot be examined completely or the middle ear is involved. Blind removal should be avoided. Transcanal retroauricular tympanotomy (with canalplasty if needed) or transmastoidal tympanotomy with facial recess approach (if necessary) is best practice if the mold material has entered the middle ear. The use of laser can facilitate dissection off the ossicular chain.
Performing the molding procedure should be an official item in the training of hearing aid specialists. Trained professionals should perform the molding procedure for aural impression taking. In case of unsuccessful or symptomatic mold removal or molding procedure (such as otalgia, vertigo, tinnitus, and hearing loss), an ENT specialist consultation should be considered.
The lack of evidence and the potential benefits, as well as the availability of an alternative for children with ventilation tubes (cotton and Vaseline), should be weighed against the risks of the molding procedure. The national otorhinolaryngological society (societies) should consider taking a firmer position in its general use.
Footnotes
Authors’ Note
Jérôme J. Waterval is also affiliated with Maastricht University Medical Centre, Maastricht, the Netherlands.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.