
Abstract
Introduction
More than 180,000 new cases worldwide were diagnosed with laryngeal cancer in 2020. 1 Previously, laryngeal cancer management was concentrated primarily on tumor control and survival rate but has evolved to incorporate functional and health-related quality of life (HRQoL) outcomes. 2 Within patients who present with laryngeal cancer managed with surgery, radiation therapy (RT), chemotherapy, or a combination of these modalities, diminished HRQoL has been investigated to varied extents. 3 Moreover, fewer studies have focused on its influencing factors. Two major problems, swallowing disorders and dysphonia, have been shown to influence HRQoL negatively. 4 Previous research indicated that patients with laryngeal cancer might need support regarding swallowing and voice rehabilitation. 5 Thus, exploration of related-factors is favorable to optimize the treatment regimens, improve the therapeutic outcomes, and eventually better HRQoL of these patients.
Fatigue and sleep disturbance have been increasingly recognized as health issues that negatively affect HRQoL for patients with other cancers. 6 Existing studies proposed that fatigue and sleep disturbance also persisted among patients with laryngeal cancer after treatment. 7 Up to now, far too little attention has been paid to identifying the association between sleep and HRQoL in laryngeal cancer patients. An often overlooked cause of sleep disorders in this population was obstructive sleep apnea (OSA). Previous studies reported that incidence of OSA afterward therapy was extensive, ranging from 12% to 96%. 8 Additionally, significant risk factors for OSA were defined in recent studies. 9,10 However, the association between tumor size, clinical stage, surgical method, radiotherapy, and OSA is still inconclusive. Furthermore, the severity of OSA and nocturnal hypoxemia was independently associated with all-cancer risk based on biological models. 11 Clinicians should recognize the prevalence, etiology, and correct management of OSA after therapy for laryngeal cancer. 12
HRQoL assessment requires an instrument that is multidimensional, standardized, easily understandable, and workable. The MOS (Medical Outcome Study) 36-item Short-Form Health Survey (SF-36) which has physical and mental scales measuring 9 domains of HRQoL was valid, credible, and compatible in the Chinese population. 13 A variety of specific instruments may assess different aspects of HRQoL in patients with laryngeal cancer, including MD Anderson Dysphagia Inventory, voice-related quality of life, and hospital anxiety and depression scale. 14 The SF-36 was confirmed to have the best validity, reliability, and responsiveness for general health-status measures of patients with OSA. 15
It might be concluded that a convincing evidence for the association between OSA with HRQoL in patients treated for laryngeal cancer was lacking. Hence, the main purpose of this research was to evaluate the impact of OSA on HRQoL of patients with partial laryngectomy. Additionally, the prevalence and possible risk factors for OSA in these patients were investigated.
Methods
Patients
From May 2020 to March 2022, patients with laryngeal squamous cell carcinoma (LSCC) who underwent partial laryngectomy in the Eye, Ear, Nose, and Throat Hospital, Fudan University were recruited postoperatively. This cross-sectional study was approved by the Ethics Committee and the Institution Review Board of the Eye, Ear, Nose, and Throat Hospital, Fudan University, Shanghai, China (Ethical Approval No. 2020014-1). Written informed consent was obtained from each patient. Inclusion criteria were a clear diagnosis of LSCC, no dyspnea during continuous tube plugging for at least a month, planned tracheostomy extubation, no recurrence of the tumor, no medical history of other malignancies, ability to undergo the polygraphy (PG), and adequate knowledge of Chinese.
Demographic and clinical characteristics were, respectively, collected via chart review and self-reported. Body mass index (BMI) was calibrated as patient’s weight in kilograms divided by the square of height in meters. Tobacco use was defined as a current or history of daily tobacco consumption. Alcohol use was defined as a daily intake of more than 80 mL of pure alcohol per day. Smoking index was calculated as the number of cigarettes consumed per day multiplied by years of smoking. Drinking index was calculated as the volume of pure alcohol consumed per day multiplied by years of drinking. The clinical staging was determined using Tumor, Node, Metastasis staging system outlined in the American Joint Committee on Cancer’s AJCC Staging Manual, 8th edition. 16 Tumor area (length multiplied by width) and tumor depth were manually extracted from pathology reports. Surgical treatment included partial laryngectomy with or without neck dissection. Surgical methods included supracricoid partial laryngectomy and vertical partial laryngectomy.
Polygraphy
All participants underwent an overnight PG home sleep test (Embletta MPR PG, Natus Medical Incorporated, Pleasanton, CA, USA) in their own house at night before extubation. The monitor consisted of nasal airflow, oxygen saturation, and electrocardiograph. An experienced sleep laboratory technician scored all the tests based on standard criteria. Individuals with an obstructive apnea–hypopnea index (AHI) ≥5 per hour were classified as OSA group. Severity on OSA was categorized into mild (5 ≤ AHI < 15), moderate (15 ≤ AHI ≤ 30), or severe (AHI > 30).
HRQoL Assessment
SF-36 was applied to assess overall HRQoL at the same time as PG test. 17 This questionnaire contains 36 items that describe 9 dimensions of health: physical function (PF), role physical function (RF), body pain (BP), general health (GH), vitality (VT), social function (SF), role emotion (RE), mental health (MH), and health transition (HT). 18 It presents a final score ranging from 0 to 100, in which 0 corresponds to the worst health condition and 100 corresponds to the best health status.
Statistical Analysis
Data were analyzed using SPSS version 20.0 (IBM Corporation, Chicago, IL, USA) and R software (version 3.6.1; http://www.R-project.org) with the ggplot2, magrittr, checkmate, forestplot, and ggpubr libraries added. The P values <.05 were considered statistically significant. Absolute numbers and percentages were identified for categorial variables. Mean and SD were calculated for continuous variables. Continuous variables were converted to binary variables and categorical variables were ordered according to the median numbers and quartiles, respectively. Categorical variables were compared using chi-squared test or Fisher’s exact tests, depending on the number of observations. Ordinal categorical variables were compared using Mantel–Haenszel chi-squared test. Continuous variables were analyzed using Student’s t test or Mann–Whitney U test, as appropriate for the type of distribution. Principal component analysis (PCA) combines K-means clustering to identify 2 clusters based on sleep-related parameters. The comparisons of HRQoL were visualized using radar charts. Multivariate analysis by ordinal regression model was shown via the forest plot.
Results
A total of 78 patients who underwent partial laryngectomy for laryngeal cancer were eligible for this study, of which 75.6% responded by answering the questionnaire. Finally, 59 patients were included in the analysis, of whom 96% were male and 4% were female, with a mean age of 60.1 ± 8.53 years (range from 33 to 80 years). Fifteen patients received neck dissection, 12 patients received adjuvant radiation, and 2 patients received chemoradiotherapy. Based on PG, 44 patients (74.6%) were diagnosed with OSA (AHI range from 5.2 to 49.8 per hour, median 12.8 per hour), specifically 25 (42.4%) with mild OSA, 11 (18.6%) with moderate OSA, and 8 (13.6%) with severe OSA. The mean time from surgery to PG was 18.6 ± 15.30 weeks, ranging from 4 to 76 weeks. There was no significant difference between the non-OSA group and the OSA group at the time (22.5 ± 18.04 weeks vs 17.3±14.25 weeks, P = .260). Baseline characteristics of the cohort were summarized in Table 1.
Demographic and Clinical Characteristics of the 59 Patients.
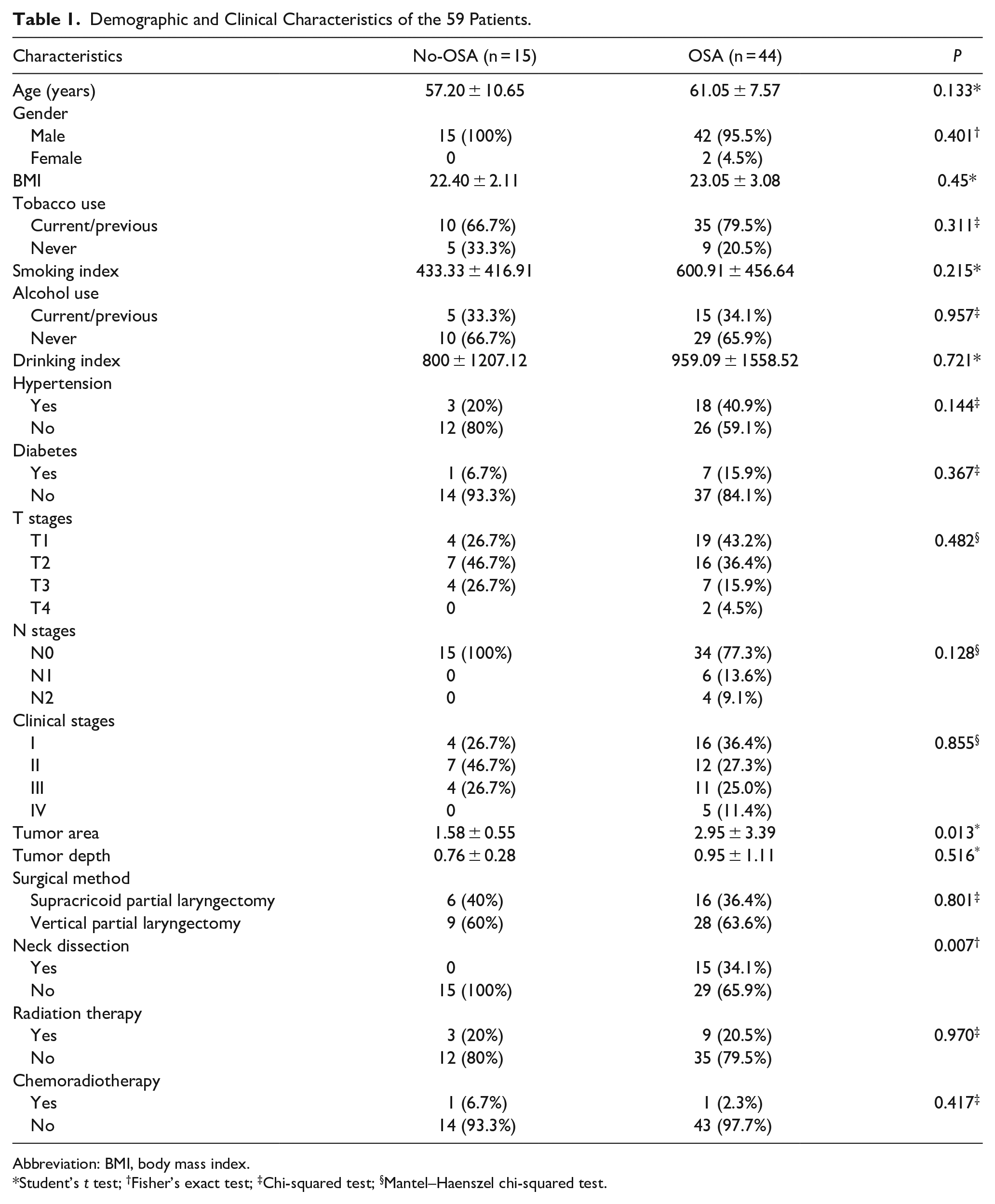
Abbreviation: BMI, body mass index.
Student’s t test; †Fisher’s exact test; ‡Chi-squared test; §Mantel–Haenszel chi-squared test.
The tumor area in OSA group was significantly larger than that in non-OSA group (2.95 ± 3.39 cm vs 1.58±0.55 cm, P = .013). In the OSA group, there were significantly more patients who underwent neck dissection than those in the non-OSA group (34.1% vs 0%, P = .007). However, both groups were similar in the distribution of age, gender, BMI, tobacco use, alcohol use, clinical stage, tumor depth, surgical method, history of hypertension, diabetes, radiation, and chemoradiotherapy.
A radar chart presents an overview of the all SF-36 domains between non-OSA group and the OSA subgroups (Figure 1a). Patients with partial laryngectomy had lower scores of RF, GH, RE, and HT than the scores of PF, BP, VT, SF, and MH. Severe-OSA subgroup had the lowest scores in majority of domains compared with that of other 3 subgroups.
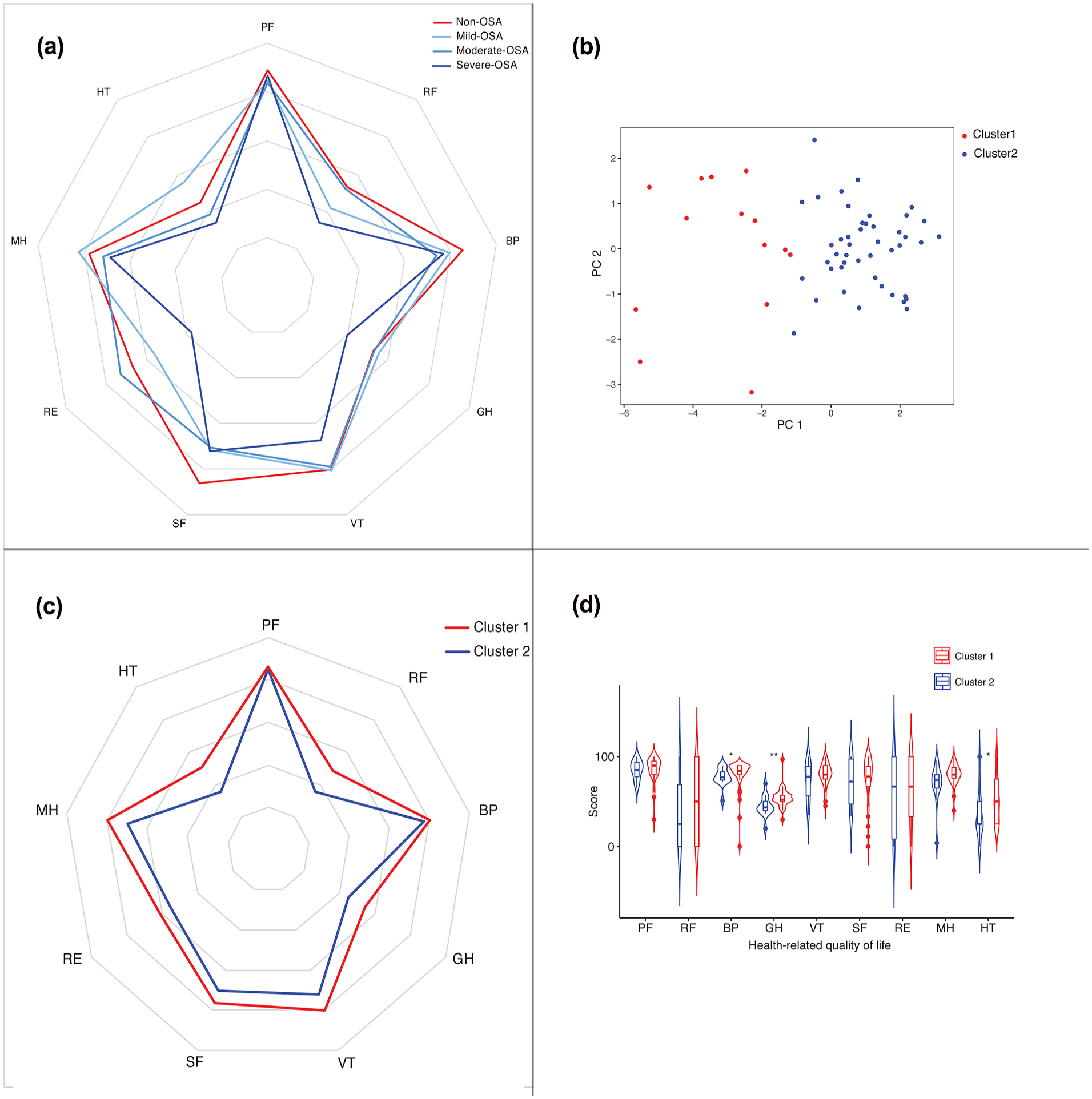
Health-related quality of life assessment in patients who underwent partial laryngectomy for laryngeal cancer. (a). Comparisons of SF-36 scores between non-OSA group and the OSA subgroups. (b) Principal component analysis-based K-means clustering. Different colors indicate the 2 clusters found for the principal components (PC1 and PC2). PC1, labeled “respiratory events,” had the greatest loadings on OD and AHI; PC2, labeled “oxygen saturation,” had the greatest loading on mean SpO2. (c) Comparisons of SF-36 scores between cluster 1 and cluster 2. (d) Violin plot showing the distribution and level of SF-36 scores in 2 clusters. The top and bottom of the embedded box signify the 75th and 25th percentile of the distribution, respectively. The line inside the box represents the median.
To study the impact of OSA on the quality of life after partial laryngectomy, patients were clustered based on sleep-related parameters as shown in Table 2. Dimensionality reduction of sleep-related parameters were performed using PCA (Supplemental Material). Combined with K-means clustering, cluster 1 and cluster 2 were identified (Figure 1b). The first component, labeled “respiratory events,” had the greatest loadings on oxygen desaturation (OD) index and AHI; the second component, labeled “oxygen saturation,” had the greatest loading on mean pulse oximeter oxygen saturation (SpO2). Correspondingly, each mean score of cluster 1 was higher than that of cluster 2 in the 9 dimensions (Figure 1c). Further statistical analysis was shown as a violin plot (Figure 1d). It revealed that 9 domains exhibited different distribution and significantly different levels of BP, GH, and HT between 2 clusters. Although it showed the phenotype of worse condition in PF, RF, VT, SF, RE, and MH of cluster 2, no statistically significant differences in these levels were observed.
Sleep-Related Parameters of the 59 Patients.
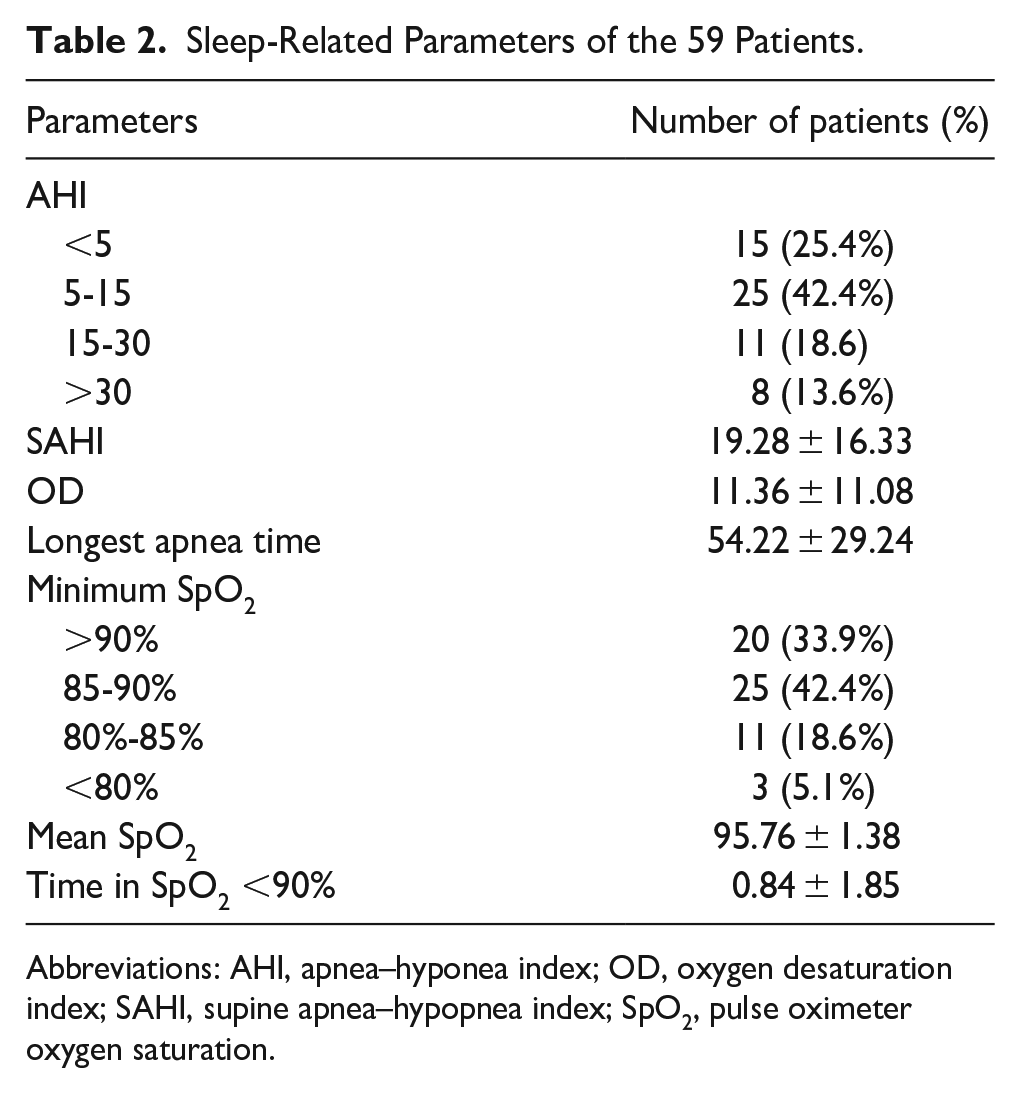
Abbreviations: AHI, apnea–hyponea index; OD, oxygen desaturation index; SAHI, supine apnea–hypopnea index; SpO2, pulse oximeter oxygen saturation.
Other factors, tobacco use, alcohol use, tumor area, and neck dissection, were screened to be also significantly associated with specific health domains (BP, GH, and HT) by univariate analysis. Multivariate analysis by ordinal regression model was shown in the forest plot (Figure 2). No factor was significantly associated with BP in the multivariate model (Figure 2a). Further independent factors associated with GH were tobacco use (OR = 4.716, 95% CI: 0.207-2.894), alcohol use (OR = 3.193, 95% CI: 0.042-2.28), and OSA (OR = 11.336, 95% CI: 0.994-3.862) (Figure 2b). Tobacco use was the only significant factor that influenced HT independently with an HR (Harzard Ratio) of 4.702 and 95% CI of 0.192 to 2.903 (Figure 2c).
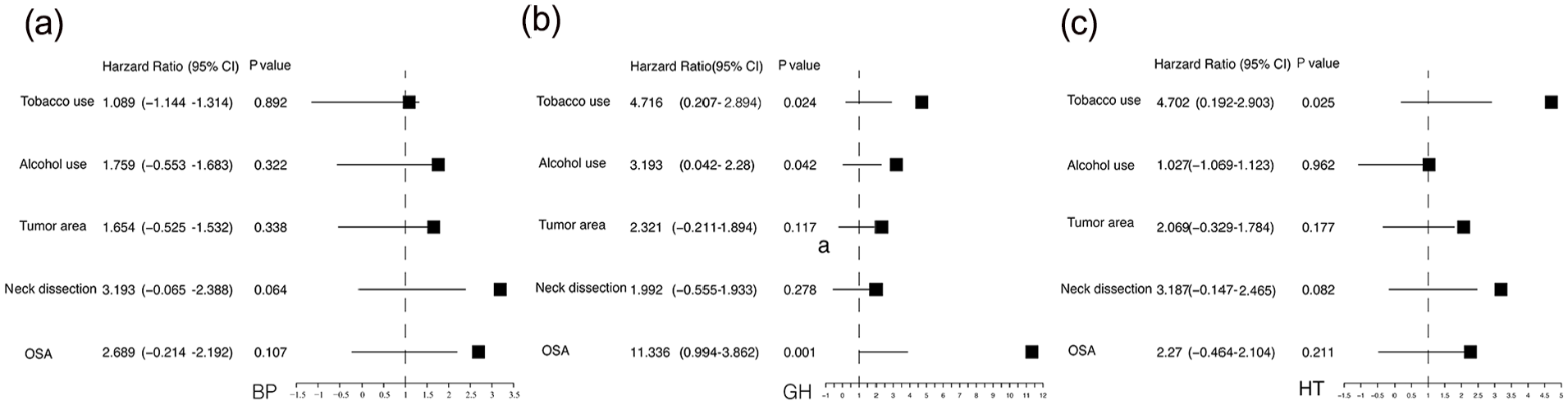
Forest plot of multivariate analysis for factors associated with specific health domains. (a) Analysis for factors associated with body pain (BP). (b) Analysis for factors associated with general health (GH). (c) Analysis for factors associated with health transition (HT). Obstructive sleep apnea (OSA)-related condition based on principal component analysis combined with K-means clustering.
Discussion
Treatment of laryngeal cancers modifies the upper airway anatomy and thereby increases the risk of OSA. 8 In this study, there was a positive screening for OSA in 74.6% of laryngeal cancer patients who underwent partial laryngectomy, which was significantly higher than the reported prevalence of OSA in the general population (15%). 19 Similar findings have also been demonstrated by others. 9,20 However, the incidence of OSA in our study was lower than that of those studies (82.5% and 92.3%, respectively). This discrepancy was most likely due to treatment bias as clinical stages and treatment modalities were diverse. All patients in our study received partial laryngectomy, 25% of them received neck dissection or adjuvant radiation or chemoradiotherapy. This proportion might be higher in the previous studies, while were not elucidated. Another possible explanation for this was the different screening tools used for OSA. Nevertheless, these studieses highlighted that treatment increases risk of developing OSA.
We compared clinical characteristics of posttreatment patients grouped by OSA status and found evidence of significant associations, which were mentioned in only a minority of studies. Firstly, a larger tumor area might be an important predictor for developing OSA; this observation was consistent with findings from others. 21 The larger tumor area indicated greater structural alterations of upper airway, which were regarded as the basis of OSA. Additionally, neck dissection was established based on the site of the primary tumor, clinical stage, and patient’s systemic condition. Specifically, when the epilarynx was involved or the patient was under 65 years old, elective neck dissection was performed on patients with N0 supraglottic tumor in this study. 22 We have highlighted for the first time that neck dissection was a significant risk factor for OSA. The mechanisms involved remain unknown and require further investigation. We speculated that damage to muscles and nerves and decrease of inspiratory strength might be responsible for the OSA after neck dissection. 23 Relatively more research focused on the impact of RT on OSA provided inconsistent conclusions. Chronic edema after RT would favor OSA, as reported in some literature. 24 Our findings pointed to no significant association between RT and OSA risk in laryngeal cancers, which in line with a recent systematic review. 25 Irradiation would hypothetically stiffen the soft tissues and subsequently would not favor OSA. Negative findings also appeared in other clinical characteristics (Table 1). Above all, screening of OSA is highly recommended in laryngeal cancer patients after treatment, especially for those with larger tumor area and neck dissection.
The current study revealed that OSA might contribute to impair HRQoL among laryngeal cancer patients after treatment. Worse status in severe-OSA group was observed in majority of the measured domains. Despite recent awareness of the association between OSA and decreased quality of life in laryngeal cancer patients, for the first time, we have provided evidence for this via using the validated questionnaire SF-36. To obtain a complete understanding of the effects of OSA on HRQoL, it is essential to involve more PG-related parameters in analysis not limited to AHI. In this study, 2 clusters next redefined using PCA followed by K-means clustering have different characteristics. In general, cluster 2 had lower mean score of each dimension than cluster 1 in variable degrees (Figure 1c). Particularly, OSA-related condition significantly correlated to the BP, GH, and HT domains of SF-36, suggesting that patients with OSA indicated a higher likelihood of exhibiting physical limitations (Figure 1d). This raises the question whether or not OSA influences patient’s health in these 3 domains independently. Since we found an odd ratio of 11 between the 2 clusters in GH, postoperative GH impairments were most likely correlated with OSA in patients with laryngeal cancer. A possible explanation for these might be that OSA in patients with partial laryngectomy involves intermittent hypoxia. As is well known, hypoxia diminished physiological functions and the overall quality of life. Previous studies have shown that continuous positive airway pressure (CPAP) may help to improve HRQoL, especially physical performance. 26,27 However, CPAP therapy for patients with partial laryngectomy was not adequate. Recently, a case report indicated that subjective symptoms of sleepiness would be improved when severe OSA was controlled by CPAP after concurrent chemoradiotherapy for laryngeal cancer. 28 A further study with more focus on impacts of CPAP treatment on the HRQoL in patients with partial laryngectomy is therefore suggested. This concerns whether CPAP is recommended for patients with OSA after treatment for laryngeal cancer.
Our interpretation of correlations between different clinical characteristics and these 3 domains was presented on the forest plot based on a multivariate analysis (Figure 2). The findings confirm previous reports in general population of poor HRQoL in smokers and drinkers. 29 The effect of smoking and drinking, the well-known risk factors of laryngeal cancer, on quality of life in postoperative patients was not fully understood. In the postoperative GH score evaluation, there was a statistically significant difference in favor of PF limitations due to tobacco and alcohol use (Figure 2b). Additionally, tobacco use was the only risk factor independently related to HT (Figure 2c). Numerous investigations have already proposed that smoking and drinking were risk factors affecting the recurrence and mortality of patients with laryngeal cancer. 30 According to our data, their role in quality of life impairments should be underlined. All patients with known laryngeal cancer would be strongly encouraged to quit smoking and drinking.
Another concern is the lack of criteria for tracheostomy extubation in patients with partial laryngectomy to data. All patients in this study met the inclusion criterion that no dyspnea during continuous tube plugging for at least a month; however, 74.6% of these were diagnosed with OSA based on overnight PG tests. These findings suggested that some patients who planned tracheostomy extubation still had nocturnal hypoxemia. Additionally, considering the negative impact of OSA on quality of life in patients with partial laryngectomy for laryngeal cancer, further study was recommended to investigate whether PG would be a useful tool in the decision-making about tracheostomy extubation.
Several limitations should be considered. PG was not performed before surgery, and the OSA status at the baseline was not evaluated. It should be pointed out that HRQoL assessment is inherently subjective, although SF-36 was proven to be valid and reliable in the Chinese population. Further work is required to evaluate the HRQoL of patients after treatment for OSA (CPAP therapy) so that the impact of OSA on HRQoL would be further confirmed. Besides, laryngopharyngeal reflux (LPR) may contribute to significant impact on OSA. LPR has not been performed on patients who underwent partial laryngectomy. To gain a better understanding, it might be possible to carry out preoperative and postoperative 24-hour pharyngeal pH probe monitoring on this population.
Conclusions
Larger tumor area and neck dissection might be associated with an increased risk for developing OSA in patients with partial laryngectomy for laryngeal cancer. OSA partially mediated the effect on physical health, including BP, GH, and HT. It is important to be aware of the potential impact of OSA on diminished HRQoL of these patients.
Supplemental Material
sj-docx-1-ear-10.1177_01455613231178955 – Supplemental material for Impact of Obstructive Sleep Apnea on Health-Related Quality of Life in Patients With Partial Laryngectomy for Laryngeal Cancer
Supplemental material, sj-docx-1-ear-10.1177_01455613231178955 for Impact of Obstructive Sleep Apnea on Health-Related Quality of Life in Patients With Partial Laryngectomy for Laryngeal Cancer by Min Chen, Fang Shi, Haitao Wu, Lei Cheng, Peijie He, Qian Jin and Jingjing Huang in Ear, Nose & Throat Journal
Footnotes
Data Availability
The data which support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Science and Technology Commission of Shanghai Municipality of China [Grant numbers 20Y11901900, 21Y11912000]; the Health and Family Planning Commission of Shanghai Municipality of China [Grant number 2019SY059]; and the Shanghai Municipal Key Clinical Specialty [Grant number shslczdzk00801].
Ethical Approval
Approval was granted by the ethics committee of the Eye, Ear, Nose, and Throat Hospital, Fudan University, Shanghai, China (No. 2020014-1).
Statement of Informed Consent
Informed consent was obtained from all individual participants included in the study.
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the ethics committee of the Eye, Ear, Nose, and Throat Hospital, Fudan University.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.