
Abstract
Endoscope provide the excellent view and observe the entire perforation edges, endoscopic cartilage myringoplasty doesn’t require the lateral circumferential incision and the elevation of tympanomeatal skin flap in most cases. The cartilage graft may be pushed through the perforation and place medial to the remnant tympanic membrane and annulus.
I read with great interest the article entitled: “Simultaneous Bilateral Same-Day Endoscopic Myringoplasty Using Tragal Cartilage From One Ear.” by Deniz et al. 1 The authors described bilateral same-day endoscopic myringoplasty using tragal cartilage from one ear in patients with bilateral tympanic membrane perforation with chronic otitis media, bilateral same-day endoscopic myringoplasty using tragal cartilage from one ear seems to be a safe and satisfactory procedure with a good satisfactory success rate. 1 The technique at least provided the following advantage. Firstly, it doesn’t require the harvesting of tragal cartilage in the bilateral ears, thereby shorten the operation time for bilateral same-day surgery. Secondly, it retained tragal cartilage on one ear to use for failure ear in future. However, I just want to declare some points that limit the power of this study.
The authors described “a lateral circumferential incision was performed 4 to 6 mm laterally from the tympanic annulus. This incision was integrated with radial incisions at the 6-o’clock and 12-o’clock positions. The middle ear cavity was visualized after the tympanomeatal skin flap was elevated. The graft was placed using the underlay technique. The tympanomeatal flap was then repositioned” in methods section. 1 I found the central perforation was in 89.3% (75/84) ears. In our department, the lateral circumferential incision and the elevation of tympanomeatal skin flap were not necessary for endoscopic cartilage myringoplasty (Figure 1), and the cartilage graft provide the excellent fashion because of the elasticity and stiffness without the property of constriction. 2 -5 The cartilage graft was pushed through the perforation and placed medial to the remnant tympanic membrane and annulus in our department (Figure 1). Recent some authors also published endoscopic myringoplasty without the elevation of tympanomeatal skin flap and obtained the graft success rate of 85% to 92.9%. 6 -8
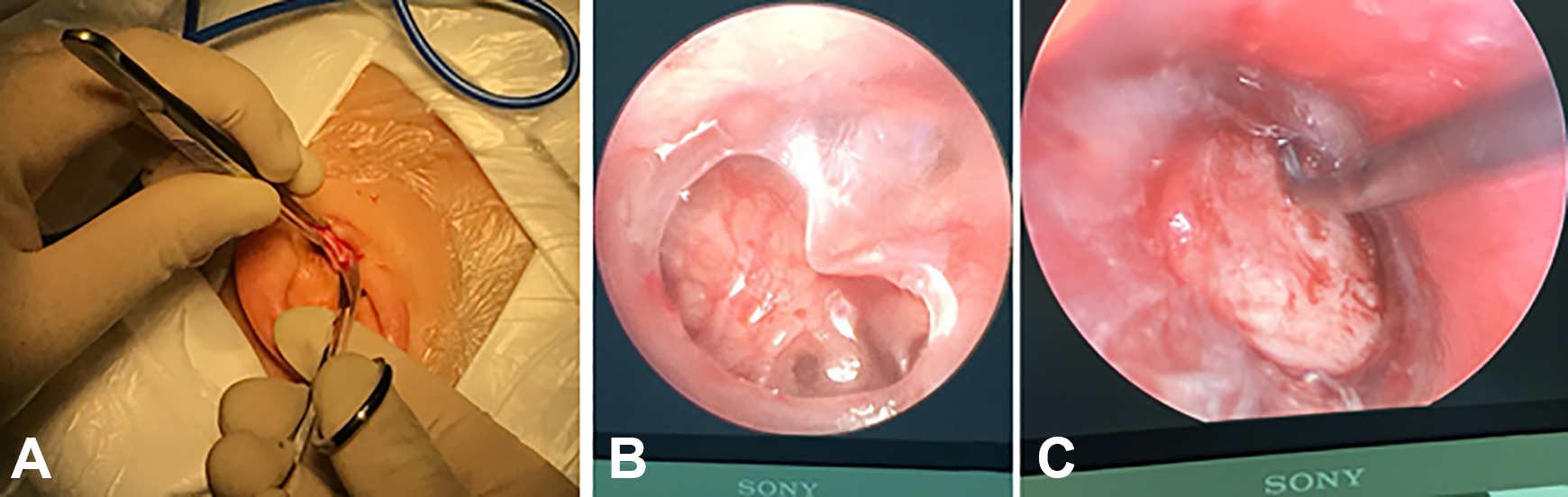
The tragal cartilage was harvested with perichondrium on one side (A). Preoperative middle tympanic membrane perforation (B). The cartilage graft was placed medial to the remnant tympanic membrane and annulus (C).
The elevation of tympanomeatal skin flap not only prolonged the operation time but also increased the possibility of postoperative complications. In addition, the authors described an absorbable material was used to suture the tragus incision. 1 In our department, the tragus incision wasn’t sutured but the packing of the external auditory canal reached the incision using Nasopore and gauze with antibiotic ointment after surgery. The packing gauze was removed from the external auditory canal (EAC) 14 days after the surgery, the tragal incision had healed (Figure 2).
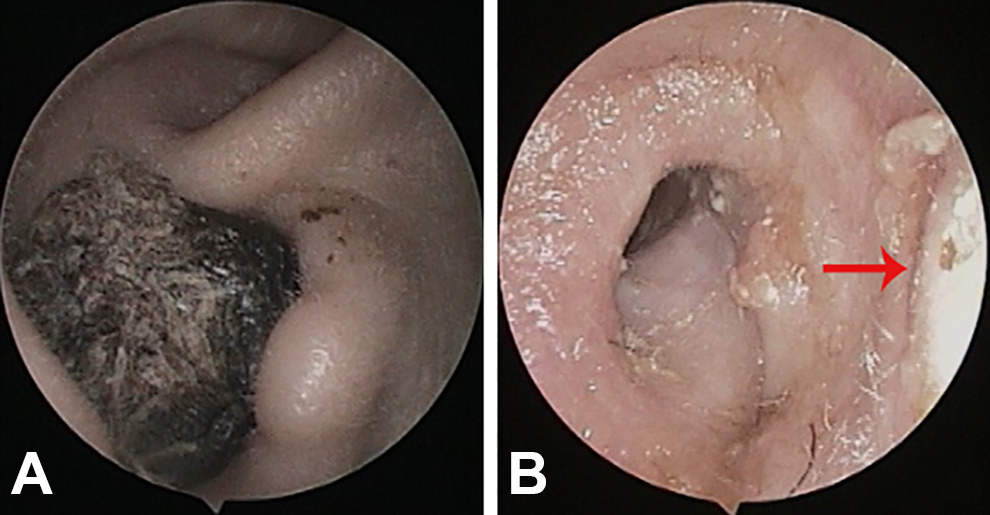
The external auditory canal was packed with Nasopore and gauze with antibiotic ointment after surgery until the tragus incision was reached (A). The packing gauze was removed from the EAC 14 days after the surgery, the tragal incision had healed (B). Red arrows indicated the tragal incision, red triangle indicated the packing gauze.