
Abstract
Both nasal alar and scalp metastases from lung carcinoma are exceedingly rare. Herein, we report a case of an elderly male smoker who had left lung carcinoma and underwent radical resection. Seven months later, masses began to appear on his nasal alar and parietal scalp which gradually increased in size. The nasal computed tomography and head magnetic resonance imaging scan revealed a dense soft tissue shadow in the right nasal alar and nasal cavity, as well as a soft tissue nodule in the middle of the parietal scalp. A biopsy was performed and immunohistochemistry suggested poorly differentiated metastatic carcinoma that was consistent with the characteristics of primary lung carcinoma and supported the diagnosis of nasal alar and scalp metastases. Then, he received a combined treatment of Albumin paclitaxel and Xindirizumab. However, he passed away 3 months later. In addition to this case, we also review the clinical features of nose and/or scalp metastases from lung carcinoma based on previously reported cases as well as this case.
Introduction
Nasal alar and scalp metastases from lung carcinoma are exceedingly rare, with 1% to 12% of lung carcinoma patients developing cutaneous metastases. 1 Cutaneous metastasis from lung carcinoma do not have any specific presentation. 2 In 2000, Rubinstein et al 3 reported a rare case of a tumor on the nose from a large cell undifferentiated lung carcinoma.
In this study, we report a case of a 55-year-old male smoker who presented with masses on the right nasal alar and parietal scalp. These masses were found to have metastasized from left lung carcinoma. We focus on the significance of identifying the tumor and metastasis using computed tomography (CT) and magnetic resonance imaging (MRI), pathology and prognosis after treatment.
Case Presentation
A 55-year-old male smoker was admitted to the respiratory medicine department and was diagnosed with left lung carcinoma a year ago. The carcinoma was a poorly differentiated adenocarcinoma (stageT2N0M0). Immunohistochemistry results showed the presence of CK (pan) and Ki-67; but the absence of NapsinA and TTF-1, CK5/6, and P40.
Six months later, he underwent radical resection of lung carcinoma. Postoperative pathology showed no lymph node metastasis. However, 7 months after surgery, the patient noticed masses on the right nasal alar and parietal scalp but did not pay much attention to them. Three months later, the masses progressively enlarged, and the patient experience right nasal congestion. The right nasal alar mass was dark purple and had a local rupture, causing pain when pressed. The parietal scalp mass was motionless, skin colored, without hair, and did not cause pain when pressed (Figure 1). The patient underwent a nasal CT scan showing a dense soft tissue shadow of 5.8 × 5.8 × 5.9 cm in the right nasal alar and nasal cavity. A head MRI scan also revealed a soft tissue nodule of 1.5 × 1.2 × 1.0 cm in the middle of the parietal scalp (Figure 2). Biopsy of both masses was performed for pathological examination, and immunohistochemistry showed the presence of CK(pan), Ki-67, CK7, CD56, and P40, but the absence of NapsinA, indicating poorly differentiated metastatic carcinoma (Figure 3). Blood test showed elevated carcinoembryonic antigen, carbohydrate antigen 125, and squamous cell carcinoma antigen (9.10 ng/ml, 10.75 U/ml, and 1.72 U/ml, respectively). These results were consistent with the characteristics of primary lung carcinoma, suggesting that both nasal alar and scalp metastases from primary lung carcinoma. The patient received 2 cycles of Albumin paclitaxel and Xindirizumab. However, his condition worsened and he died 3 months later.

Mass in the right nasal alar and parietal scalp (A and B).
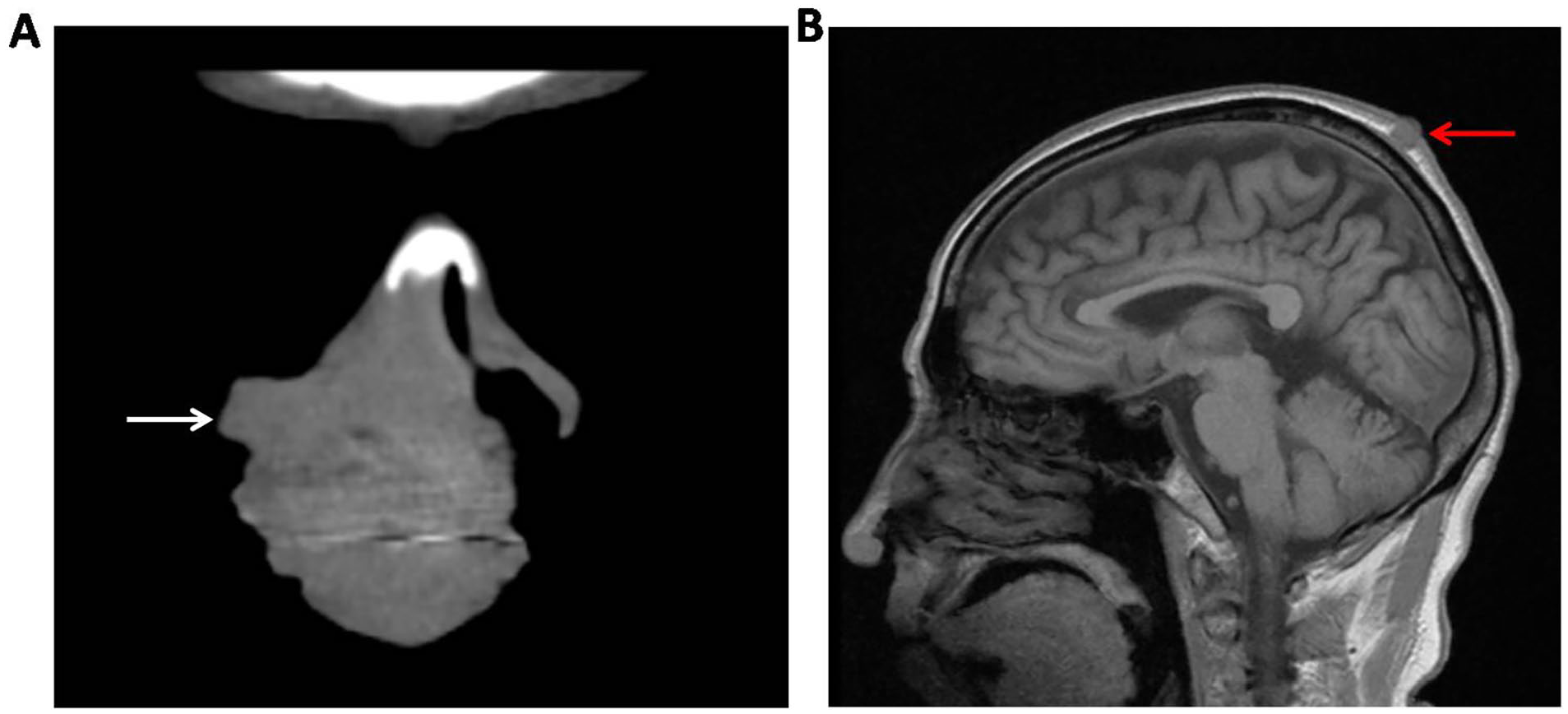
The nasal computed tomography scan showed a dense soft tissue shadow in the right nasal alar and nasal cavity (A, the white arrow). The head magnetic resonance imaging scan showed a soft tissue nodule in the middle of the parietal scalp (B, the red arrow).
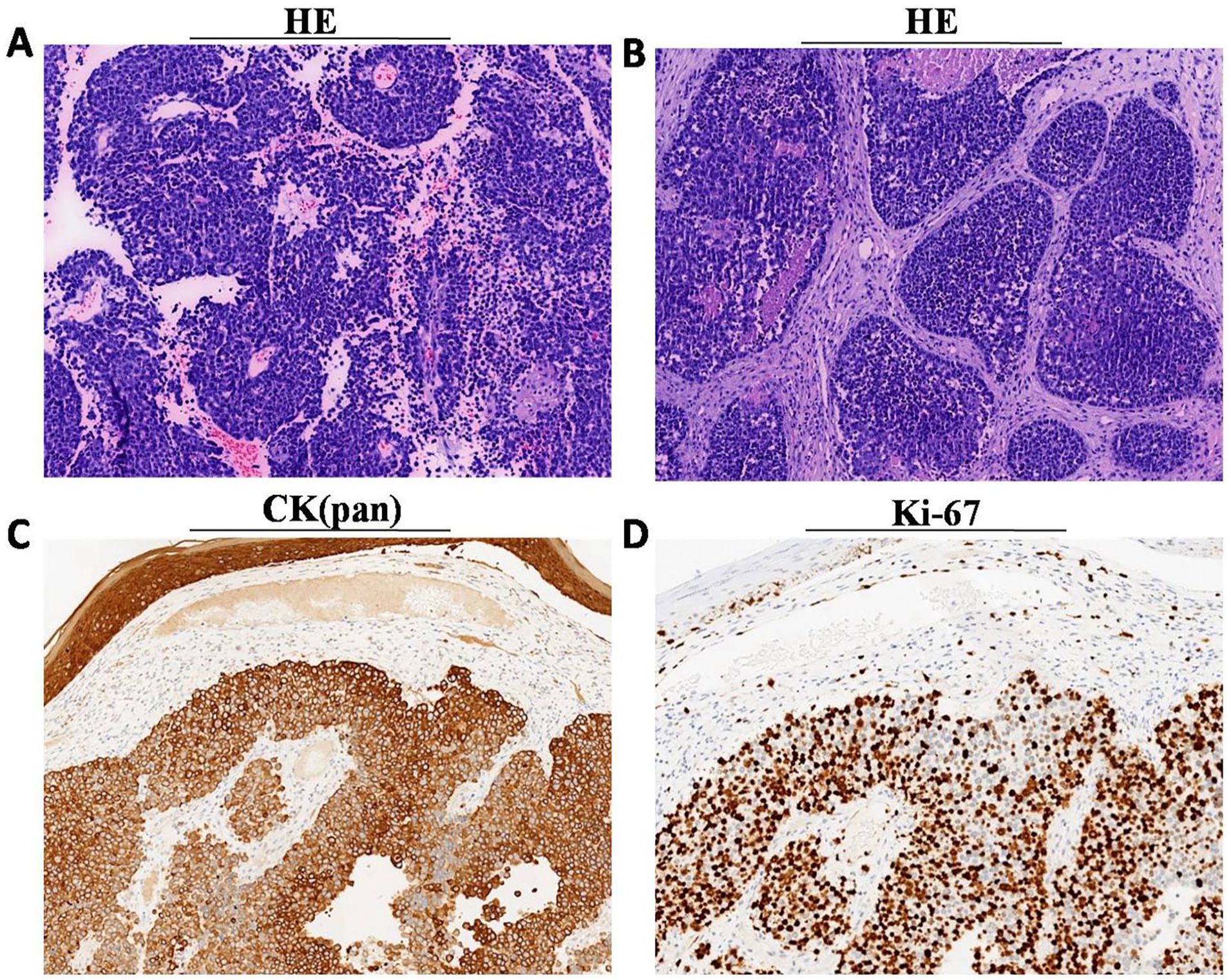
Hematoxylin-eosin staining showed a poorly differentiated carcinoma of the nasal alar and scalp mass (A and B, 100×). The immunohistochemistry showed the following results: CK(pan) (+); Ki-67(+) (C and D, 100×).
Discussion
The most common primary tumor to metastasize to the scalp is lung carcinoma, followed by hematopoietic malignancies and melanoma. 2 Among scalp lesions, metastasis from lung carcinoma is responsible for the third most common malignancy, followed by primary basal cell carcinoma and squamous cell carcinoma. 4 Skin metastasis from the lung carcinoma is often moderately or poorly differentiated.5,6 All histological types of lung carcinoma may metastasize to the skin, and clinical lesions are variable. The most common type is adenocarcinoma, followed by squamous cell carcinoma, small cell carcinoma, and large cell carcinoma.7 -9 In this case,the histological type is the poorly differentiated adenocarcinoma.
Cutaneous metastasis from lung carcinoma is an extremely rare phenomenon and is universally accepted as a sign of progression or widespread metastatic disease. 7 We described a rare case of both nasal alar and scalp metastases from lung carcinoma. Seven months after radical resection of left lung carcinoma, masses of nasal alar and parietal scalp appeared, but no much attention was paid. Three months later, the masses progressively increased with right nasal congestion and the patient was presented to our department for further diagnosis. Then,the nasal CT scan and head MRI scan showed a dense soft tissue shadow in the right nasal alar and nasal cavity,and a soft tissue nodule in the middle of the parietal scalp.The immunohistochemistry of both masses showed the following results: CK (pan): +; Ki-67: +, consistent with those of primary lung carcinoma. These results further suggested that both nasal alar and scalp metastases are from primary lung carcinoma.
This case showed an extremely rare metastasis of lung carcinoma. The primary lung carcinoma was located on the left side, but we observed masses in both the right nasal alar and middleparietal scalp. In this case, tumor markers in the blood, carcinoembryonic antigen, carbohydrate antigen 125, and squamous cell carcinoma antigen were high. We think that the metastasis might move through the lymphatic and blood systems. Related mechanisms need to be further studied.
We reviewed the literature on nose or scalp metastasis from primary lung carcinoma. The nose or scalp was the only or most important site of metastasis from primary lung carcinoma, with or without an identifiable lung carcinoma symptom. This was the case of the almost elderly male smoker. The most common original type was an undifferentiated type followed by a moderately differentiated type. The most common originaltreatment is chemoradiotherapy, because the patients were at the advanced stage at the time of presentation. Time of metastasis is almost less than half a year and the sites of metastatic tumors were diverse. The patients received palliative treatment of chemoradiotherapy, radiotherapy, or chemotherapy. They had worse prognosis and mostly died within 6 months after diagnosis of metastasis (Tables 1 and 2).
Literature Review of the Reported Cases of Metastatic Lung Carcinoma in the Nose.
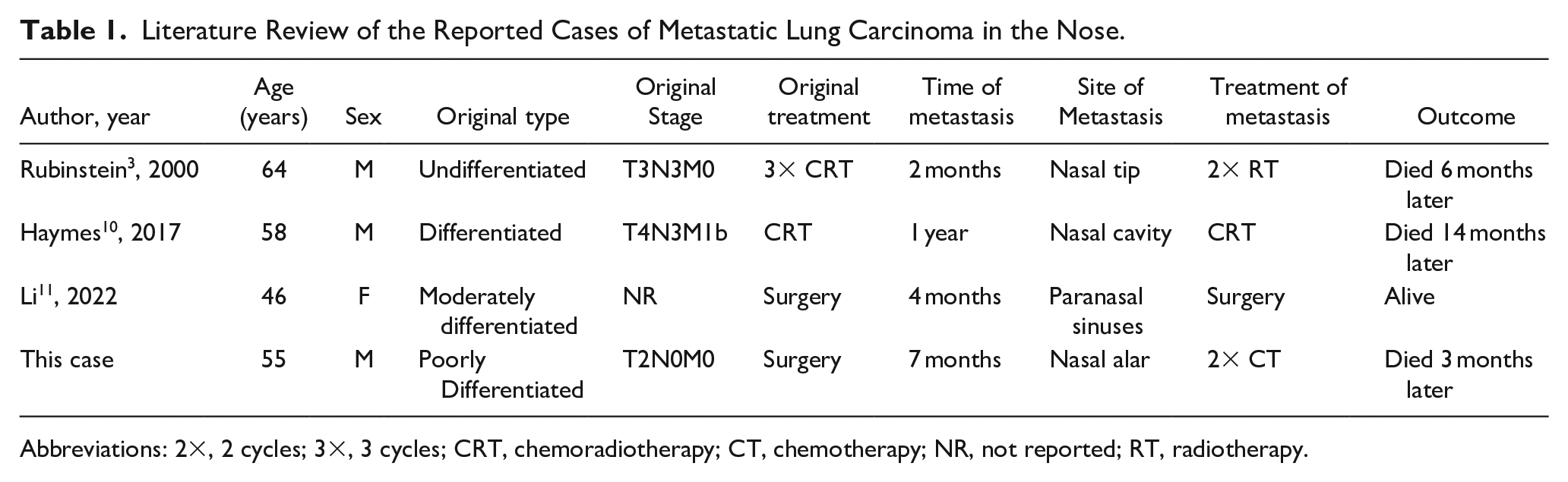
Abbreviations: 2×, 2 cycles; 3×, 3 cycles; CRT, chemoradiotherapy; CT, chemotherapy; NR, not reported; RT, radiotherapy.
Literatu Rereview of the Reported Cases of Metastatic Lung Carcinoma in the Scalp.
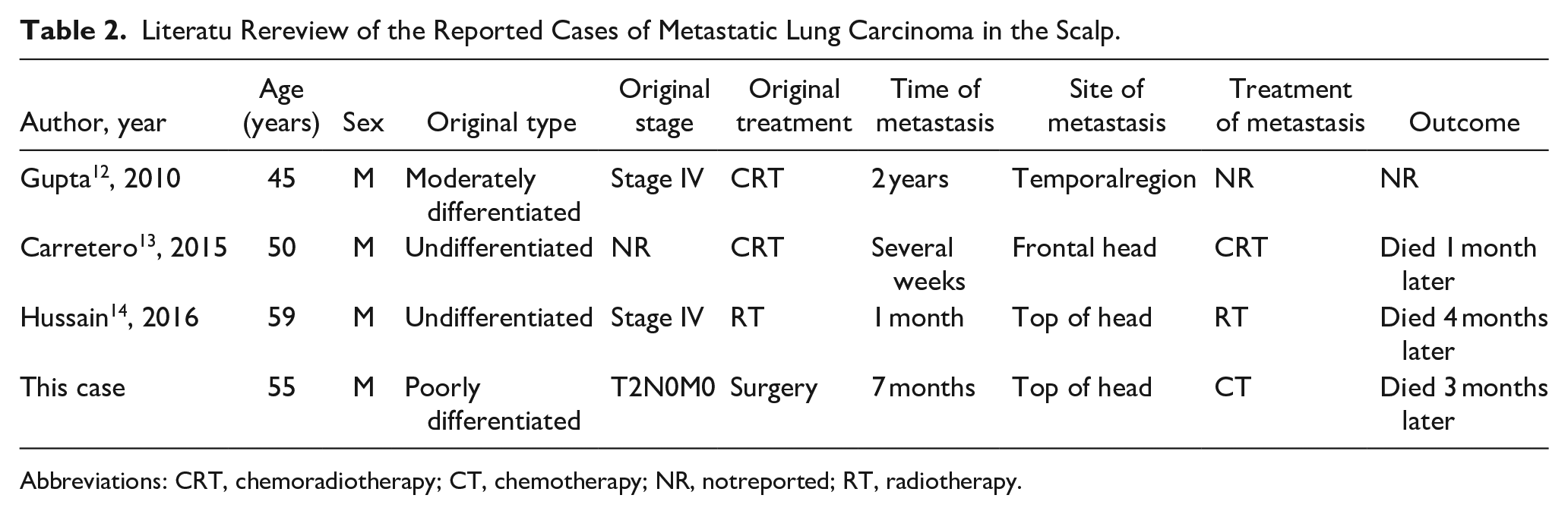
Abbreviations: CRT, chemoradiotherapy; CT, chemotherapy; NR, notreported; RT, radiotherapy.
When nasal alar and scalp masses that are hard to touch is clinically encountered, a detailed inquiry about the disease history, specifically the carcinoma history, is important for the diagnosis and treatment. When nasal alar and scalp metastases from malignant tumor is suspected, CT, MRI, and pathological examination can be used to clarify the primary tumor. The pathological examination is always the gold standard for diagnosing metastasis from the primary tumor. After nasal alar and scalp metastases from primary lung carcinoma is confirmed, the patient should be referred to the department of oncology for further treatment.
Conclusion
Both nasal alar and scalp metastases from lung carcinoma is extremely rare. For patients with a healthy appearance and those with a history of malignant tumors, much attention should be paid to the cutaneous masses. Early diagnosis and treatment are helpful to the clinical outcome. Both nasal alar and scalp metastases from lung carcinoma indicate a poor prognosis.
Footnotes
Authors’ Note
Lu Zhang and Jiyun Wang contributed equally to this work.
Data Availability Statement
Datas in the manuscript can be free available.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
The study was approved by the Ethics Committee of Ningbo No.2 Hospital.
Consent Statement
Informed consent has been obtained from the patient.