
Abstract
Cutaneous metastases from thyroid carcinomas are extremely rare; however, the scalp is a common site for cutaneous metastases from follicular thyroid carcinomas (FTCs). We report the case of a 77-year-old male patient with a blood-rich scalp lesion. Histopathological tests of punch biopsy specimens revealed subcutaneous well-formed follicular structures that were similar to those found in the thyroid gland. Immunohistochemistry using thyroid transcription factor-1 (TTF-1) and paired-box gene family 8 (PAX8) revealed an FTC metastasis. We performed total thyroidectomy and resection of the scalp lesion at the same time and administered postoperative radioactive iodine treatment. The primary thyroid lesion was diagnosed as an FTC based on extracapsular extension and vessel invasion. The patient has not experienced disease recurrence since the treatment. When scalp metastasis of thyroid carcinoma is suspected, we recommend total extirpation, including the primary tumor and scalp metastasis, for an improved prognosis.
Introduction
Follicular thyroid carcinoma (FTC) is the second most common type of carcinoma of the thyroid, accounting for 6–10% of thyroid carcinomas. 1 FTC is more invasive than papillary thyroid carcinoma (PTC) as vascular invasion is often recognized with FTCs, and distant metastasis is more common. FTC generally spreads via hematogenous dissemination, most commonly to the lungs and bones. Uncommon metastatic sites include the liver, adrenal glands, kidneys, pancreas, and skin. 2 Cutaneous metastasis, also caused by hematogenous metastasis, is extremely rare. We report the case of a 77-year-old patient with a blood-rich scalp metastasis from an FTC and discuss the imaging and therapeutic choices for scalp metastasis and primary thyroid lesions.
Case Report
A 77-year-old man was admitted to the dermatology department of our hospital with bulging at the scalp of his neck. He had a 2-year history of an enlarging non-tender tumor with erythema tumor on the scalp (Figure 1(A)). Ultrasonography revealed the tumor hypervascularity (Figure 1(B)). Initial presentation of the tumor at the nape of the neck. (A) The tumor is reddish and not tender. (B) The hypervascularity of the tumor is shown on Doppler-type ultrasonic flow meter imaging.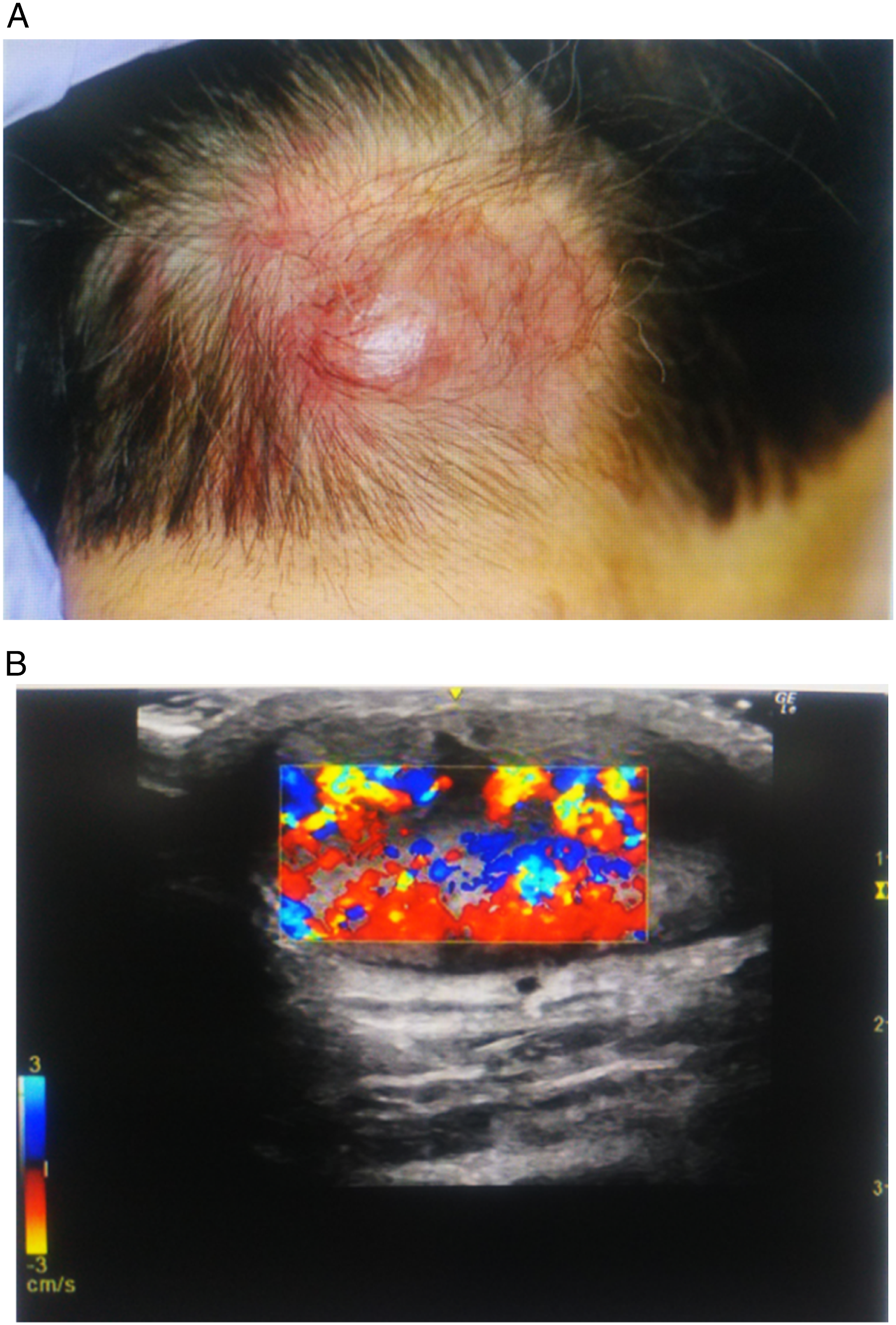
A punch biopsy of the affected section of the scalp showed an intradermal tumor composed of well-formed follicular structures such as those found in the thyroid gland (Figure 2(A)). Immunoreactivity for thyroglobulin was absent (Figure 2(B)), although immunoreactivity for thyroid transcription factor-1 (TTF-1) and paired-box gene family 8 (PAX8) was strongly positive (Figure 2(C) to (D)). Based on these results, the scalp tumor was diagnosed as being metastasis of thyroid carcinoma. Hematoxylin and eosin staining and immunochemical staining findings of the punch biopsy section. (A) Hematoxylin and eosin staining shows the follicular structures with colloid material. (B) Immunohistochemical staining with antithyroglobulin antibody is insufficient. (C) Immunohistochemical staining with anti-thyroid transcription factor-1 is positive. (D) Immunohistochemical staining with anti-PAX8 is positive.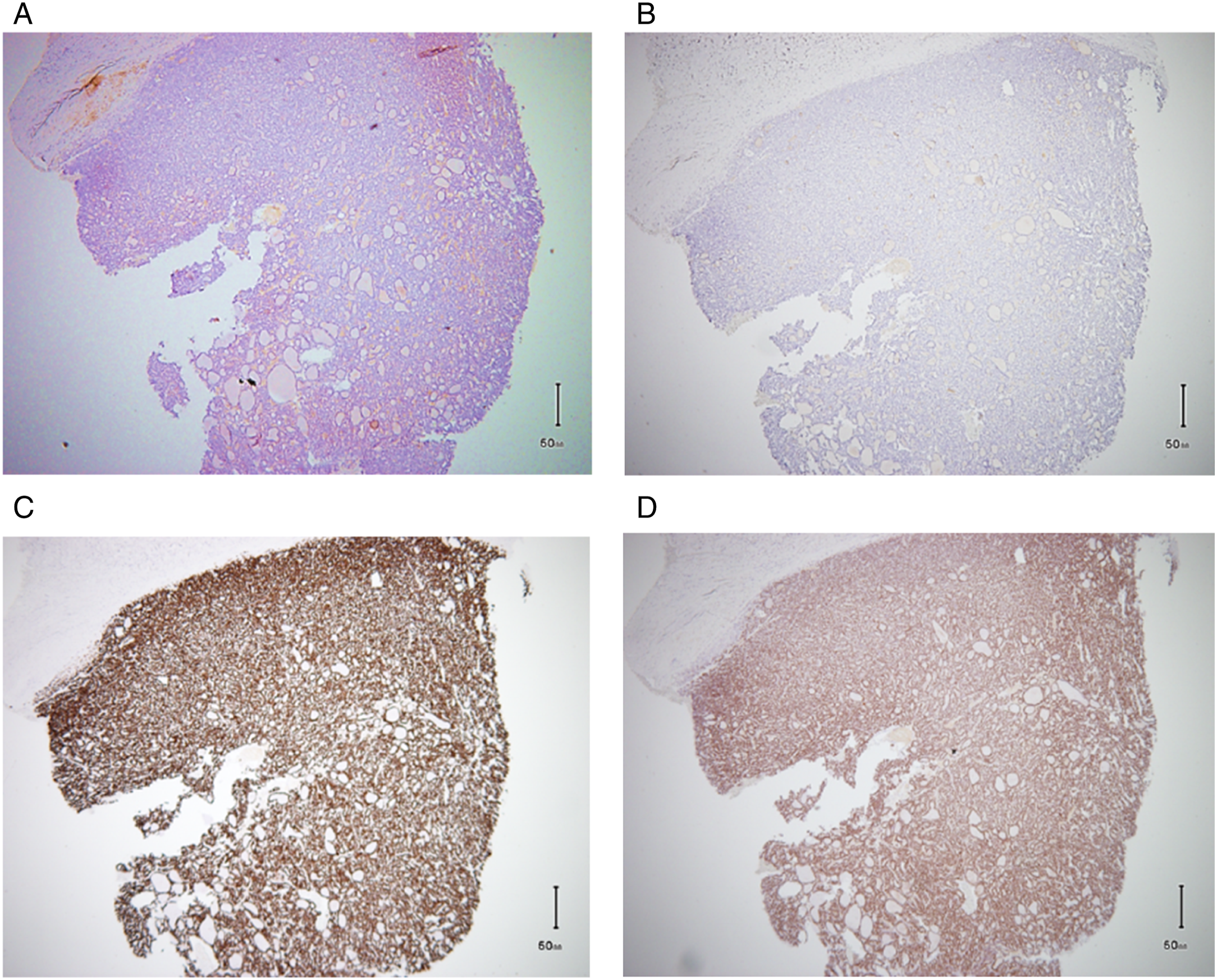
Our patient was referred for a positron emission tomography-computed tomography (PET-CT) examination to evaluate the fluorodeoxyglucose uptake of scalp lesion to determine the biopsy side and to search for other possible metastases and thyroid tumors. PET-CT images showed intense fluorodeoxyglucose uptake in the left lobe of the thyroid gland and the nape of the neck, with a soft tissue component. The maximum standard uptake values for the thyroid and scalp tumors were 5.43 and 4.21, respectively (Figure 3). The fluorodeoxyglucose-PET findings show the fluorodeoxyglucose uptake on the (A) left side of the thyroid gland and (B) nape of the neck. The maximum standard uptake values were 5.43 for the thyroid tumor and 4.21 for the scalp tumor.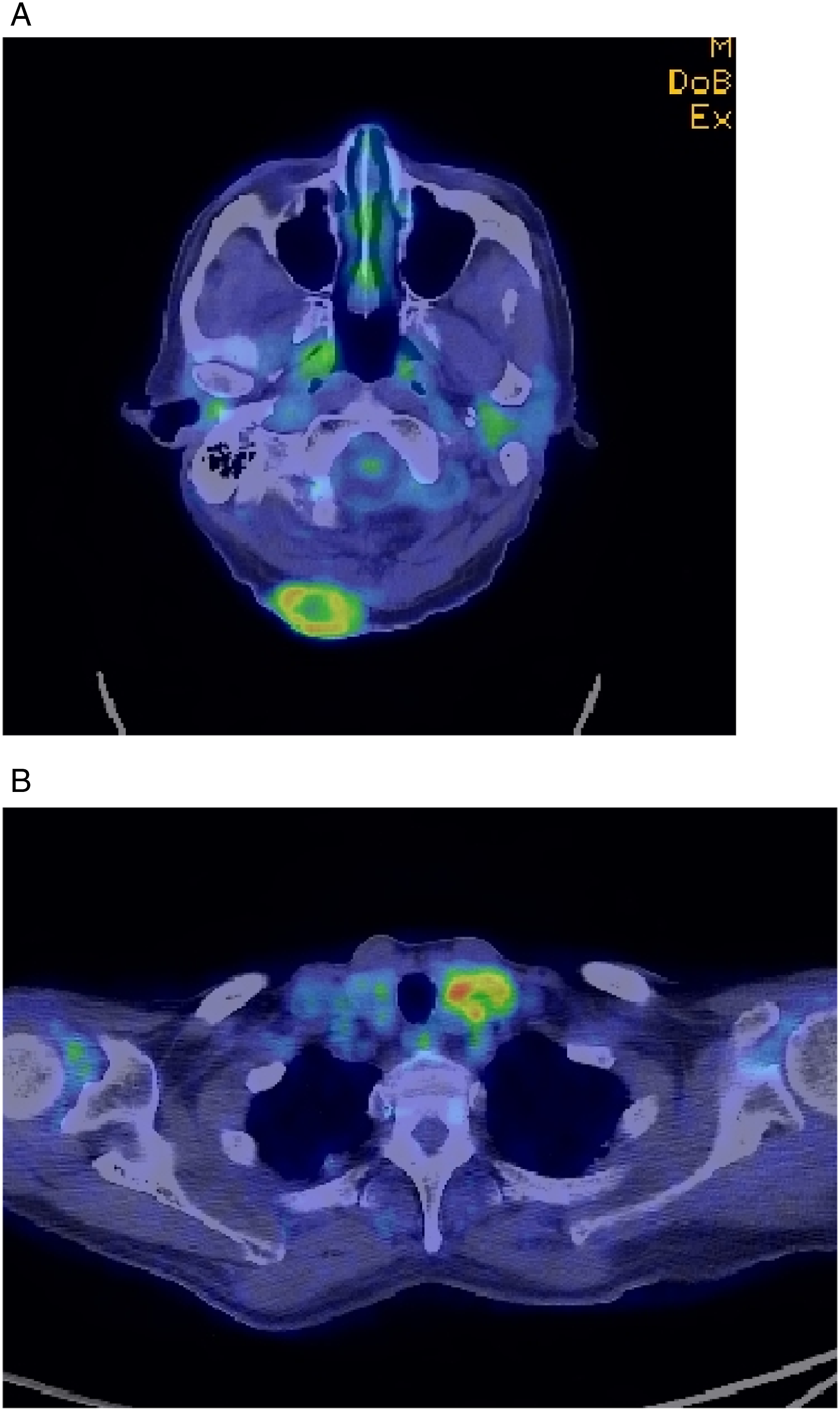
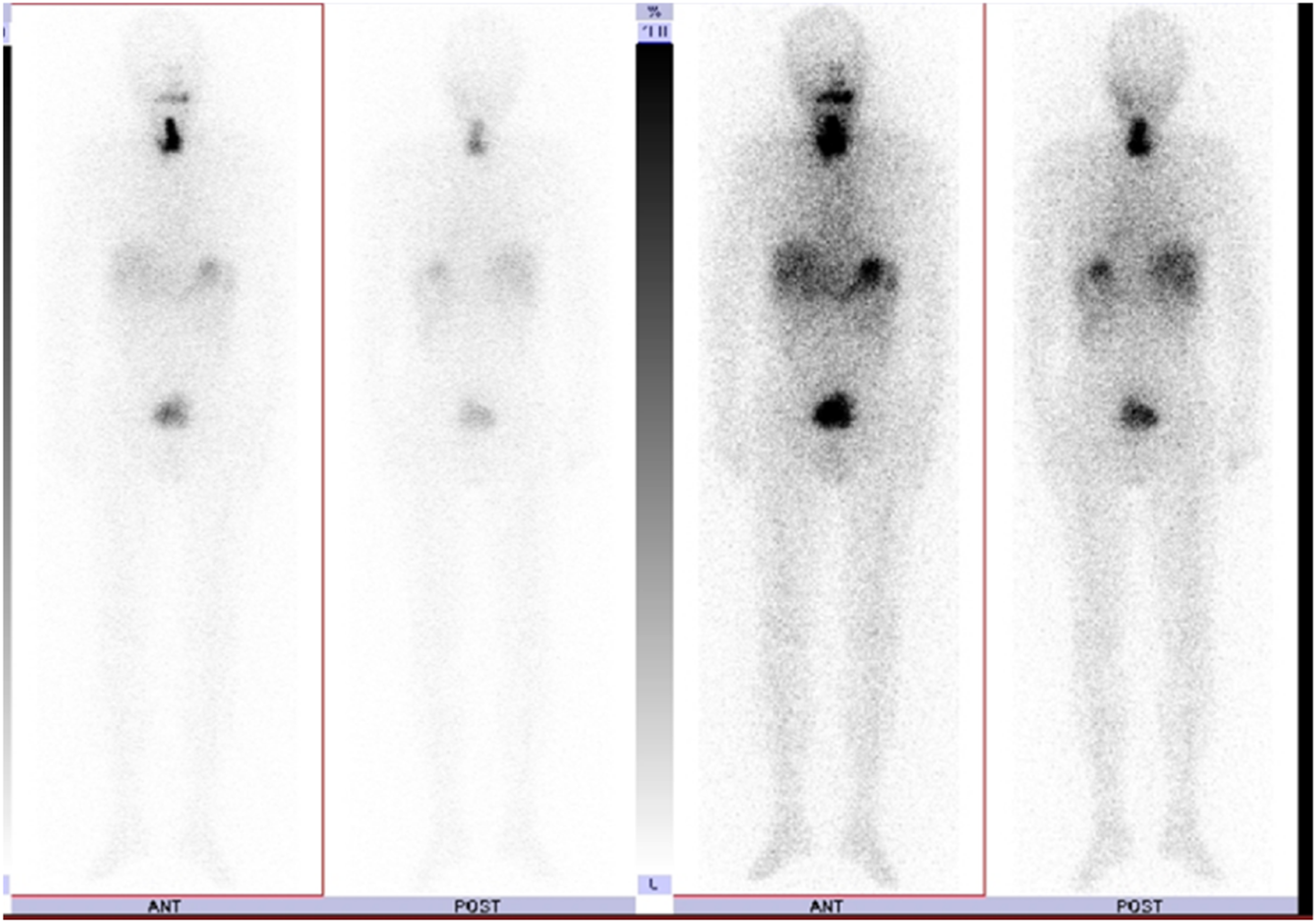
After conducting PET-CT imaging, we performed a total thyroidectomy on the patient and simultaneously resected the scalp metastasis (Figure 4). After the surgery, the patient was referred to the nuclear medicine department for radioactive iodine (RAI) therapy. High-dose I-131 was administered, and whole-body I-131 imaging was performed 3 days after the RAI therapy. The imaging showed focal uptake on the thyroid bed (Figure 5). Macroscopy of the total thyroidectomy and scalp tumor. The surgical section shows an encapsulated solid tumor with thick capsules at both the (A) primary and (B) metastatic sites. Whole-body I-131 imaging shows focal uptake on the thyroid bed.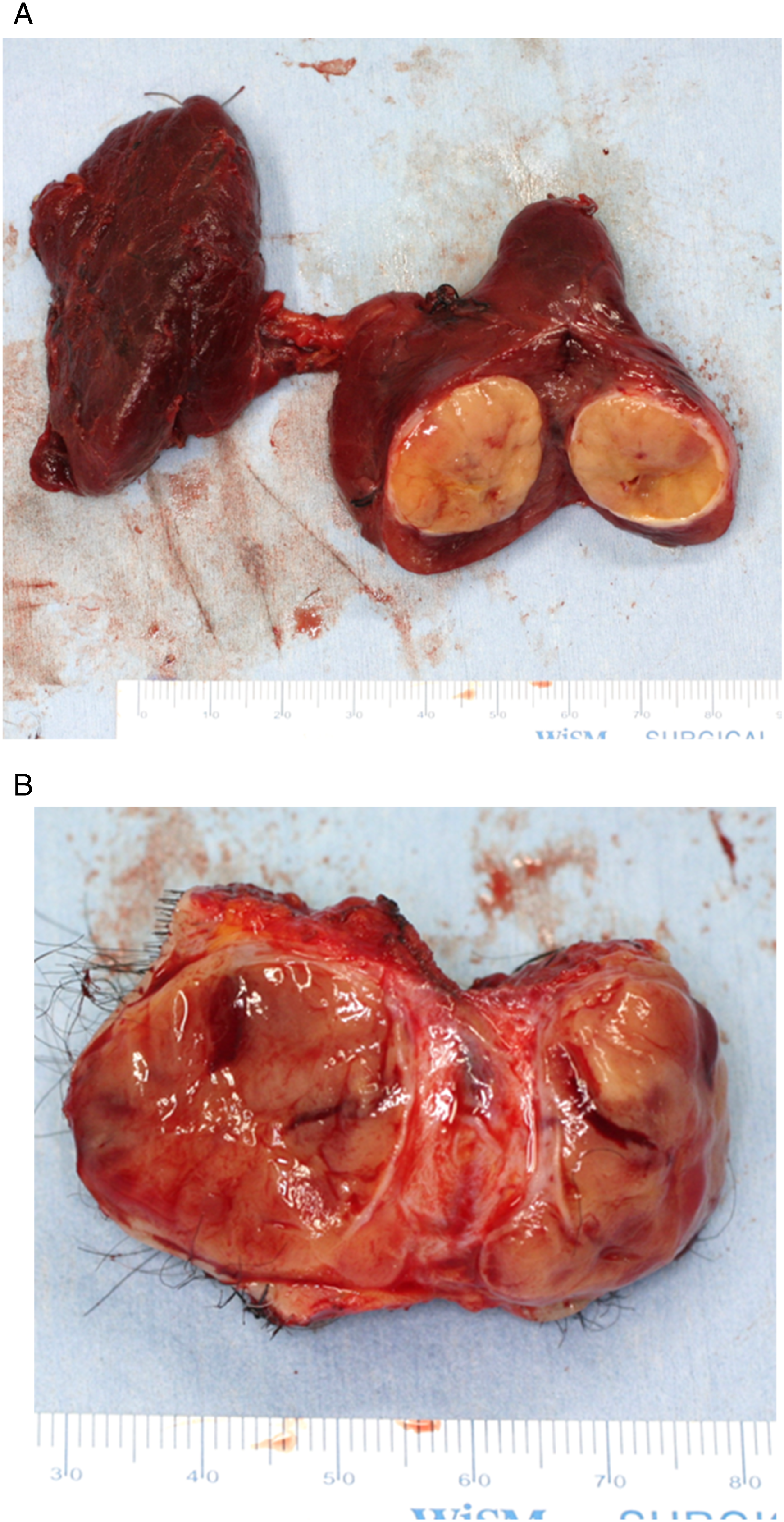
Six months after RAI therapy, the low-dose I-131 whole-body image was evaluated as no abnormalities, and the patient’s blood thyroglobulin levels were <0.05 ng/mL. The primary pathological findings were extracapsular extension and vascular invasion (in one place). Using the 2017 World Health Organization Classification of Tumors (4th edition)
1
criteria, we diagnosed encapsulated angioinvasive FTC with scalp metastasis (M1) (Figure 6). The patient has not experienced any cancer recurrence since undergoing treatment. The primary pathological finding confirmed extracapsular extension and vascular invasion in one place.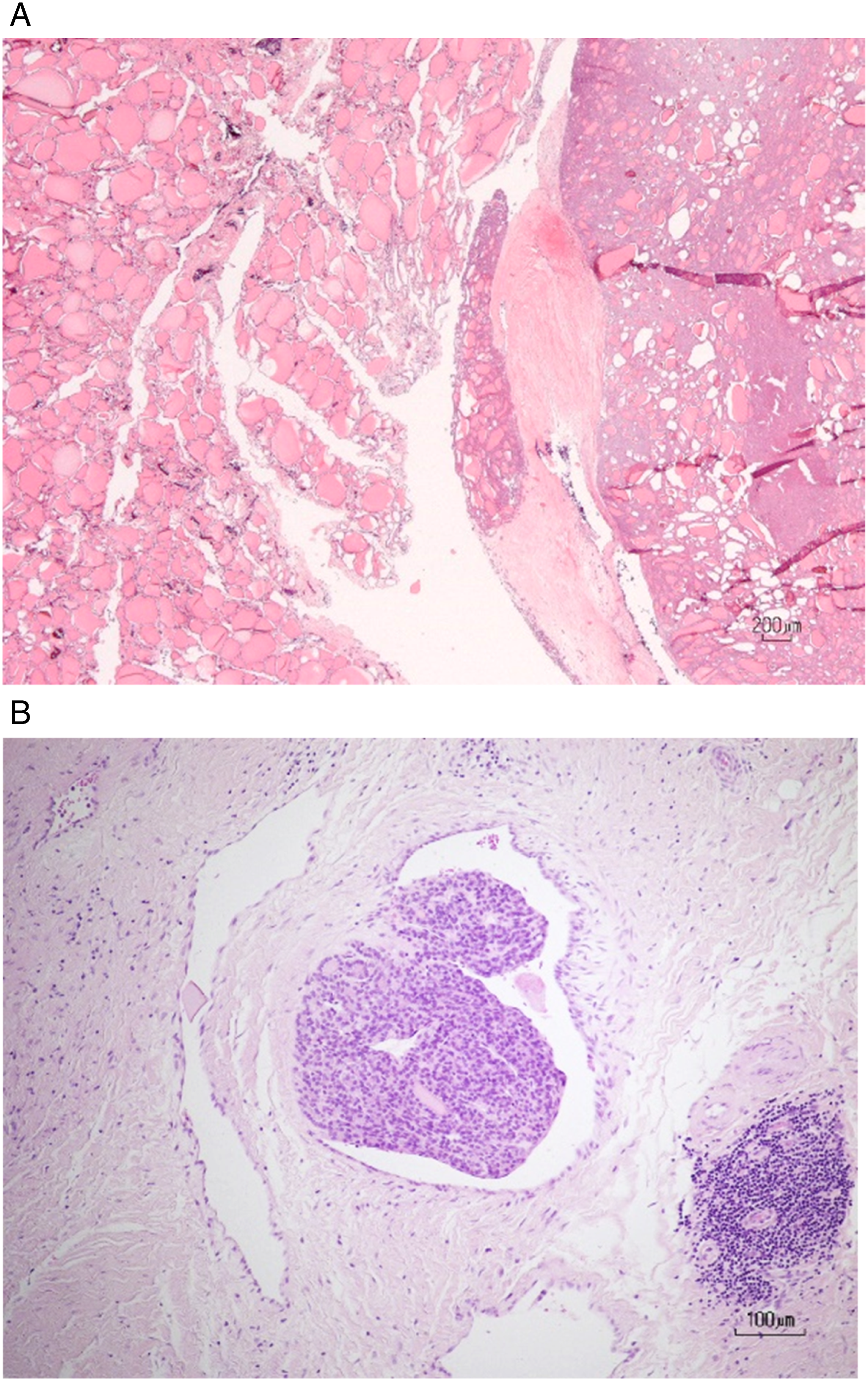
Discussion
There are 2 types of differentiated thyroid carcinoma: PTC and FTC. PTC is the most common type, and it accounts for approximately 86.2% of all cases in the USA and 93% of all cases in Japan. In contrast, FTC accounts for 6–10% of thyroid carcinomas. 1
The cytological diagnosis of FTC reflects the difficulty of thyroid cytology: diagnosis is based on the demonstration of capsular and/or vascular invasion without cellular atypia. FTC may be diagnosed only after metastasis is detected because it is difficult to distinguish FTC from follicular adenoma. The main route of FTC dissemination is via the blood, usually to the lungs and bones. Uncommonly, FTC may disseminate to the liver, adrenal glands, kidneys, pancreas, and skin. 2 Cutaneous metastasis is also caused by hematogenous metastasis; however, it is extremely rare. In a study of 724 patients, Brownstein and Helwig 3 reported only 4 cases of skin metastases from the thyroid with histological confirmation. Skin metastases of thyroid cancer are often found in the head and neck regions. Quinn et al. found scalp metastases in 9 of 14 patients with cutaneous metastases of FTC. 4 Dhal et al. reviewed 43 patients with skin metastases from thyroid carcinoma. PTC was the most common (41%), followed by FTC (28%), anaplastic carcinoma (15%), and medullary carcinoma (15%). 5
Vives et al. reviewed 21 cases of cutaneous metastases from thyroid carcinomas. These included 6 FTCs, 5 PTCs, and 4 giant-cell carcinomas. Although papillary carcinoma is the most common type of thyroid cancer, many follicular carcinomas metastasize to the skin. Follicular carcinoma can easily cause hematogenous metastasis to the cutaneous region. The scalp is the most common site for metastasis. 6 We consider that the rich blood supply to the scalp is the main cause of hematogenous metastasis in this area, given the many published reports similar to our case.
The 2017 World Health Organization guidelines 1 classify FTC into 3 subgroups: (1) minimally invasive (MI, capsular invasion only), (2) encapsulated angioinvasive, and (3) widely invasive. 1 O’Neill et al. showed disease-free survival rates were 97%, 81%, and 46% in 3 groups of FTCs (group 1: capsular invasion-only MI-FTCs, group 2: angioinvasive MI-FTCs, and group 3: angioinvasive widely invasive FTCs, respectively). 7 Based on the study by O’Neil et al., the fourth edition of the WHO classification divides MI-FTCs into 2 subgroups: capsular invasion-only MI-FTCs and encapsulated angioinvasive FTCs.
Patients with tumors with limited vessel invasion (<4) have a better prognosis than those with tumors with extensive vascular invasion. 8 Vascular invasion is often prominent, but alone, it does not categorize an FTC as widely invasive. Identification of extensive angioinvasion, which is associated with a poor prognosis, is more important than the extent of invasion of the thyroid or soft tissue. The tumor in our case was encapsulated, angioinvasive (<2), and with scalp metastasis.
In some cases, the initial symptom is metastasis, and with FTC it is not unusual for a primary tumor to be diagnosed based on distant metastasis. Koller et al. reported that cases showing metastasis and primary tumor simultaneously, or cases in which metastasis developed earlier than the primary tumor were half. 9 Sugino et al. reported that the prognosis of the group with distant metastases at pretreatment was significantly poorer than that of the group without distant metastases at pretreatment. 10 Quinn et al. 4 reported that patients with extracutaneous disease at the time of cutaneous metastasis of FTC may have a worse prognosis than those with isolated cutaneous metastases. Farina et al. 2 reported that metastases in rare sites do not always represent a negative prognostic factor for disease outcome and, in fact, can occur as single distant lesions; if surgically resectable, their treatment can also lead to local disease remission. As metastasis was a single, distant lesion in our case, we resected the primary site and metastasis at the same time. Our patient had a good prognosis.
FTC expresses cell-lineage-specific thyroglobulin and TTF-1, and PAX8 is usually positive. 1 Immunohistochemical tests using these markers and tissue samples are therefore essential to confirm a diagnosis. We performed immunohistochemical examinations using antithyroglobulin antibody, TTF-1, and PAX8. In our case, the primary site was positive for all 3 tests, but the metastatic site was insufficient for antithyroglobulin antibody. When scalp metastasis of FTC was suspected, we performed an immunohistological test on the biopsy lesion. The primary thyroid lesion in our case was suspected on fluorodeoxyglucose-PET, and we examined the thyroid gland using ultrasonography. PET-CT may be effective in detecting primary tumors in cutaneous metastases.
Sager et al. reported that in scalp metastasis of FTCs, the best treatment option is resection of the lesion, followed by thyroid tissue ablation with RAI and thyroid-stimulating hormone suppression. 11 However, the efficacy of thyroid-stimulating hormone suppression remains controversial. Our patient underwent total thyroidectomy and simultaneous resection of the scalp metastasis, followed by radioactive iodine treatment after surgery. Currently, the patient has no recurrence.
When a lesion on the scalp is suspected to be metastasis, we recommend performing a biopsy of the tumor and conducting immunohistological tests for pathological diagnosis confirmation. In addition, the thyroid gland should be inspected using ultrasonography.
When metastasis of thyroid carcinoma is confirmed, we recommend performing total extirpation of the primary tumor and scalp metastases to improve the patient’s prognosis.
Footnotes
Acknowledgements
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.