
Abstract
A frontal sinus cutaneous fistula (FSCF) is a rare and challenging condition. Remarkable advancements in endonasal endoscopic surgery (EES) have enabled the treatment paradigm for a FSCF to gradually shift from open procedures to ESS. Nevertheless, the experience of EES for a post-trephination-related FSCF is rare, especially in patients with a pronounced frontal recess (FR) ossification. Here, we report an endoscopic strategy for successfully treating a post-trephination-related FSCF with complete ipsilateral FR neo-osteogenesis. Through two surgical corridors created by the modified mini-Lothrop procedure and an ipsilateral frontal osteotomy window, we established a patent drainage pathway from the affected side to the opposite side. This strategy may prevent potential orbital and cranial base injuries from affecting the ossified region of the ipsilateral FR. Moreover, in addition to the advantage of aesthetic outcomes, the procedure allows a single-stage surgery and facilitates the debridement and surveillance of the wound through the drainage pathway postoperatively. In conclusion, this technique could be a feasible endoscopic strategy for a FSCF, regardless of the severity of the FR ossification.
Introduction
A frontal sinus cutaneous fistula (FSCF) is a rare but challenging condition that is often a consequence of Pott’s puffy tumor (PPT), a clinical entity characterized by subperiosteal abscess and osteomyelitis.1 -3 Surgical management is the mainstay for treating a FSCF, with the open procedure remaining the standard strategy as it maintains low recurrence and revision rates.4,5 However, an open approach may lead to significant aesthetic and functional morbidities; thus, intervention should be carefully planned to ensure its therapeutic efficacy against potential complications.4,5
Endonasal endoscopic surgery (EES) has become preferred over open procedures for managing various sinus and extrasinus conditions because it provides better visualization, lower invasiveness, and an incision-less approach. 6 Recent investigations on the treatment of a FSCF have shifted from open procedures to the endoscopic approach completely or partly, in combination with an open procedure.3,6 However, most of these surgical experiences are related to PPT or mucocele, 7 and the diseases are inherently characterized by an apparent bone destruction, which could lessen the potential benefit of the endoscopic approach. However, evidence regarding the feasibility of ESS for a post-trephination-related FSCF remains limited, particularly in patients with underlying recalcitrant chronic rhinosinusitis (CRS). One reason for this is that refractory CRS is often associated with overt osteitis and fibrosis. 8 After tissue remodeling, dissection of the restricted and distorted frontal recess (FR) may potentially increase the risk of inadequate drainage pathways or endanger nearby structures, such as the orbit or skull base.
In this study, we aim to describe the outcomes of endoscopic treatment in a patient with recurrent CRS complicated by an iatrogenic FSCF with ipsilateral complete FR neo-osteogenesis after multiple bilateral ESS and a frontal sinus trephination.
Case Report
A 63-year-old male patient visited our clinic with a recurrent frontal discharge over the last 3 years. He had a history of multiple sinus surgeries: the first one was performed for rhinosinusitis with polyps, and then subsequent surgeries were performed for residual frontal sinusitis. He stated that he experienced refractory symptoms since the most recent procedure, which involved external frontal trephination with a rubber tube placement for the drainage of purulent material. Physical examination revealed a draining fistula below the patient’s right eyebrow, accompanied by a swelling of the upper eyelid (Figure 1A). The laboratories demonstrated an elevated blood eosinophil percentage of 8.3% and an immunoglobulin E level of 533.3 IU/mL but a normal white blood cell count of 6450 mm3. A culture of the lesion revealed the presence of Pseudomonas aeruginosa. Treatment with ciprofloxacin for 2 weeks provided a temporary relief, but the refractory discharge resumed shortly thereafter. Sequential endoscopy revealed scarring over the right frontal outlet without secretions, suggesting the complete stenosis of the frontal opening, which prevented the drainage of the frontal sinus. Computed tomography confirmed this finding, as it showed an extremely thickened bony wall of the right frontal sinus with a draining fistula on the external skin (Figure 1B and C). Considering the refractory situation, we performed an endoscopic surgery to address the issue. The surgical steps are illustrated in Figure 2, and the surgical procedures are shown in detail in Figure 3A to F. The patient’s postoperative course was uneventful. Endoscopic finding and external photograph were taken 4 months postoperatively, as illustrated in Figure 3G and H, which show that the sinus is now clear and the frontal sinus drainage pathway is patent. The cosmetic appearance was favorable, and the patient has remained disease-free for 17 months postoperatively.
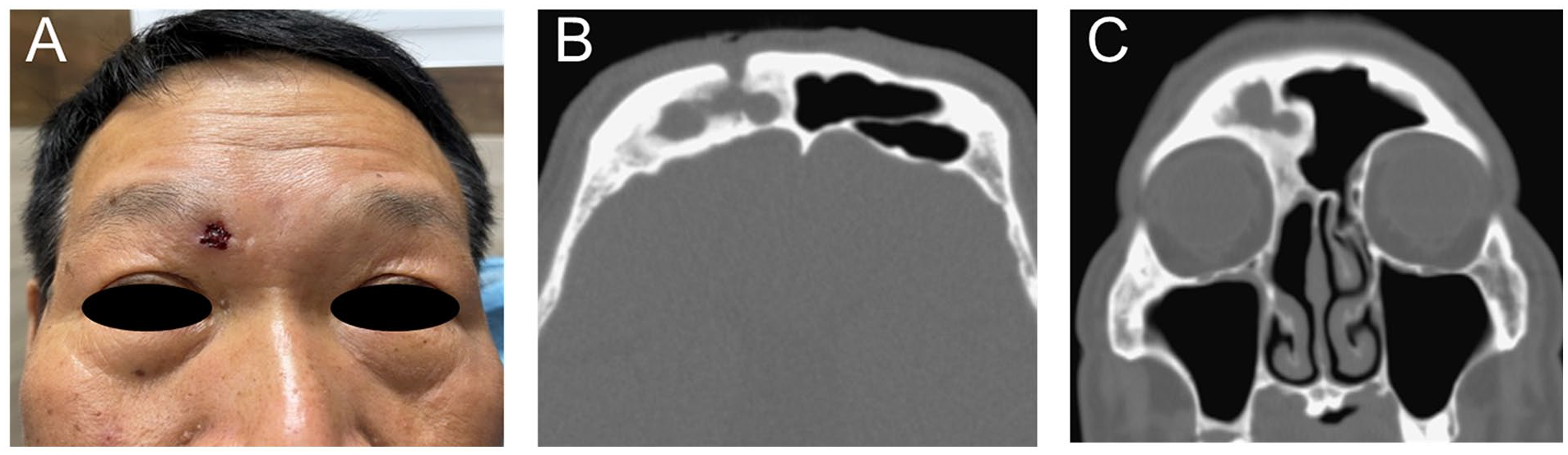
Pre-surgical photograph and computed tomography scans of the patient. (A) A preoperative photo showing a fistula above the eyebrow, overlying the right FS. Axial computed tomography (B) and coronal (C) views showing a bony defect over the anterior table of the FS that communicates with the external skin. The bony compartment of the FS is significantly thickened, with complete neo-osteogenesis of the frontal drainage pathway. FS, frontal sinus.
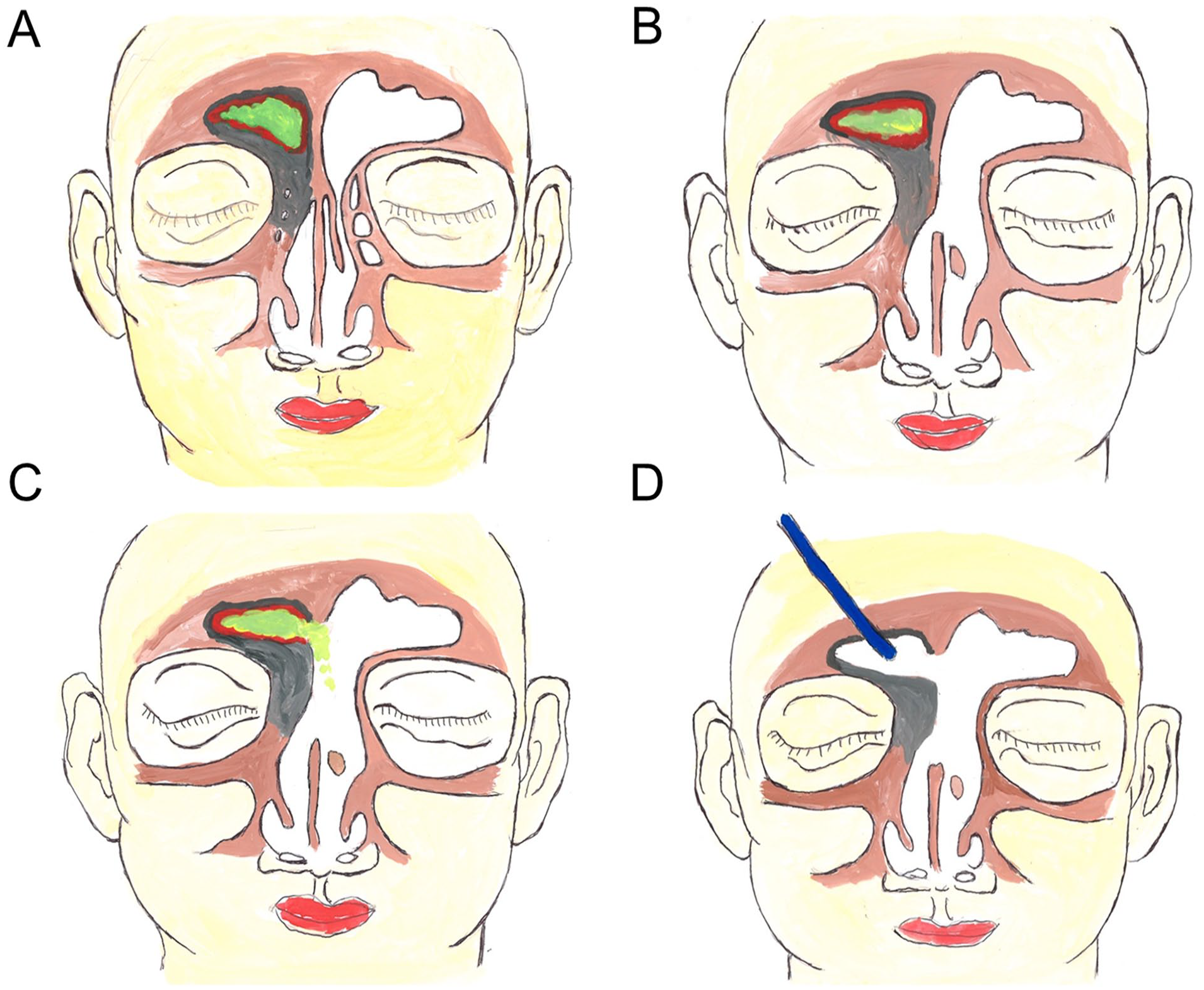
Schematic illustration of our surgical steps. (A) The disease extent and the complete neo-osteogenesis of the ipsilateral FS (gray color, ossification; red color, diseased frontal mucosa; green color, frontal sinus secretion). (B) The extent of contralateral Draf IIB frontal sinusotomy and superior nasal septectomy. (C) The extent of the modified mini-Lothrop procedure by additional removal of the ISS of the FS. (D) Removing FS mucosa and the residual ISS of the FS from the frontal osteotomy window using endoscopic surgery. FS, frontal sinus; ISS, intersinus septum.
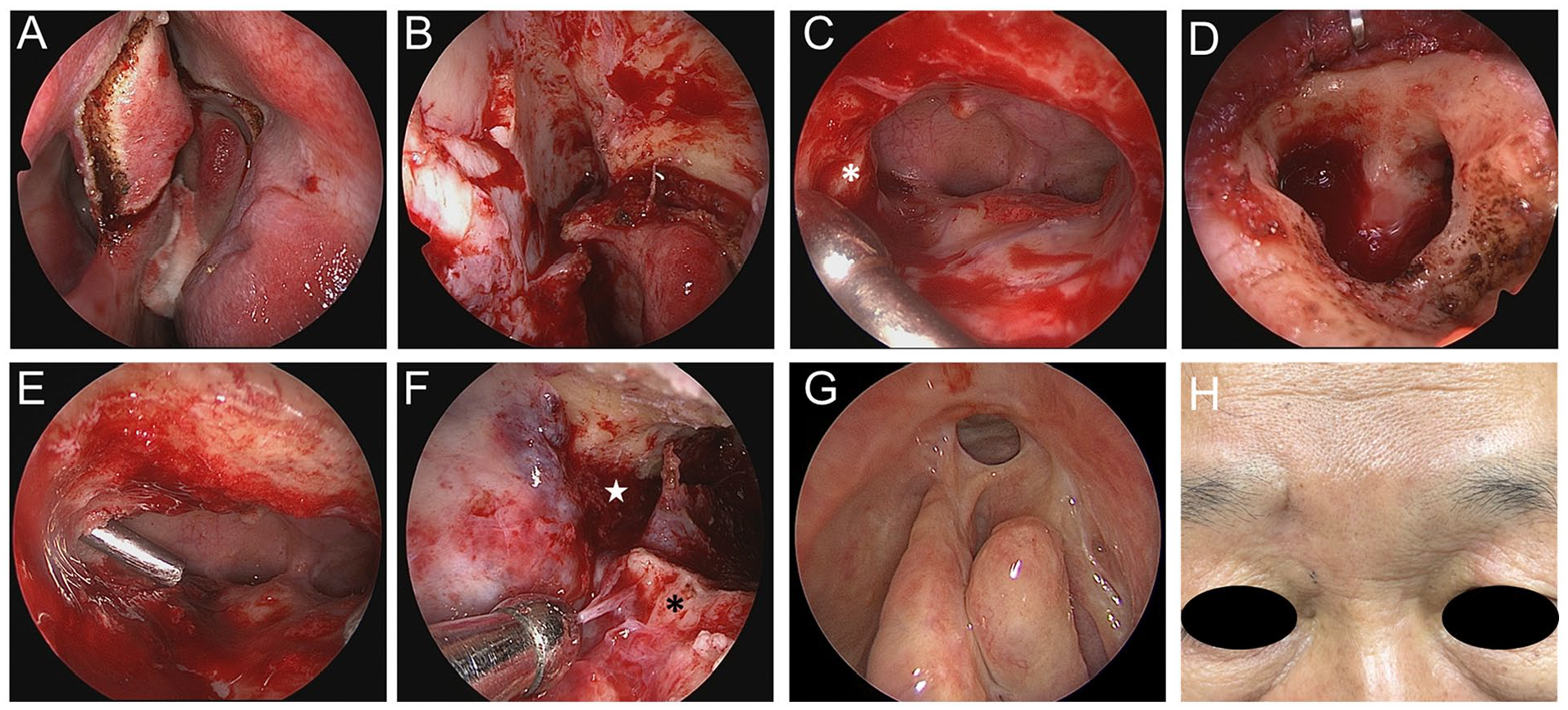
Surgical steps and post-surgical images of our case of trephination-related-FSCF with complete ipsilateral FR neo-osteogenesis. (A) An incision made above the iatrogenic septal perforation using a Colorado® microdissection needle (Sryker, Inc., Kalamazoo, MI, USA). (B) The raised lateral-inferior-based pedicle mucosal flap and the exposed anterior skull base and lateral nasal wall of the opposite side. (C) A view after completing the contralateral Draf IIB procedure by removing the bony structures surrounding the FR, superior nasal septum, and the superomedial attachment of the middle turbinate, leaving a thin shell of bone anteriorly and laterally. The left frontal sinus is exposed, showing intact mucosa. The suction tip indicates the ossified FR (asterisk). (D) The frontal osteotomy window after removing the FSCF. (E) The frontal sinus intersinus septum above the neo-osteogenic region perforated by drilling through the MMLP corridor. (F) The endoscopic findings of the ipsilateral bony obliterated region (asterisk) and contralateral drainage pathways (star) observed using a 0° endoscope through the frontal osteotomy window after the complete removal of the intersinus septum and mucosal lining through both surgical corridors. (G) Endoscopic examination revealing clear sinus mucosa with a patent outflow pathway inside the left frontal sinus. (H) The external photograph taken 4 months postoperatively showing the condition of the patient. FR, frontal recess; FSCF, frontal sinus cutaneous fistula; MMLP, modified mini-Lothrop procedure.
Discussion
Advancements in EES have dramatically reduced the need for external approaches in treating various sinonasal pathologies. However, certain conditions such as a FSCF or frontal sinus osteomyelitis pose a challenge for endoscopic surgery. A study by Thomas et al 2 on the feasibility of using endoscopic or endoscopic-assisted approaches in 16 patients with frontal sinus osteomyelitis suggested that these approaches should be avoided if the ipsilateral frontal sinus drainage pathway (FSDP) has more than 50% narrowing or a small anteroposterior diameter of less than 8 mm. 2 In contrast, open procedures such as the Riedel procedure, osteoplastic flap, or cranialization should be considered for these patients to reduce failure rates or detrimental complications in the orbital or skull base. 2
The modified mini-Lothrop procedure (MMLP), also known as the Eloy IID procedure, 9 is a promising approach of endoscopic surgery in cases of unilateral frontal sinus disease, particularly when the frontal sinus recess on the same side is inaccessible.10,11 This procedure involves a Draf IIB on the opposite side and a complete frontal intersinus septectomy to address the ipsilateral lesions.10,11 In a study on 4 patients with a frontal outlet obstruction due to neo-osteogenesis or orbital herniation, all experienced symptoms resolved after undergoing the MMLP, and openings became patent without mucostasis for 9 to 28 months of follow-up. 11 In addition to its cosmetic benefits and low risk of complications compared to those of external approaches, the MMLP offers an additional advantage of less dissection than that in traditional drill-out procedures. This results in a decreased surgery time. 11 However, certain limitations must be considered when performing this surgery, such as the increased risk of restenosis if the contralateral FR and frontal intersinus septectomy are inadequate, the possible need for removing a part of the nasal septum to improve visibility and maneuverability in the limited-sized frontal sinus, and the potential insufficiency of the surgical corridor for managing complex or far lateral frontal sinus lesions. 11
The frontal osteotomy window following the fistulectomy can provide an additional corridor for removing the ipsilateral frontal sinus mucosa. 12 This is similar to the canine fossa trephination for treating maxillary sinus pathologies. 13 With the assistance of a high-resolution angled endoscope, we can clearly visualize and directly access the affected areas located at the lateral most extent of the frontal sinus or regions that are above or behind the neo-osteogenesis; such locations are inaccessible through the contralateral exposure by the MMLP.10,11 The trephination window may also help in maximizing the frontal intersinus septectomy, 12 thus reducing the risk of circumferential restenosis and improving bilateral sinus drainage by the MMLP. Our strategy of performing frontal trephination to assist endoscopic frontal sinusotomy has been supported by previous successful experiences. 14 Geltzeiler et al 14 carried a study on performing frontal sinus mega-trephination for 64 complex frontal pathologies, whereas 54 cases were employed together with a frontal sinusotomy, and they found that the combined approach was well-tolerated and did not increase surgery-related comorbidities.
In this case, we did not employ a pure frontal intersinus septum takedown, a surgical technique proposed by Pope and Thompson in 1976, 15 to divert the diseased material to the healthy side, as a patent FSDP is required for this technique to be effective. 12 The contralateral frontal outflow patency is a significant concern in this case, as the patient had previously undergone endoscopic management of the contralateral FR twice, which could have resulted in the scarring of the drainage pathway. This was confirmed during the intraoperative assessment, which revealed that the contralateral FSDP was significantly narrowed. Another advantage of performing the contralateral MMLP is that it allows the debridement and surveillance of the wound through the open drainage pathway obtained. This is also useful in cases where there is a concern of a residual or recurrent disease, as it provides an easier access to the surgical site to perform follow-up procedures or further interventions, if needed. Moreover, despite being time-consuming and complex, the strategy of performing the contralateral MMLP and ipsilateral frontal trephination allows for a single-stage intervention, which can be more convenient and efficient for both the patient and the surgical team.
Conclusion
In conclusion, we successfully performed single-stage surgery by combining the endoscopic MMLP and frontal sinus trephination following fistulectomy for treating a post-trephination-related FSCF. With a thorough anatomic consideration and refinement of surgical techniques, we have found that the current approach may minimize cosmetic issues and maintain patent frontal outflow drainage to prevent recurrence. This implies the feasibility of one-stage endoscopic surgery in patients with FSCF despite the complete ossification of the ipsilateral FR.
Footnotes
Authors’ Note
This manuscript is original and it, or any part of it, has not been previously published, nor is it under consideration for publication elsewhere.
Author Contributions
LYH was involved in concept and design. LYH, CPF, and SYL were involved in acquisition, analysis, or interpretation of data. LYH was involved in drafting the manuscript. LYH was involved in critical revision of the manuscript for important intellectual content. LYH, CPF, and SYL were involved in final approval.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Yen Tjing Ling Medical Foundation (CI-112-24).
Compliance With Ethical Standards
The protocol of this study was approved by the institutional review board of Kaohsiung Veterans General Hospital (KSVGH 22-CT12-10).
Informed Consent Statement
Written informed consent was obtained from the patient.