
Abstract

Significance Statement
A frontal sino-cutaneous fistula is an abnormal connection between the frontal sinus and the skin. They usually occur as a consequence of frontal osteomyelitis with subperiosteal abscess formation (Pott’s puffy tumour) or of an infected mucocele. 1 They are rare in the post-antibiotic era. 2 Here, we present a case of a frontal sino-cutaneous fistula, masquerading as a basal cell carcinoma of the medial canthus, that resolved completely following a modified endoscopic Lothrop procedure.
Case Report
A 76-year-old female was referred to the dermatology skin cancer clinic with a 2- to 3-month history of a crusting, bleeding lesion of the medial canthus (Figure 1). After clinical examination including dermatoscopy, a provisional diagnosis of basal cell carcinoma was made and the patient listed for Mohs micrographic surgery under local anaesthetic. Appearance of medial canthus pre- and post-Mohs surgery.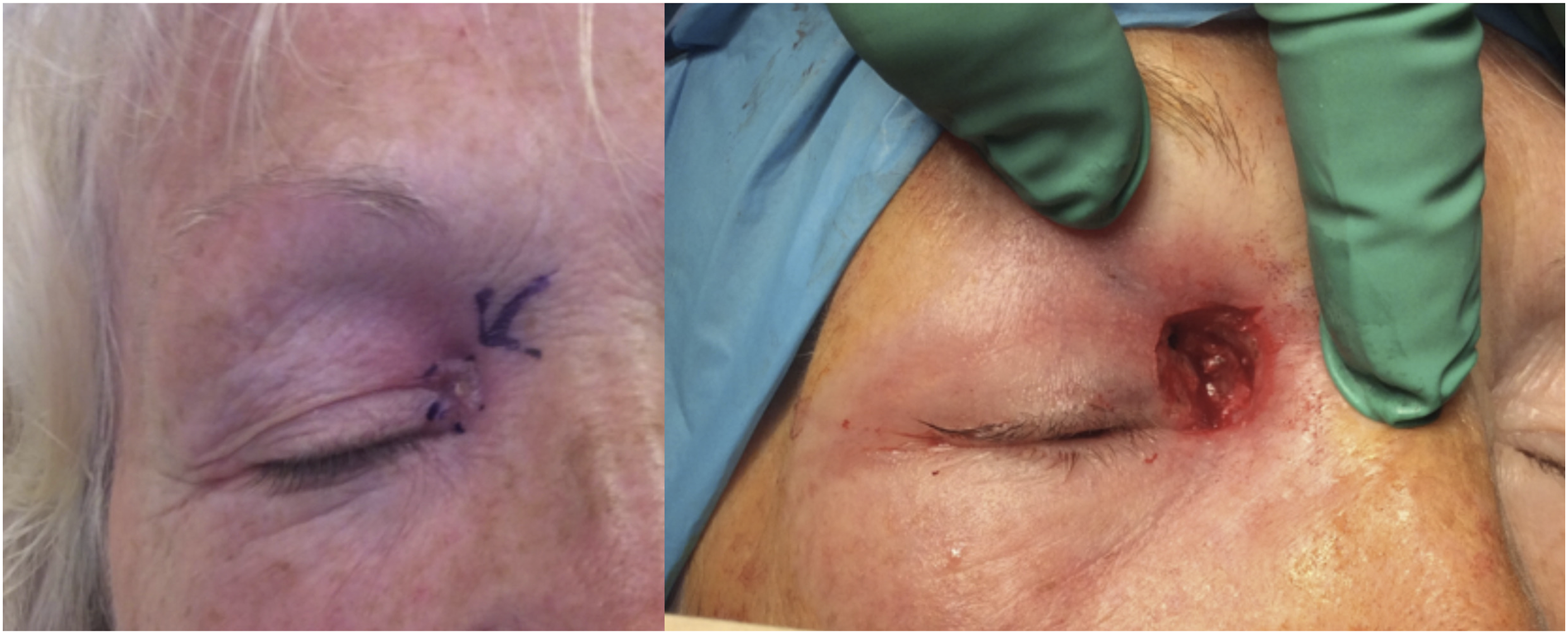
Intra-operative frozen section at the first 2 levels of excision demonstrated only fibro-fatty inflammation with no evidence of tumour. A ‘flow of white pus’ was noted from the base of the wound, and it was felt primary closure inappropriate due to the persistent discharge. The wound was dressed, and an urgent CT sinus was performed due to concerns over a sinogenic origin. This demonstrated complete opacification of the frontal, ethmoid and maxillary sinuses with sclerosis of the frontal bone in keeping with chronic inflammation. More pertinently, it showed a defect within the right frontal recess with extension of sinus contents to the region of the right medial canthus (Figure 2). A diagnosis of a frontal mucocele with a sino-cutaneous fistula was made, and the patient was referred urgently to the rhinology service. Coronal CT and T2 mDIXON MRI images demonstrating a defect in frontal recess and postcontrast enhancement of mucosa and soft tissues continuous from the right frontal sinus to the medial canthus.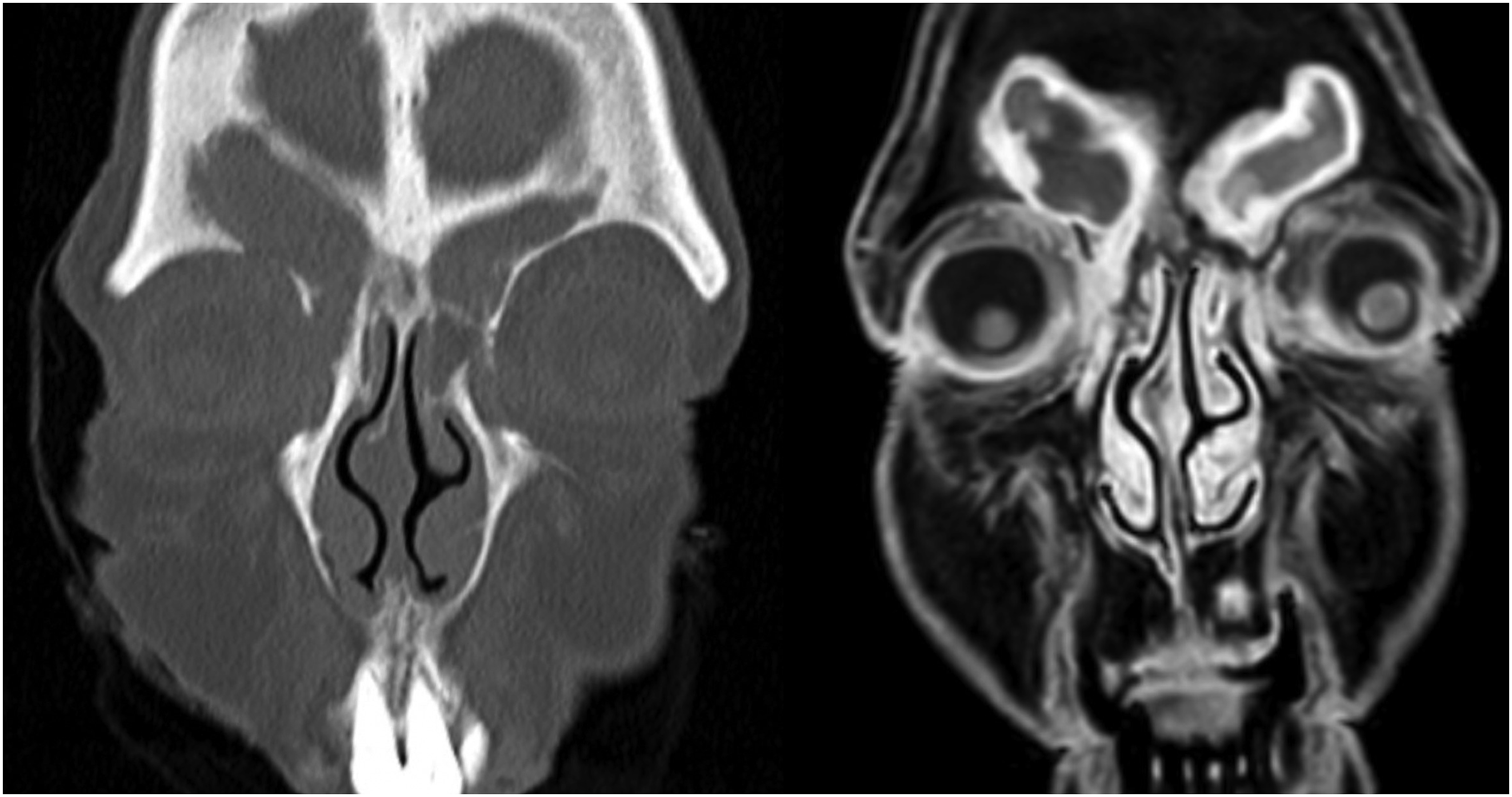
The patient reported no sinonasal symptoms and had no history of previous sinus disease or surgery. Nasal endoscopy was normal. A 2.5cm cutaneous defect was present at the medial canthus with obvious purulent discharge. The patient underwent functional endoscopic sinus surgery (FESS) with full skull base clearance and a Draf 3/modified endoscopic Lothrop procedure (MELP) was performed. The fistula tract was not violated, and the bony defect was likewise left alone.
Post-operatively, the patient was commenced on a 1-week course of oral antibiotics and advised to perform high-volume low-pressure nasal douching 4 times a day. At a 3-week post-op review, the frontal sinus cavity remained patent and the original medial canthal wound had healed by secondary intention, with no external intervention, leaving an exceptional aesthetic result. At her most recent clinical review, 3 months following surgery, she remained asymptomatic from her sinuses, with no discharge from the healed wound and a patent frontal neo-ostium (Figure 3). Left: Healed medial canthus following the modified endoscopic Lothrop procedure. Right: Endoscopic view of left frontal recess demonstrating patent neo-ostium of right frontal sinus. 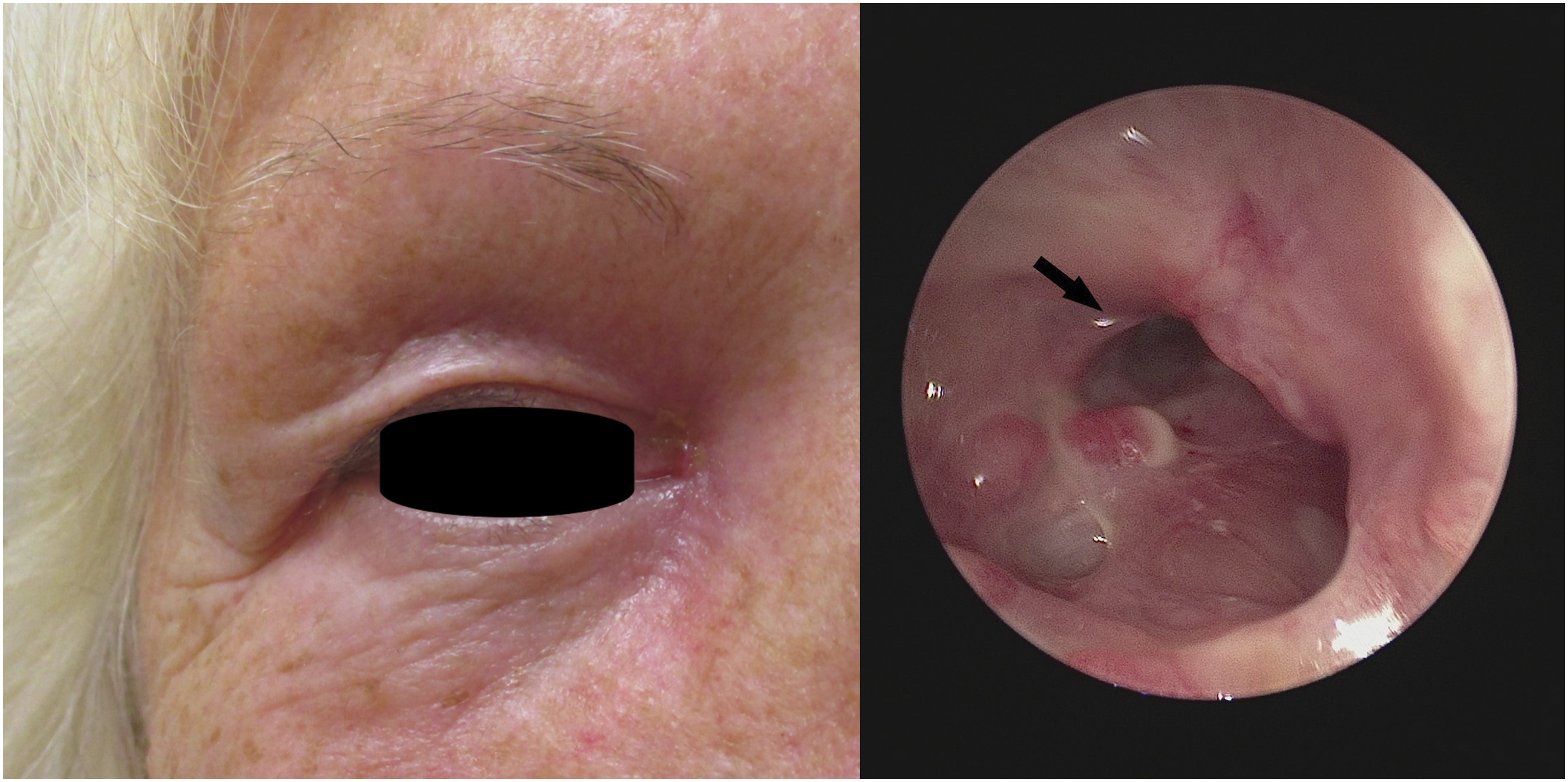
Discussion
The frontal sinus is prone to obstruction due to its complex, narrow drainage pathway, although in our case, significant, bony sclerosis of the frontal outflow tract is the likely cause of the pathology. Obstruction of this pathway with retention of secretions can lead to chronic inflammation and sinusitis or mucocele formation. Frontal mucoceles are prone to secondary infection with pyomucocele formation. Frontal sino-cutaneous fistula is an uncommon, but recognised complication of frontal sinusitis.1. Patients usually present with symptoms of headache and nasal congestion in the period prior to development of the cutaneous discharge. 1
There are previous reports in the literature of sino-cutaneous fistulas being misdiagnosed as epidermoid cysts 3 and of odontogenic fistulas mimicking basal cell carcinoma 4 and squamous cell carcinoma. 5 However, to our knowledge, there are no reports of painless frontal sino-cutaneous fistulas masquerading as basal cell carcinoma.
Due to the unusual nature of the presentation, there is no consensus on the most appropriate management strategy for frontal sino-cutaneous fistulae. Previously described methods include obliteration of the fistula cavity with omentum followed by coverage with a local pedicled forehead flap. 6 This was successful but does leave significant scarring and a potentially poor cosmetic result. Other authors have described trans-fistula obliteration of the sinus, but this does leave potential for mucocele development if the mucosa is not completely removed. 7
Our case demonstrates that by simply re-establishing the frontal sinus drainage pathway through a wide surgical neo-ostium, the fistula tract can heal spontaneously with excellent cosmetic results and prevent recurrent mucocele and fistula reformation. The Draf 3/MELP should be considered the gold standard procedure for complex pathology of the frontal sinus. Increased access to high-quality endoscopic and image guidance technology is making endonasal frontal sinus surgery more accessible and achievable, permitting a low morbidity option for dealing with fistulas originating from the frontal sinus.
Footnotes
Declaration of conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written consent for publication was gained from the patient prior to manuscript submission.