
Abstract
Objective:
Prelacrimal recess approach can be used to access lesions of the anterior wall of the maxillary sinus (MS). Moreover, the longer the prelacrimal recess window distance (PLRWD), the easier it is to access the anterior wall. This study aimed to define the correlation between maxillary sinus pneumatization (MSP) and PLRWD, a previously defined anatomic factor predictive of the ease of prelacrimal recess approach (PLRA).
Methods:
In total, 506 sides of 253 participants were studied. In the axial image, the PLRWD, the distance between the anterior wall of the MS and the lacrimal duct, was measured through radioanatomical analysis and classified as type I (<3 mm), type II (3-7 mm), or type III (>7 mm). On the coronal image, the distance between the nasal floor and the lower end of the MS was measured. When MSP did not reach the nasal floor, it was classified as grade I, as grade II when MSP reached the nasal floor, and grade III when the MS was pneumatized below the nasal floor.
Results:
Type I included 115 sides (22.7%); type II, 277 sides (54.7%); and type III, 114 sides (22.5%). Grade I was observed in 58 sides (11.5%), grade II in 38 sides (7.5%), and grade III in 410 sides (81.0%). The mean PLRWD of grade I was 2.35 ± 2.41 mm, II was 3.37 ± 2.46 mm, and III was 5.55 ± 2.54 mm, showing a significant difference (P < .001). Post hoc analysis showed significant differences in the mean PLRWD among grades I, II, and III. Two anatomical factors, the MSP and PLRWD, were positively correlated (r = .507, P < .001).
Conclusions:
This study demonstrates a correlation between the feasibility of MSP and PLRA. Both MSP and PLRWD are essential diagnostic parameters for preoperative planning and better surgical outcomes.
Introduction
Maxillary sinus (MS) diseases are mainly treated by middle meatal antrostomy. However, this approach has limited access for lesions in the anterior and lower sinus walls. Simultaneous middle and inferior meatal antrostomies enable access to the MS; however, this may prove insufficient to access the prelacrimal recess (PLR). 1
To overcome these limitations, Zhou et al2,3 proposed an endoscopic prelacrimal recess approach (PLRA) that enables easy removal of lesions in the PLR in MS under endoscopic guidance. Before surgery, sinus computed tomography (CT) can determine the feasibility of PLRA, which, in turn, can be evaluated by prelacrimal recess window distance (PLRWD), for a successful PLRA.4,5
Simmen et al 4 reported differences in the surgical feasibility of PLRWD. The distance is divided into 3 types: I (<3 mm), II (3-7 mm), and III (>7 mm); type III is the most favorable for PLRA without the need to remove bone, allowing access to the PLR using a chisel. Type II requires temporary lacrimal duct dislocation, whereas type I requires significant bone removal and dislocation of the lacrimal duct, proving to be the least feasible for PLRA.
However, correlating maxillary sinus pneumatization (MSP) to the ease of PLRA could be significantly difficult as MSP varies from one person to another. The authors aimed to define the correlation between MSP and PLRWD, a previously defined anatomic factor that is predictive of PLRA ease.
Materials and Methods
Materials
We analyzed 637 paranasal sinus (PNS) CT scans that were performed at our university hospital between January 2019 and December 2020. Patients aged 18 to 70 years were included in this study. We excluded patients with MS lesions, nasolacrimal duct disease, history of sinus and nasolacrimal duct surgeries, or facial fracture history. This study was approved by the Institutional Review Board of Wonkwang University Hospital (2022-03-010).
PNS CT Analysis
PNS CT was conducted as follows: Axial planes with a thickness of 0.5 mm were obtained using Aquilion ONE Genesis TSX-305A (Canon Toshiba, Otawara-shi, Japan), and coronal and sagittal planes with a thickness of 2 mm were obtained using Display-Consol (Canon Toshiba, Otawara-shi, Japan) for reconstruction.
As previously described by Simmen et al, a 3-dimensional cursor was applied to the corresponding part of the axial plane image after confirming anterior insertion of the inferior turbinate into the frontal process of the maxilla (Figure 1). A tangential line through the posterior end of the anterior wall of the MS and another line parallel to the anterior surface of the lacrimal duct were drawn on the axial plane image of the PNS CT. Then, the distance between 2 lines was measured, which was classified as type I (<3 mm), type II (3-7 mm), and type III (>7 mm) (Figure 1). 4 Next, 3 groups were established using the previously described MSP classification suggested by Kim et al. 6 To put it simply, based on the nasal floor in coronal image, when MSP did not reach the nasal floor, it was classified as grade I, grade II when MSP reached the nasal floor, and grade III when MS was pneumatized below the nasal floor (Figure 2). With reference to the nasal floor, the MSP distance was 0, positive (+), and negative (−) if the lower end of the MS was located on the nasal floor, below the nasal floor, or above the nasal floor, respectively (Figure 2).
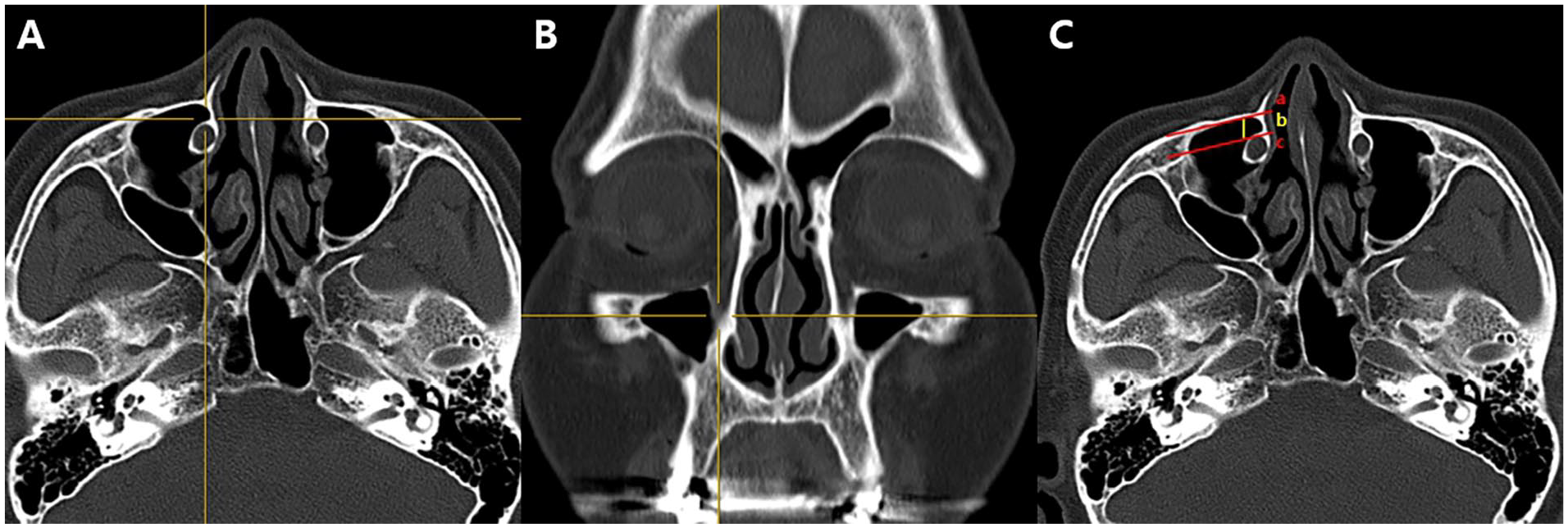
(A) Axial and (B) coronal sinus computed tomography (CT) images show the anterior insertion of the inferior turbinate into the frontal process of the maxilla using a 3-dimensional cursor. (C) Axial sinus CT image shows measurement of the distance (b) between a tangential line through the posterior surface of the anterior wall of the maxillary sinus (a) and a parallel line through the anterior wall of the lacrimal duct (c).
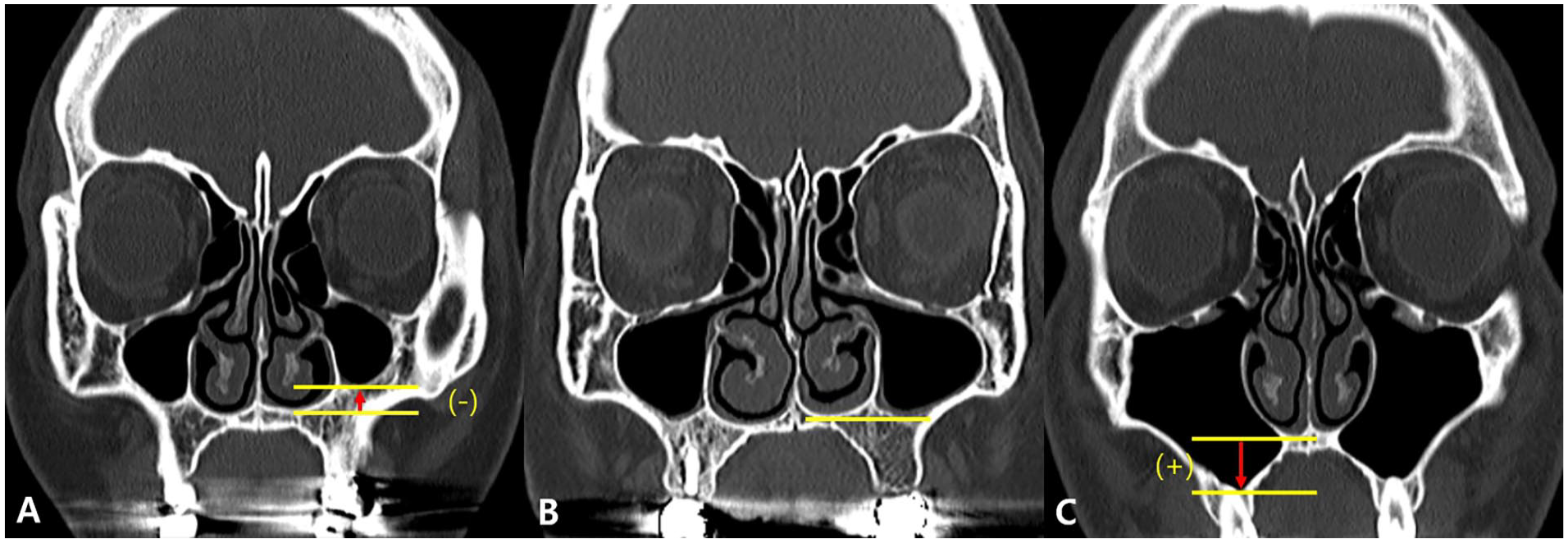
Computed tomography (CT) findings of maxillary sinus pneumatization (MSP). (A) Grade I shows MSP limited above the nasal floor level. (B) Grade II shows MSP limited to the nasal floor level. (C) Grade III shows MSP extended below the nasal floor level. The distance (degree of MSP) is measured by indicating positive (+) value (arrow) when the lower end of the maxillary sinus is located below the nasal floor and negative (−) value (arrow) when located above.
Statistical Analysis
SPSS version 24.0 program (IBM Corp., Armonk, NY, USA) was used for statistical analyses in this study. Analysis of variance (ANOVA) and Duncan’s post hoc tests were conducted to analyze the mean PLRWD by MSP grade. Pearson’s correlation analysis was conducted to determine the correlation between the PLRWD and MSP distance. Statistical significance was set at P < .05.
Results
Demographic Characteristics and Distribution of PLRA Types I, II, and III
We analyzed 637 PNS CT scans that were performed at our university hospital between January 2019 and December 2020. Patients aged 18 to 70 years (517 PNS CT scans) were included in this study. Of the 517 PNS CT scans, we excluded patients with MS lesions (158 cases), nasolacrimal duct disease (13 cases), history of sinus (78 cases) and nasolacrimal duct surgeries (8 cases), or facial fracture history (7 cases), following which 253 PNS CT scans were included. A total of 506 bilateral sides of each patient were included in the analysis. Of the 253 patients included in the analysis, 149 were males and 104 were females. The mean age was 49.6 ± 15.19 years for men and 51.7 ± 15.2 for women, with no significant difference between men and women (P = .637). The distributions of PLRA types I, II, and III on the left and right sides were as follows: Types I, II, and III were observed on the right side in 60 (23.7%), 130 (51.4%), and 63 (24.9%) patients, respectively. Types I, II, and III were observed on the left side in 55 (21.7%), 147 (58.1%), and 51 patients (20.2%), respectively. Types I, II, and III were observed in 115 (22.7%), 277 (54.7%), and 114 (22.5%) patients, respectively (Table 1).
Demographics of the Study Group.
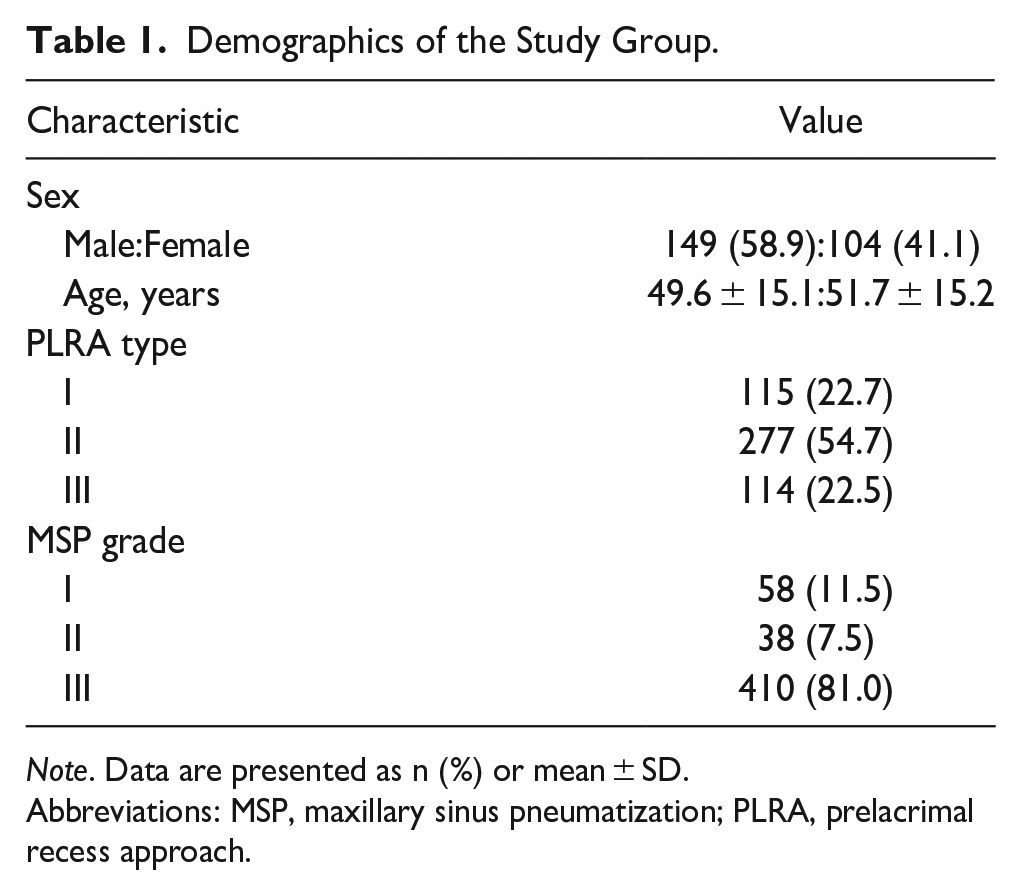
Note. Data are presented as n (%) or mean ± SD.
Abbreviations: MSP, maxillary sinus pneumatization; PLRA, prelacrimal recess approach.
Distribution of MSP Grade
The distribution of the MSP grades on the left and right sides is as follows: Grades I, II, and III were observed on the right side in 32 (12.6%), 18 (7.1%), and 203 (80.2%) participants, respectively. Grades I, II, and III lesions were observed on the left side in 26 (10.3%), 20(7.9%), and 207 (81.8%) patients, respectively. Grades I, II, and III were observed in 58 (11.5%), 38 (7.5%), and 410 (81.0%) participants, respectively (Table 1).
Analysis of MSP Grade and PLRWD
The mean PLRWD was 2.35 ± 2.41 mm for grade I, 3.37 ± 2.46 mm for grade II, and 5.55 ± 2.54 mm for grade III, showing significant differences among the grades I, II, and III (P < .001) (Table 2). Post hoc analysis showed significant differences in the mean PLRWD among grades I, II, and III.
PLRWD According to MSP Grade.
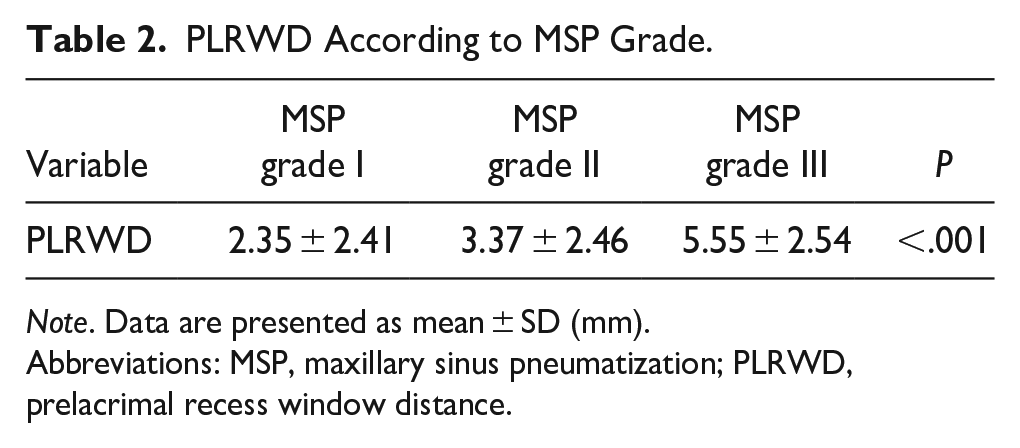
Note. Data are presented as mean ± SD (mm).
Abbreviations: MSP, maxillary sinus pneumatization; PLRWD, prelacrimal recess window distance.
Correlation Between PLRWD and MSP Distance
The PLRWD and MSP distances were positively correlated (r = .507, P < .001) (Figure 3). The minimum and maximum PLRWD values were 0 and 12.94 mm, respectively. The minimum and maximum values of MSP distance were −12.86 and 16.93 mm, respectively.
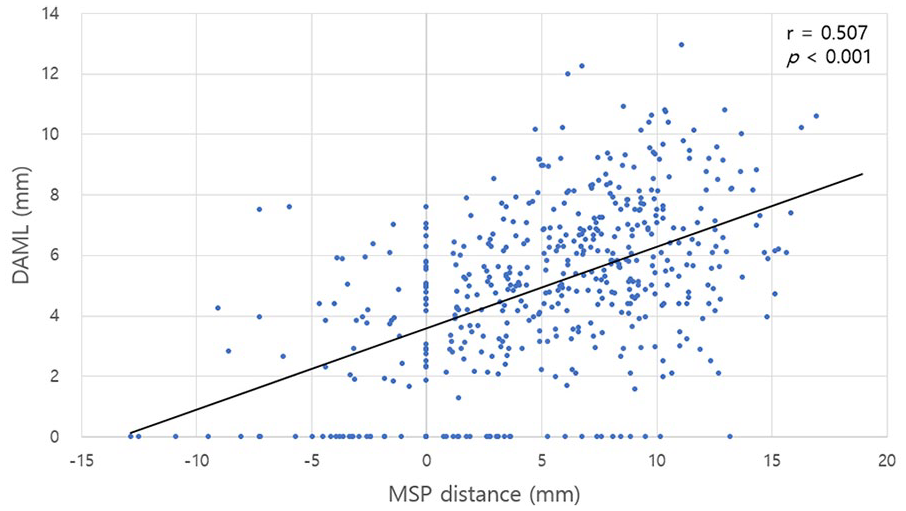
Correlation between the MSP and PLRWD.
Discussion
In addition to the study by Simmen et al, there have been other reports on the ease of using PLRA. In Westerners, type I accounts for approximately 30%, whereas in Asians, it is slightly less than 10%; therefore, there is an anatomical difference between them.1,4,7,8 These results are expected to be easier to apply in Asians than in Westerners. In this study, type I was 22.7%, which was lower than that in previous studies on Westerners but higher than that in previous studies on Asians.
According to the MS classification proposed by Sirikçi et al, type I hypoplasia is characterized by a normal coronoid process, open infundibulum, and mild MS hypoplasia. Type II is characterized by the hypoplasia of the coronoid process, a narrow infundibulum, and marked MS hypoplasia, whereas type III is characterized by aplasia of the coronoid process and severe hypoplasia of the MS. 9 Duman et al 10 measured PLRWD in an MS hypoplasia group of 78 sides and a control group of 70 sides. The PLRWD was 3.11 ± 1.49 mm in the MS hypoplasia group and 4.77 ± 1.76 mm in the control group. 10
We investigated the correlation between the PLRWD and MSP distance by classifying the PLRWD into PLRA types I, II, and III. In our participant population, the types II and III MS classifications by Sirikçi et al were not observed. Herein, 3 groups were established using the previously described MSP classification suggested by Kim et al. 6 MSP grade for both sides was I in 58 sides (11.5%), II in 38 sides (7.5%), and III in 410 sides (81.0%). Grade III showed the longest mean PLRWD, followed by grades II and I, with significant differences between the 3 groups. In addition, with reference to the nasal floor, the MSP distance was either 0, positive (+), or negative (−) if the lower end of the MS was located at the nasal floor, below the nasal floor, or above the nasal floor, respectively (minimum value: −12.86 mm, maximum value: 16.93 mm). There was a clear positive linear correlation between MSP distance and PLRWD, with r = .507. These results show a correlation between the level of MSP and the feasibility of PLRA. Grade I is not feasible for PLRA, which requires the dislocation of the lacrimal duct and significant removal of the surrounding bone to access the PLR. Access to the PLR may be affected by the level of MSP in each individual, and preoperative CT may help in planning an adequate approach for sinus surgery.
The strength of this study was its relatively large sample size. A total of 253 participants with 506 sides were included in the analysis and divided into 3 groups according to the MSP grading. Our findings showed significant differences in the PLRWD according to the MSP grade. In addition, in light of our findings, we observed a clear correlation between the MSP and PLRWD with reference to the nasal floor. However, the control group comprised participants without MS lesions and did not include patients with inverted papillomas. Thus, further studies including such patient groups should be conducted in the future.
Conclusion
This study demonstrated a correlation between MSP levels and PLRA feasibility. The better the MS pneumatization, the easier it is to access the PLR. Both MSP and PLRWD are helpful for optimal preoperative planning and better surgical outcomes.
Footnotes
Authors’ Note
This study was supported by Wonkwang University in 2023.
Data Availability
All authors had full access to all data in the study and take responsibility for the integrity of the data and accuracy of the data analysis. These data are available to anyone upon request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The authors confirm that we have read the journal’s guidelines on issues involved in ethical publication and affirm that this report is consistent with these guidelines.