
Abstract
Adult esophageal duplication (ED) is a rare congenital anomaly that is rarely encountered in clinical practice. There have been only a few reported cases of adult tubular esophageal duplication. A patient presented with symptoms of odynophagia and dysphagia. Upon examination, gastroscopy and X-ray contrast imaging revealed the formation of a fistula in the upper esophagus that connected to a sinus tract running along the esophagus. After managing the initial infection, an open surgery was performed. The esophageal tubular duplication was removed and the defect was reconstructed using a supraclavicular artery island (SAI) flap. The post-operative recovery was uneventful and the patient’s odynophagia and dysphagia were relieved. In conclusion, ED can be effectively diagnosed through esophagogram and gastroscopy. Surgical excision is currently the preferred treatment option, and the use of the SAI flap technique shows great promise in reconstructing the esophageal defect after surgery.
Keywords
Introduction
Esophageal Duplication (ED) is a rare congenital abnormality with an estimated occurrence rate of 0.0122%. 1 While ED is primarily diagnosed in early childhood, adult cases are rarely seen in clinical settings. 2 Only a few cases of adult tubular esophageal duplication have been reported.3 –5 Symptoms of ED include odynophagia, dysphagia, chest pain, or in some cases, pneumonia. Esophagogram or gastroscopy are the preferred diagnostic tests, and open surgery or endoscopic surgery are the recommended treatment options.4 –7 The supraclavicular artery island (SAI) flap has been used in various defect reconstruction surgeries since its first reporting in 1979 and is widely considered to be an convenient and reliable technique.8 –10 The SAI flap is a preferred option due to its ease of harvest and good success rate in surgical reconstruction.
In this case, we report an adult patient with a severe esophageal stricture caused by tubular ED. We successfully removed the duplicated portion of the esophagus and reconstructed it using the SAI flap. The surgery was successful, resulting in significant relief of the patient’s symptoms.
Case Presentation
History and Physical Examination: A 29-year-old female patient was admitted to our department with symptoms of odynophagia and dysphagia. The symptoms had begun to develop 5 days prior to her visit and included progressive odynophagia, dysphagia, and hoarseness. Upon initial admission to a local hospital, a CT scan revealed paraesophageal and superior mediastinal abscesses. Despite initial treatment with antibiotics, the infection persisted and the patient was referred to our hospital. On admission, laryngoscopy revealed a fixed right vocal cord. Neck contrast-CT scan showed the presence of a paraesophageal abscess (Figure S1). Gastroscopy revealed an esophageal fistula located 16 cm from the incisor. Both the esophagus and the adjacent fistula had a diameter around 0.5 cm (Figure S2). While esophagogram showed a mediastinal fistula to the right side of the cervical esophagus (Figure 1). Bronchoscopy did not reveal any unusual findings. An esophageal X-ray esophagogram showed a fistula in the right cervical esophagus at the level of the 7th cervical vertebra and extending down to the 4th thoracic vertebra level. The sinus tract compressed the adjacent esophagus and caused a stricture.
The patient was first treated with antibiotics to control the infection. Open surgery was performed three days after admission. During the surgery, an esophageal fistula in the right side of the cervical esophagus was observed, connecting to a sinus tract 8 centimeters in length. The lower end of the sinus tract extended down the length of the esophagus and adhered tightly to surrounding tissue, ending in a blind pouch containing only necrotic material. The sinus tract and septal wall were excised and the esophagus was reconstructed using a right SAI flap (Figure 2). The post-operative pathology confirmed the diagnosis of ED (Figure S3). During the post-operative recovery period, the patient’s hoarseness persisted. A repeat laryngoscopy showed a fixed right vocal cord, consistent with the pre-operative examination. The patient was given a nasogastric tube for enteral feeding on the first post-operative day and was discharged seven days after the surgery. Approximately one month after the surgery, the patient began an oral liquid diet, gradually transitioning to a low-fiber diet. The nasogastric tube was removed around two months after the surgery, and a contrast-CT scan showed a viable SAI flap and a patent cervical esophagus (Figure S4). During the four-month follow-up, the patient demonstrated good swallowing function, and their odynophagia and dysphagia were relieved, although hoarseness was only partially relieved. Access the fistula from the right pyriform fossa. Carefully dissect and safeguard the recurrent laryngeal nerve. Completely remove the sinus tract and the esophageal septum. Utilize a 9 cm × 5 cm superior array flap with a thickness of 2 cm for reconstruction of the esophagus. The incisions in the neck and shoulder were observed to have healed properly during the 2-month follow-up examination.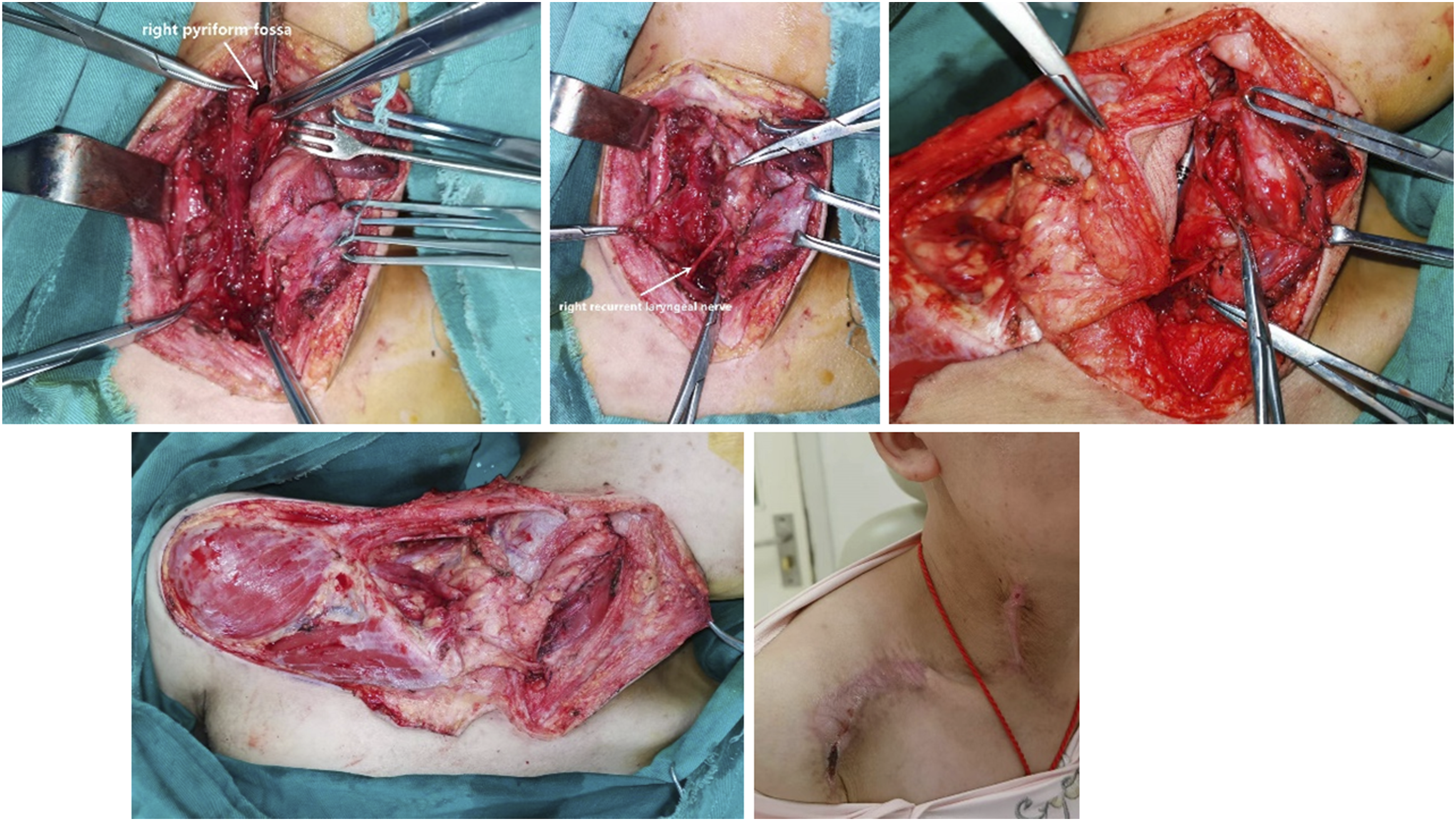
Discussion
Esophageal duplication (ED) is a congenital gastrointestinal tract malformation that accounts for 20% of all such malformations. 11 It is caused by incomplete vacuolization during embryogenesis’s fifth to eighth week and migration into the esophageal wall. ED is commonly found in the thoracic or abdominal esophagus and is often accompanied by esophageal stricture, tracheoesophageal fistula, or even esophageal cancer. 5 There are 3 main types of ED: cystic, diverticular, and tubular. Cystic ED is the most common type, while tubular ED accounts for about 23% of all cases. 5 Tubular ED is typically connected to the esophagus at one or both ends and shares a part of the esophageal wall with the esophagus. The symptoms of ED patients vary depending on the size, location, and infectious status of the ED. Many cases are identified in childhood due to dysphagia or recurrent pulmonary infections, while some patients may remain asymptomatic until adulthood. The diagnostic tests of choice are neck contrast-CT scan, esophagogram, and gastroscopy. Gastroscopy can directly identify and locate the opening of the fistula on the esophagus, while esophagogram can reveal the shape of the esophagus and ED and their relative positions. Differential diagnosis should include third and fourth branchial cleft abnormalities, which typically occur in a similar location to ED, although they don’t usually share the septal wall with the esophagus and are not typically connected to the esophagus.
The preferred treatment for ED is open surgical excision; 12 however, it is known to be more traumatic and have higher post-operative complications. Some researchers advocate for endoscopic surgery, which has the benefits of reduced trauma, quicker recovery time, and fewer complications. 5 The endoscopic procedure involves opening the septum between the esophagus and the duplication, expanding the esophagus. 7 In this case, open surgery was chosen with subsequent reconstruction using an SAI flap for several reasons: (1) The sinus tract was 8 cm in length; (2) The fistula was located at the entrance of the esophagus and caused stricture; (3) The infected sinus tract caused adhesion and fibrous scarring in the septal wall, resulting in a large esophageal defect after excision; and (4) The SAI flap was relatively easier to harvest and had a perfect skin color match for the cervical region. Although the surgery was successful in excising the ED without damaging the surrounding tissue, the patient continued to experience hoarseness after the procedure. This was likely due to infection affecting the recurrent laryngeal nerve, as evidenced by a fixed right vocal cord in the pre-operative laryngoscopy. However, the hoarseness partially improved during the 4-month follow-up period.
In conclusion, tubular esophageal duplication in adults is an uncommon congenital condition. If a patient presents with symptoms of an acute upper digestive or respiratory infection, along with abnormal esophagogram and gastroscopy findings such as a fistula, sinus tract, or cystic structure, ED should be considered in the differential diagnosis. The preferred treatment is surgical excision. Pre-operative planning of esophageal stricture management and post-operative defect reconstruction is crucial, and the use of the SAI flap technique has great potential for reconstruction.
Supplemental Material
Supplemental Material - Supraclavicular Artery Island flap for Post-operative Esophageal Defect Reconstruction in a Tubular Esophageal Duplication Adult
Supplemental Material for Supraclavicular Artery Island flap for Post-operative Esophageal Defect Reconstruction in a Tubular Esophageal Duplication Adult by Xin Yang, Zheng Jiang, Jun Liu, and Fei Chen in Ear, Nose & Throat Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Written informed consent for publication of this paper was obtained from West China Hospital. Written informed consent was obtained from the patient.
Data Availability
All the available data is included in the article and the supplementary files.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.