
Abstract
Dermatofibrosarcoma protuberans (DFSP) is a locally aggressive tumor with high rate of local recurrence but low metastatic potential. Its high-grade fibrosarcomatous variant and occurrence on the head and neck are rare findings associated with increased morbidity and mortality. The most significant prognostic feature of DFSP is obtaining tumor free surgical margins. As such, accurate recognition and proper management of this uncommon and locally aggressive malignancy is especially crucial in head and neck surgery.
Dermatofibrosarcoma Protuberans of the Face
A 62-year-old male presented with a painless facial mass of over 24 months duration. The mass originally developed as an asymptomatic lump on the left lateral aspect of the face which had increased steadily in size and was now pruritic (Figure 1A). Examination revealed what appeared to be two discrete lesions in the area of the left parotid gland: a 3 × 3 cm firm mass adherent to the overlying skin at the angle of the mandible, and a 2 cm flat, multinodular lesion directly anterior to the first. The patient’s facial nerve function was intact and there was no palpable cervical lymphadenopathy. Based on the patient’s presentation and exam, a benign vs. malignant neoplasm was suspected, rather than chronic infection, granulomatous disease, subcutaneous cystic lesion, or sialolithiasis, and the appropriate work-up was initiated. A-C Surgical management of dermatofibrosarcoma protuberance of the face. In the preoperative setting (A), the tumor is seen on the lateral aspect of the face as a 3 × 3 cm mass at the angle of the left mandible and a 2 cm flat, multinodular lesion directly anterior to the first. Surgical management involved wide tumor resection using 2.5 cm margins, superficial parotidectomy, and left anterolateral thigh free flap reconstruction (B, C).
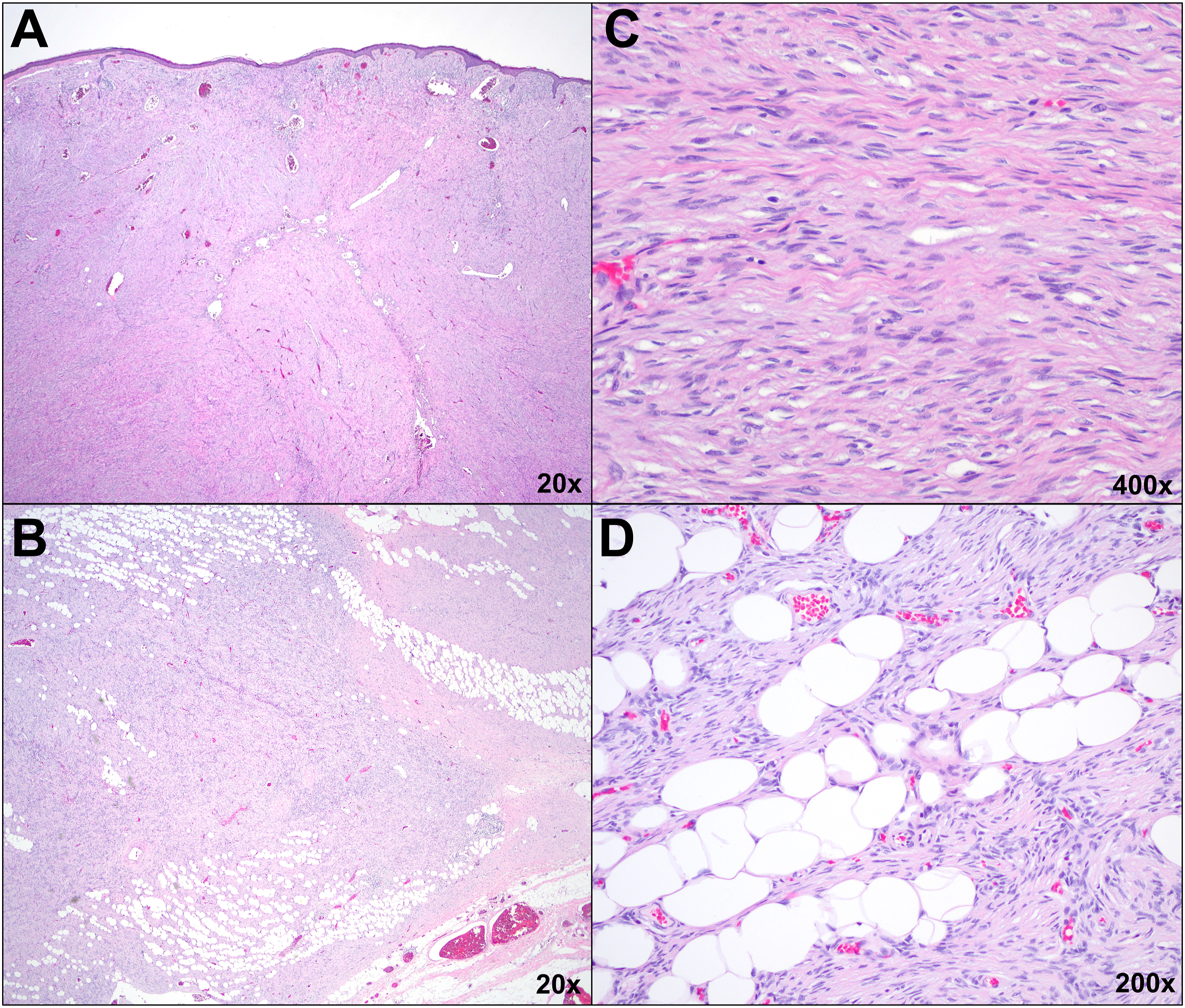
Computed tomography (CT) with IV contrast of the neck showed three enhancing masses (2.4 cm, 15 mm, and 8 mm) within the subcutaneous tissues immediately superficial to the left parotid gland without parotid involvement (Figure 2A-D). Initial sampling of the 2.4 cm mass revealed a spindle cell neoplasm with an immunohistochemical profile (diffuse positivity with CD34, focal positivity with Factor XIIIa, and no reactivity for S-100, CD45, actin, desmin, AE1/AE3, SOX-10, Beta-catenin, STAT6, and EMA) consistent with dermatofibrosarcoma protuberans (DFSP). Rearrangement of the platelet-derived growth factor β (PDGFβ) gene was subsequently identified using fluorescence in situ hybridization, further supporting a diagnosis of DFSP. The patient underwent wide surgical resection of the tumor with 2.5 cm margins, superficial parotidectomy, and left anterolateral thigh free flap reconstruction (Figure 1B-C). Final pathology showed high-grade DFSP with fibrosarcomatous changes with tumor present at multiple margins, including a deep margin corresponding to the facial nerve (Figure 3). The patient recovered well from surgery and completed adjuvant radiation therapy. A-D Contrast-enhanced CT soft tissue of the neck showing three enhancing masses (2.4 cm, 15 mm, and 8 mm) within the subcutaneous tissues immediately superficial to the left parotid gland without parotid involvement in the axial (A, B) and coronal (C, D) planes. CT indicates computed tomography. A-D Histologic examination utilizing routine hematoxylin and eosin staining. On low power (A), the tumor consumes the dermis, completely replacing normal dermal architecture and effacing the overlying epidermis. The tumor infiltrates the subcutis along fibrous septa and amongst fat lobules (B). Higher power examination (C) reveals the tumor is comprised of spindle shaped cells with eosinophilic cytoplasm and monomorphic, elongated nuclei. Tumor cells of similar morphology interdigitate between fat lobules creating a “honeycomb” pattern (D).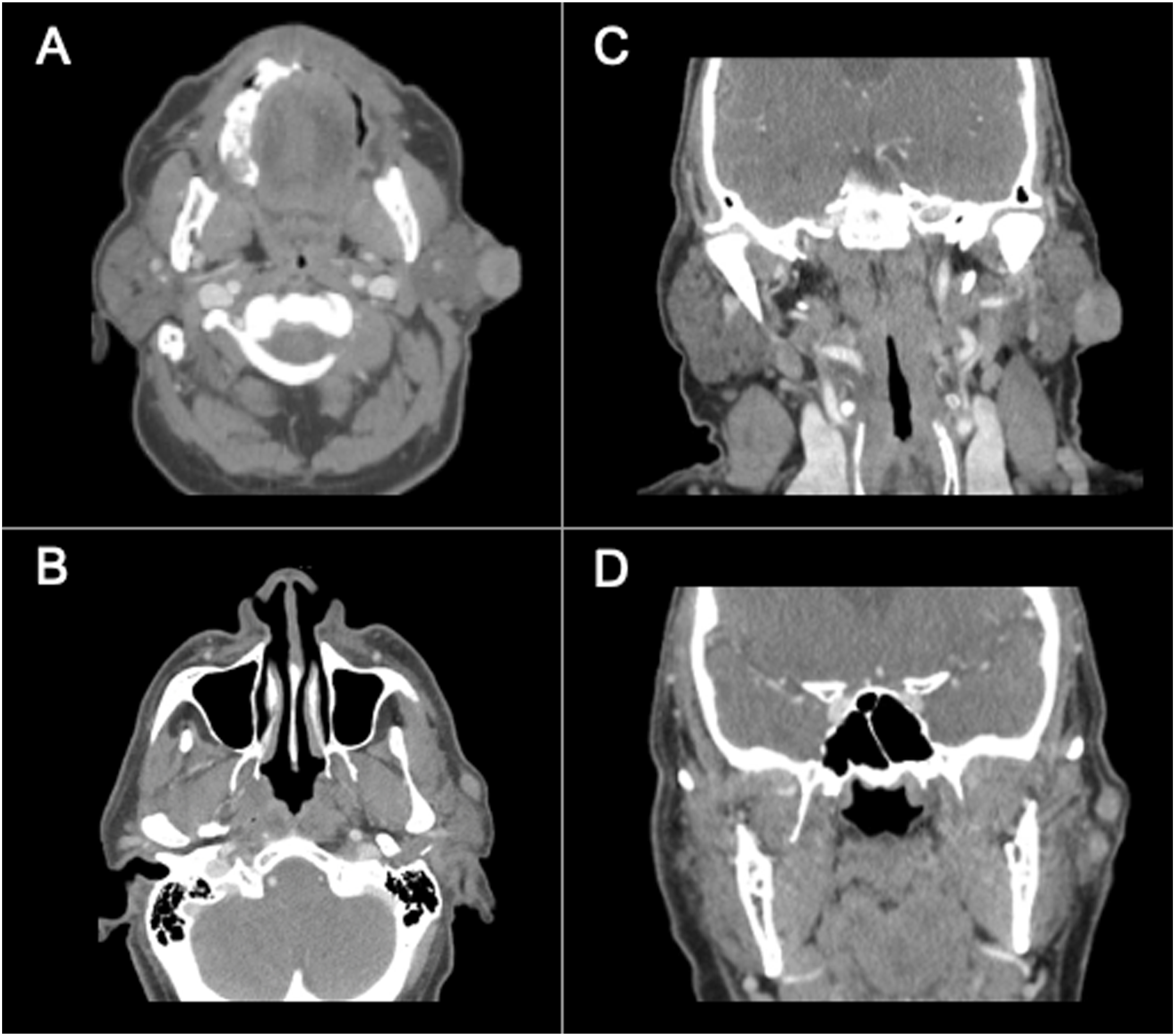
Here we document a rare case of dermatofibrosarcoma protuberans with fibrosarcomatous changes (FS-DFSP) of the face. DFSP is a locally aggressive and highly recurrent tumor with low metastatic potential. It has an incidence rate of less than five cases per million people per year, yet makes up 6% of all soft tissue sarcomas, making it the most common type of deep dermal neoplasm.1,2 However, DFSP makes up less than 1.4% of all head and neck soft tissue sarcomas, and only 5% to 15% of DFSP cases display fibrosarcomatous changes. 3
The presence of fibrosarcomatous changes and occurrence on the head and neck are negative prognostic features. A recent study on DFSP of the face found that patients with FS-DSFP had higher recurrence (83.3%) and metastasis (33.3%) rates compared to those with usual DFSP (59.1% and 0%, respectively). 4 Surgical excision with 2cm to 4cm margins is the mainstay treatment for DFSP. 1 Microscopically, DFSP is characterized by a proliferation of spindle shaped cells arranged in a storiform or whorled fashion, often interdigitating along fibrous septa, adipocytes (causing a “honeycomb” pattern), and other structures, making the periphery of the tumor difficult to identify.3,5 This is believed to be the reason for the high recurrence rates observed in DFSP despite clinically clear surgical margins. As such, Mohs micrographic surgery is the preferred modality, especially with involvement of the head and neck, where the evaluation of the entire surgical margin is possible while best preserving the structure and function of facial anatomy.1,3
Chemotherapy is ineffective at treating DFSP and radiotherapy is not recommended as primary treatment. 6 However, DFSP is a radioresponsive cancer and adjuvant radiotherapy can improve local control but not overall survival in these patients. While there are no consensus guidelines on adjuvant radiotherapy in DFPS, it is typically reserved for patients with an increased risk of recurrence.3,6 Targeted treatment with imatinib may improve outcomes for patients with locally advanced or metastatic disease, however, benefit has not been demonstrated for patients with FS-DFSP. 5 Overall, the prognosis of DFSP is good, with a reported 10-year survival of 99.1%. 7 However, occurrence in the head and neck is associated with a 1.4 times increased risk for mortality. 7 Because positive surgical margins increase morbidity and may contribute to the increased mortality risk in patients with DFSP of the head and neck, head and neck surgeons should aim to secure histologically confirmed tumor free tissue margins, or when possible, incorporate Mohs micrographic surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.