
Abstract
Thyroglossal duct cysts (TDCs) are generally single cyst, multiple TDCs are rare. We describe a case of multiple TDCs, discuss its characteristic features and management, and provide a review of the literature, to improve clinical diagnosis and treatment. We report an extremely rare case of multiple TDCs containing five cysts, together with a review of the relevant English medical literature. To the best of our knowledge, this is the first reported case of TDCs containing more than three cysts in the anterior cervical region. The five cysts were completely excised in a Sistrunk operation. Histological examination of the cystic lesions revealed TDCs. The patient recovered well and no recurrence was found during the 6-year of follow-up. Multiple TDCs are extremely rare, and may be misdiagnosed as a single cyst. Clinicians should be aware of the possibility of multiple thyroglossal duct cysts. Adequate preoperative radiological examinations should be performed, and careful interpretation of the CT or MRI scans is important to diagnosis and surgery.
Introduction
Thyroglossal duct cyst (TDC) is a common congenital disease in the neck which can occur in any part of the midline of the neck between the foramen cecum of the tongue and the suprasternal notch. It usually presents as a compressible mass near the hyoid in the middle of the neck. Thyroglossal duct cysts (TDCs) are generally single cyst, multiple cysts are rare. There have been few reports of multiple TDCs, only ten cases have been reported in the English medical literature.1 –10
We report an extremely rare case of multiple TDCs containing five cysts, together with a review of the relevant English medical literature. To the best of our knowledge, this is the first reported case of TDCs containing more than three cysts in the anterior cervical region.
Clinical Report
A 55-year-old male presented to the Department of Otolaryngology, The First Affiliated Hospital, College of Medicine, Zhejiang University (Hangzhou, China), with a 4-month history of cervical mass. There was no significant change in mass size during the course of the disease. The patient exhibited no neck pain, pharyngalgia, hoarseness, dyspnea, dysphagia, or fever. He was a nonsmoker and nondrinker. His medical history was otherwise unremarkable.
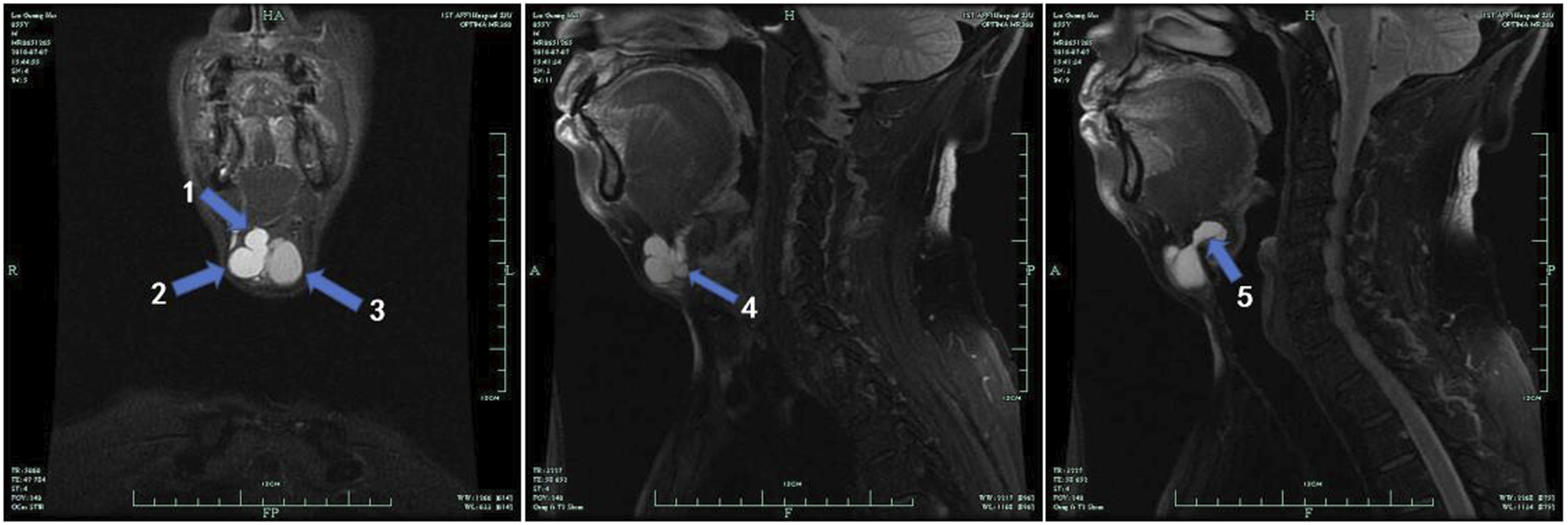
Upon cervical palpation, a soft mass approximately 5.0 × 4.0 cm was found at the level of thyroid cartilage and hyoid bon, and it moved up-and-down when he swallowed. Physical examination revealed no abnormalities within the nasopharynx, tongue, hypopharynx, laryngeal and cervical lymph nodes. Ultrasound confirmed multiple cystic masses in the region of thyroid cartilage and hyoid bon (Figure 1). Magnetic resonance imaging (MRI) of the neck revealed that five well-defined cystic lesions were adjacently located in the midline from the thyroid cartilage to the foramen cecum linguae. These cysts were separated from each other and seemed to be connected to the hyoid bone (Figure 2). The appearance of the thyroid gland was normal. According to the clinical presentation and MRI findings, we made a preliminary diagnosis of multiple thyroglossal duct cysts, and Sistrunk operation was planned. Cervical ultrasound: multiple cystic masses in the region of thyroid cartilage and hyoid bon. MRI of the neck revealed that five well-defined cystic lesions were adjacently located in the midline from the thyroid cartilage to the foramen cecum linguae. These cysts were separated from each other and seemed to be connected to the hyoid bone (T2-weighted image).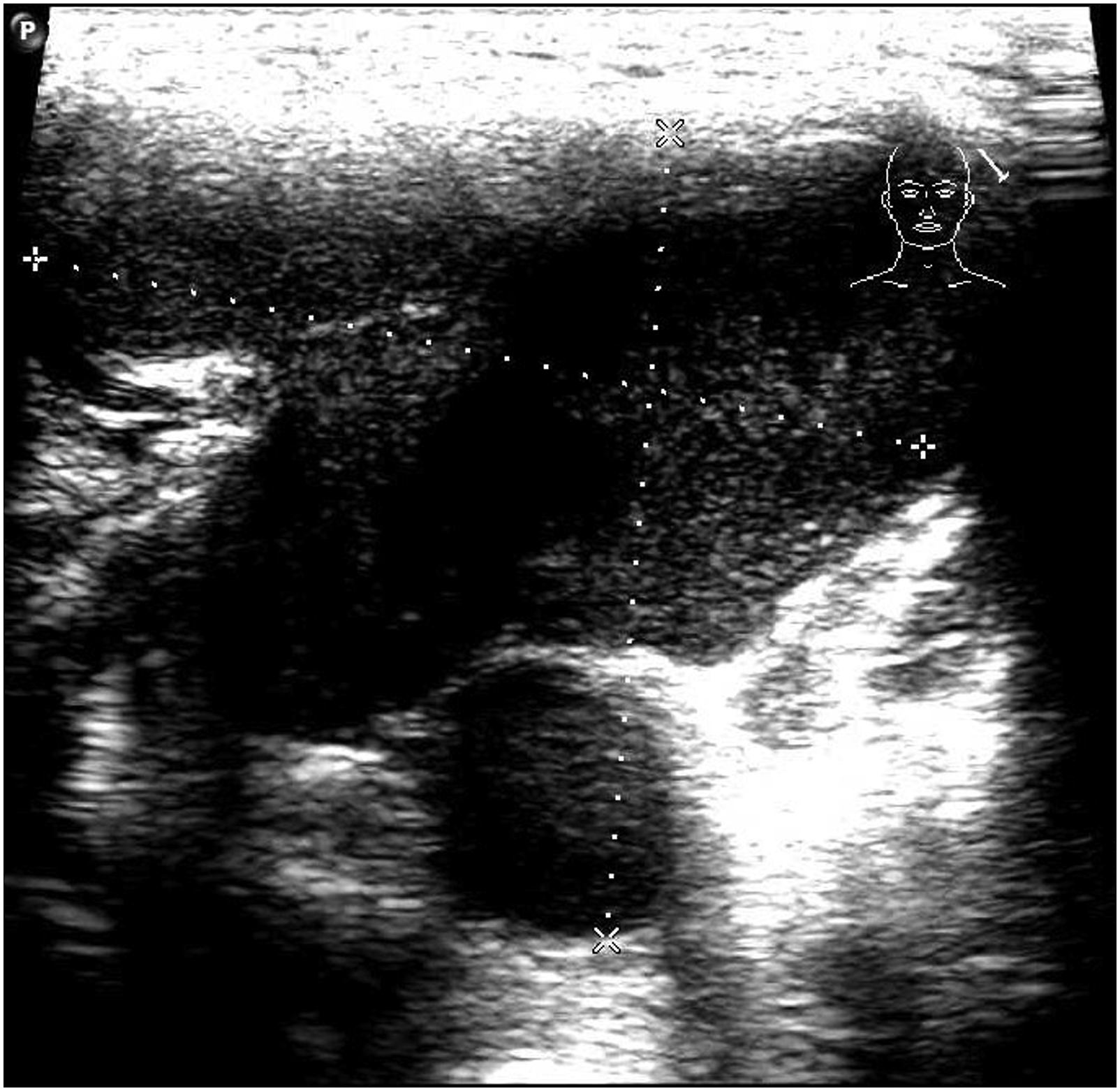
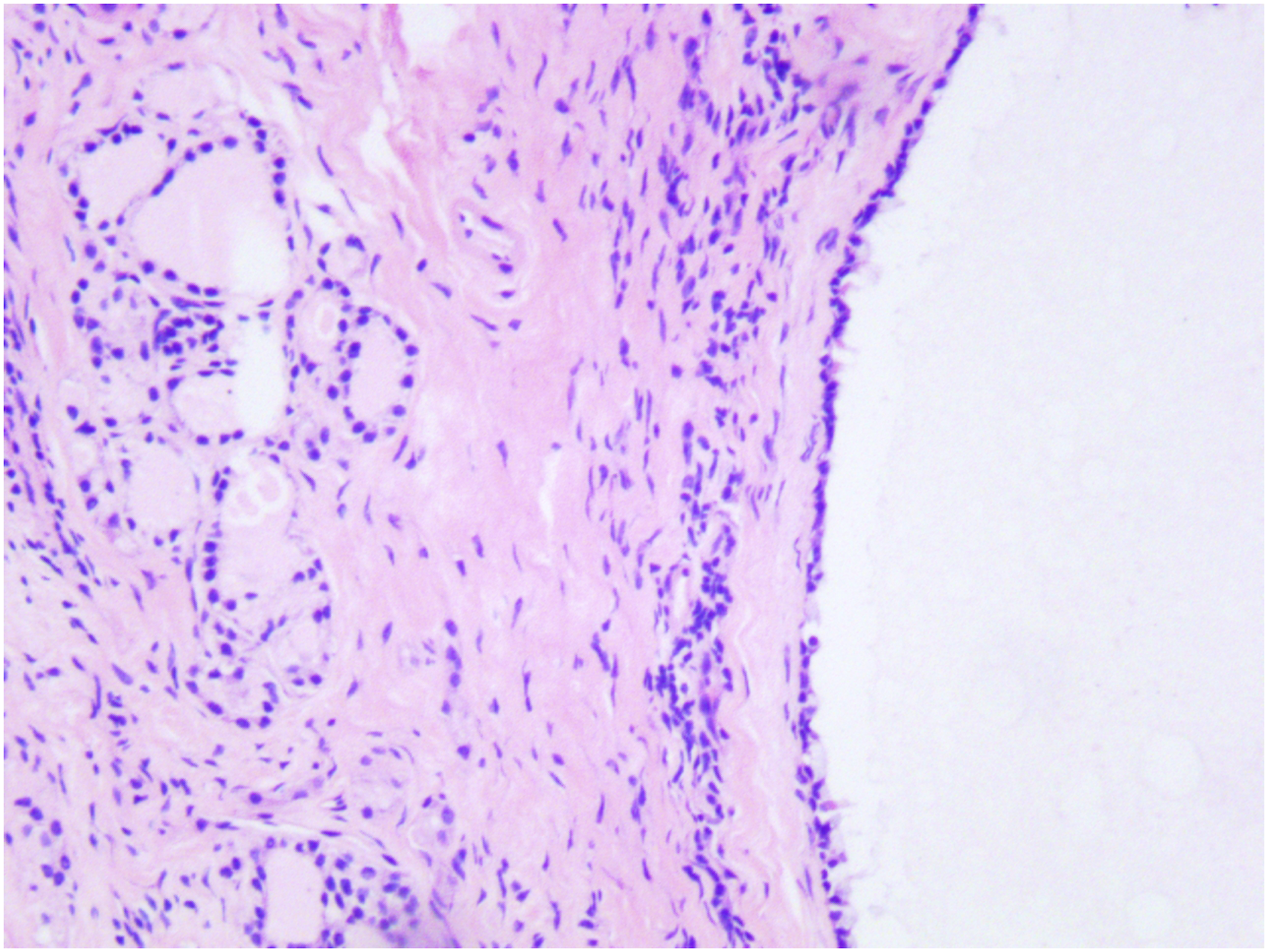
The patient underwent a transcervical approach under general anesthesia. A transverse skin incision was made at the level of the hyoid bone. At surgery, three cystic lesions between 2 and 3 cm in size anterior to the hyoid, one cyst measured approximately 1 cm posterior to the hyoid, and another cyst measured approximately 2 cm above the hyoid, which were all connected to the midline of the hyoid bone (Figure 3). The five cysts were completely excised in a Sistrunk operation. Histological examination of the cystic lesions revealed TDCs: the fibrous wall of the cyst was lined with pavement epithelium and colloid-containing thyroid acini (Figure 4), and no evidence of malignancy was detected. The five cysts were completely excised in a Sistrunk operation. Microscopic examination showed the fibrous wall of the cyst was lined with pavement epithelium and colloid-containing thyroid acini (HE × 100).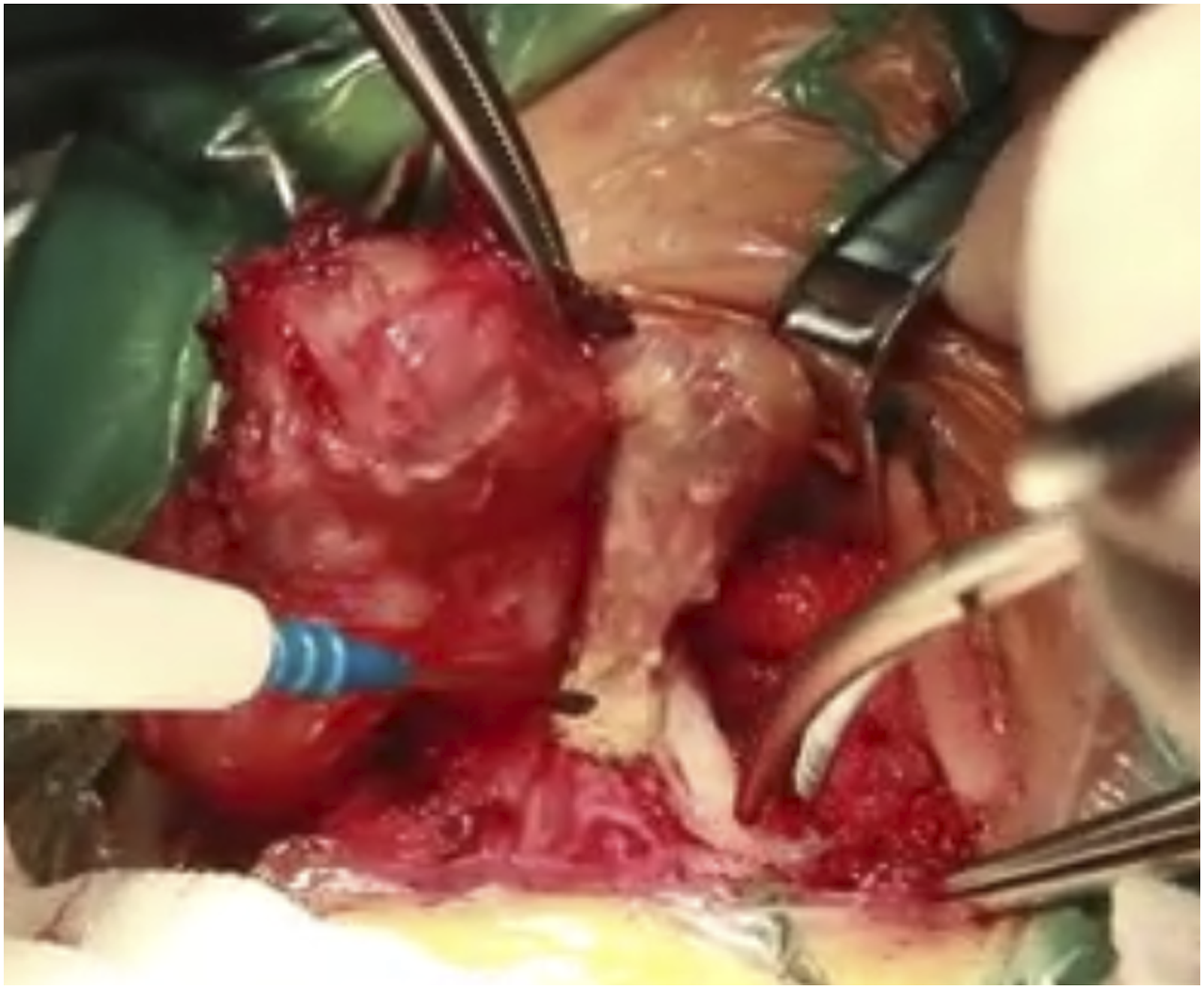
The patient had an uneventful postoperative recovery and was discharged on the third postoperative day. He remains asymptomatic, and there was no recurrence during the 6-year of follow-up. No recurrence during the 6-year of follow-up.
Discussion
We reviewed the English medical literature in the MEDLINE database, using the search terms “double” OR “multiple” OR “Polycystic” AND “thyroglossal duct cyst.”
Multiple thyroglossal duct cysts reported in the English medical literature
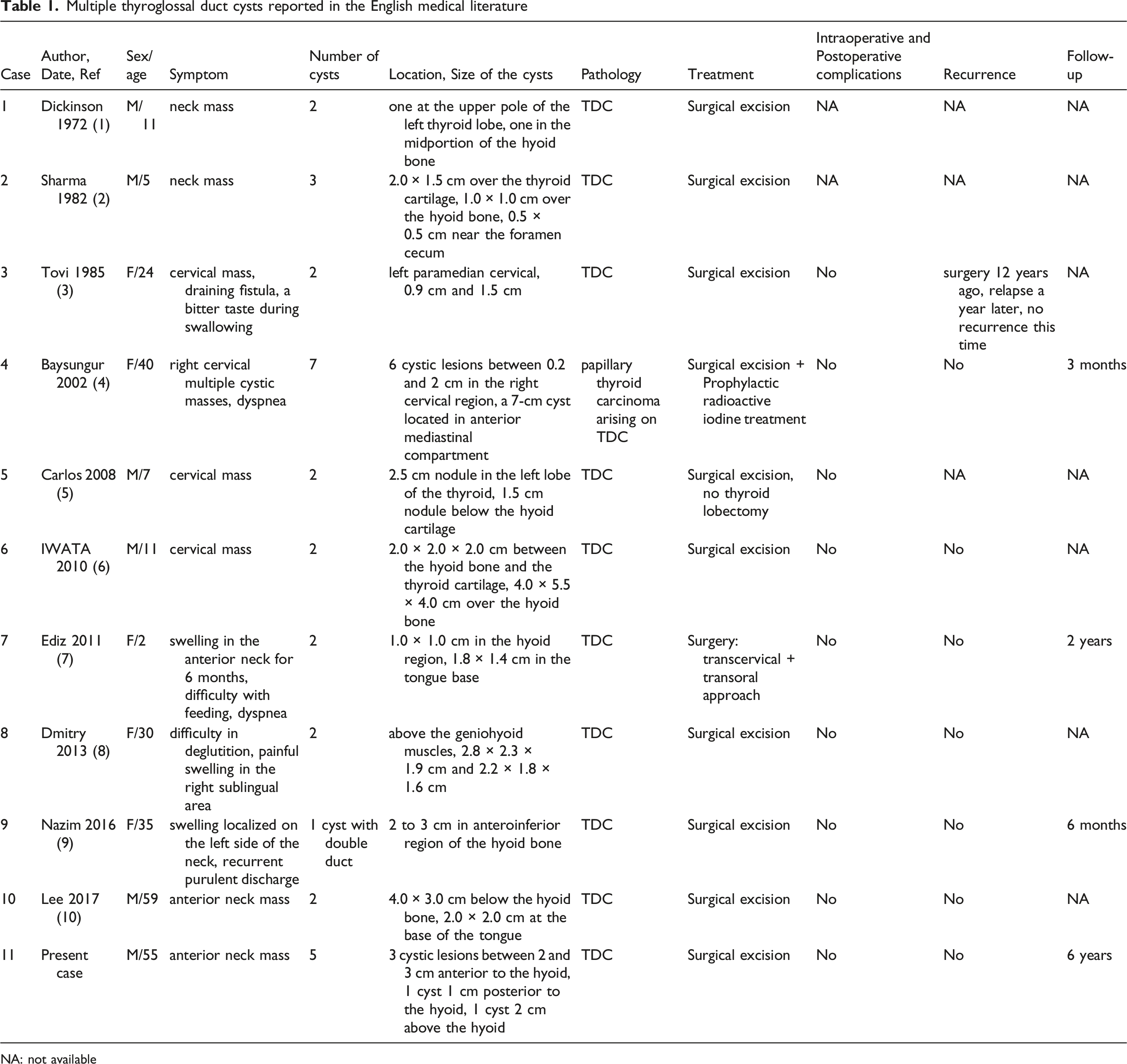
NA: not available
Imaging plays an important role in the diagnosis of TDC. Ultrasonography is the initial selection method to evaluate neck masses clinically suspected to be TDCs, but it can't provide much more detailed information about the masses. Computed tomography (CT) and magnetic resonance imaging (MRI) are useful and reliable imaging methods that can provide information on the location, size, number, and relationship of cysts to surrounding structures. In our case, we performed an MRI scan. Upon cervical palpation, we palpated only a neck mass at the level of thyroid cartilage and hyoid bon. While MRI of the neck revealed that five well-defined cystic lesions were adjacently located around the hyoid bone in the anterior cervical region, which had an important guiding effect on our subsequent surgical treatment.
TDCs are mostly benign masses, development of malignancy are very rare (< 1%). 11 The pathological types of thyroglossal duct cyst carcinoma (TDCCa) were mainly papillary carcinoma (92.1%) and squamous cell carcinoma (4.3%), while other cell types such as follicular, folliculo-papillar, mucoepidermoid, and adeno-squamous types are rarely encountered.11 –15 Baysungur et al reported a case of multiple cystic lesions in cervical and mediastinal region; the postoperative pathologic result was showed as papillary carcinoma arising on the TDC (case 4). The remaining 10 cases of multiple TDCs were benign (case 1-3, 5-11). Clinically, it is difficult to distinguish between benign and malignant cysts, but rapid growth and fixed cyst should alert for malignancy.16 –18 TDDCa should be highly suspected when the following conditions occur: preoperative ultrasonography shows that the cyst is not merely isoechoic hyposignal, but heterogeneous mixed signals, realistic wall nodules accompanied by rich blood flow or microcalcification; calcified wall nodules can be seen on CT, and edge enhancement of the cyst wall nodules can be seen on enhancement.16,19,20
The current accepted treatment for multiple TDCs is surgery. The Sistrunk operation is the most frequently used procedure for treating TDCs. But there are special cases where an extra approach is needed. Ediz et al describe a case of two cysts derived from the same thyroglossal duct, one in the hyoid region and the other in the tongue base, so the patient underwent a transcervical and transoral approach. The Sistrunk operation procedure was performed to remove the cervical cyst, while transoral excision technique was made to remove the tongue base cyst (case 7). Our case containing 5 cysts around the hyoid bone in the anterior cervical region, so we chose a transcervical approach. The five cysts were completely excised in a Sistrunk operation. Our case showed that CT or MRI scans should be read carefully before surgery. During the operation, we should be careful to avoid the cysts to crush each other and rupture. At the same time, we should carefully separate the cysts and remove the middle part of the hyoid bone and the surrounding tissue together, which can prevent cyst residue that leading to recurrence.
Conclusions
Multiple TDCs are extremely rare, and may be misdiagnosed as a single cyst. Clinicians should be aware of the possibility of multiple thyroglossal duct cysts. Adequate preoperative radiological examinations should be performed, and careful interpretation of the CT or MRI scans is important to diagnosis and surgery.
Footnotes
Author Contributions
BYY and YKQ designed and wrote the manuscript. LKD and FZM reviewed the references and made the tables. ZJT made the pictures. ZSH and WCC analysis of the data, revision of the manuscript.
All authors contributed to the article and approved the submitted version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient for the publication of any potentially identifiable images or data included in this article.
Data Availability
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.