
Abstract
Basal cell adenomas (BCA) arising from the nasal cavity or paranasal sinuses are very rare. A 64-year-old male patient was suspected of having a malignant tumor after undergoing preoperative computed tomography scans and magnetic resonance imaging. The intraoperative frozen section showed a malignant tumor; however, the final diagnosis revealed BCA with atypia, tubular pattern.
Introduction
Basal cell adenoma (BCA) is a rare benign neoplasm characterized by the basaloid appearance of the tumor cells, accounting for 1–3% of all salivary gland tumors. 1 BCA most commonly occurs in the major glands, with the parotid gland being the most common location (∼75%), followed by the submandibular gland (∼5%). 2 We report a rare case of BCA in the nasal cavity. We also review the literature and discuss the diagnostic difficulties in cases of BCA in the nasal cavity.
Case Report
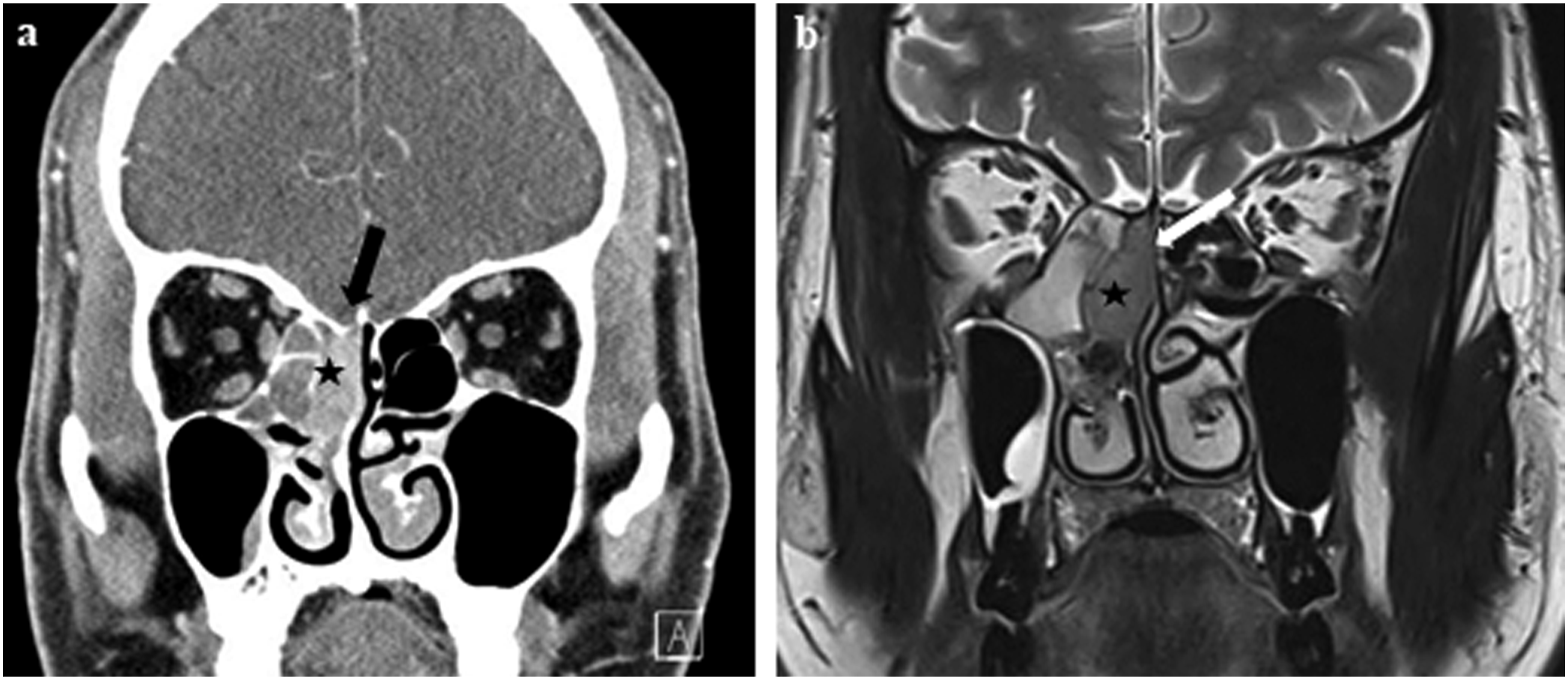
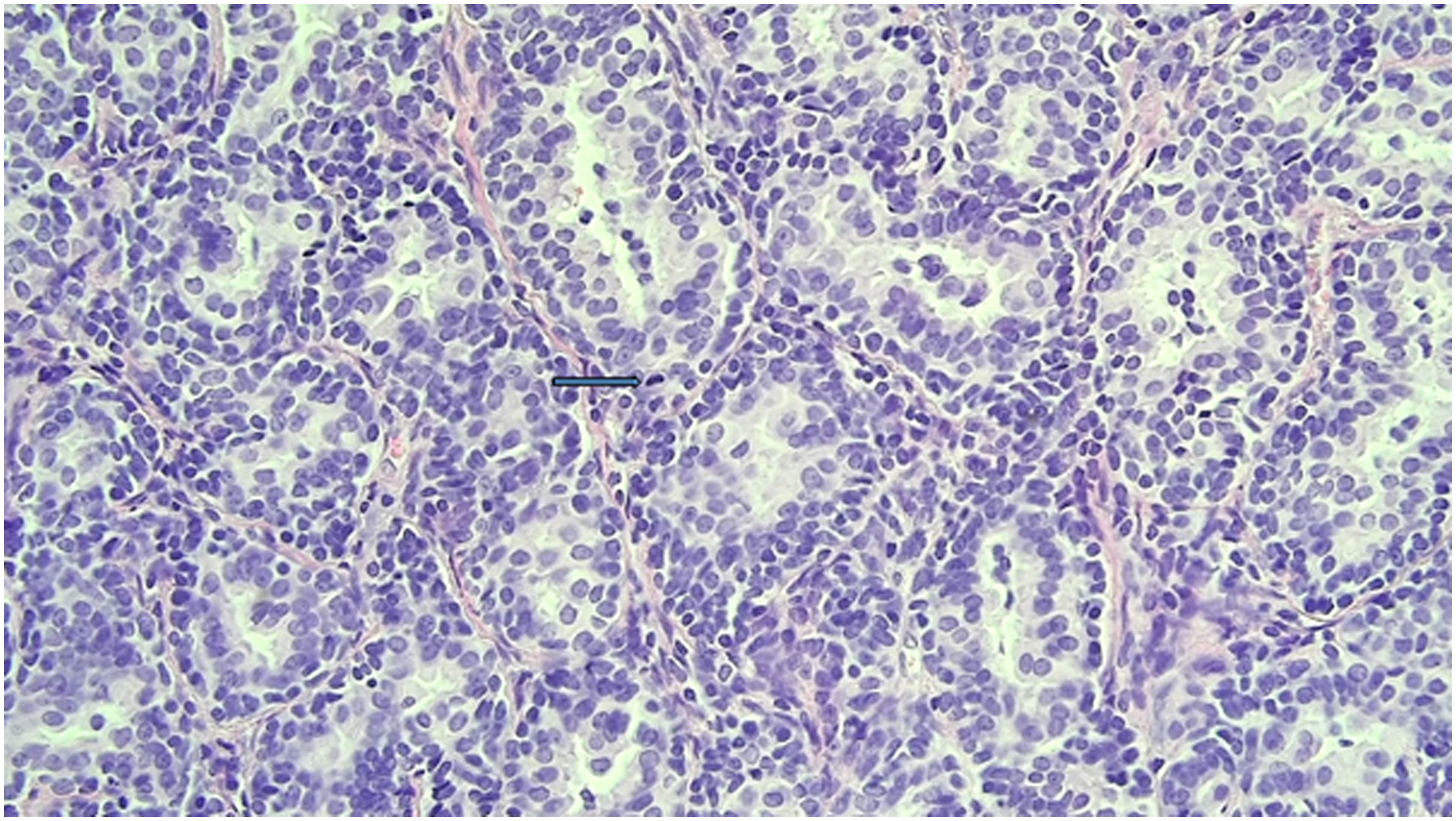
A 64-year-old male patient presented with right nasal bleeding. The patient had a history of hypertension and diabetes mellitus and was on an antihypertensive agent. Endoscopic examination revealed a smooth-surfaced round mass located at the right sphenoethmoidal recess (Figure 1). We performed a biopsy under local anesthesia at the outpatient clinic, and histological analysis revealed a benign serous gland as a proliferative mass. The patient underwent contrast-enhanced computed tomography (CT) scans and magnetic resonance imaging (MRI). The CT scans showed that a 1.2 × 2.9 × 2.4 cm-sized heterogeneous enhancing mass occupied the area from the olfactory recess to the sphenoethmoidal recess (Figure 2A) at the right nasal cavity. T2-weighted MRI image revealed septal erosion due to mass effect but an intact cortex of cribriform plate (Figure 2B). Based on the preoperative CT and MRI findings, the possibility of a malignant tumor such as an olfactory neuroblastoma was suspected. The intraoperative frozen section was analyzed, and a malignancy was suspected. Therefore, endoscopic mass removal, posterior septectomy, and endoscopic sinus surgery were performed. The operation was terminated after confirming that the frozen section margins were negative. However, the final diagnosis showed BCA with atypia based on histopathologic findings of mid nuclear atypia and focal mitosis with no invasive growth (Figure 3). There were no signs of recurrence at the 12-month follow up. Smooth-surfaced, round mass (asterisk) lesion in the right nasal cavity. (arrow: right middle turbinate, arrow head: right nasal septum). CT and MRI of patient. (A) Coronal CT shows a heterogeneously enhanced mass (asterisk) combined with thinning of the cribriform plate (black arrow) of the right nasal cavity. (B) Coronal T2-weighted MRI shows a heterogeneous isointense signal mass (asterisk) and erosion of the septum (white arrow) of the right nasal cavity. Basal cell adenoma with tubular pattern. The tubular structure demonstrates the bilayer of luminal (ductal) and abluminal (basal and myoepithelial) cells. The tumor cells show mild nuclear atypia and focal mitosis (arrow) (Hematoxylin and Eosin, X400).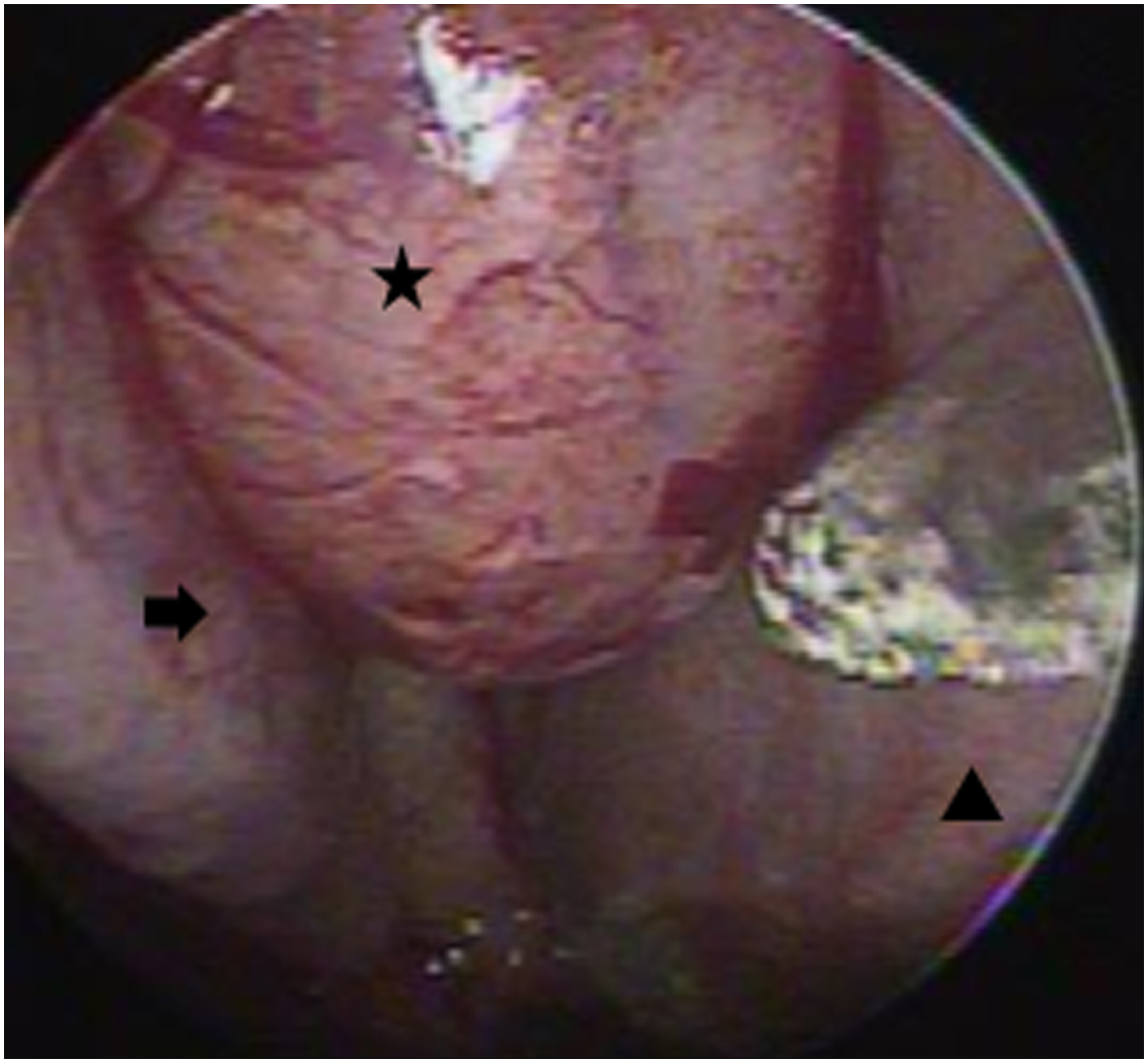
Discussion
BCA is an uncommon benign tumor that is less common in young adults and frequently occurs in major salivary glands, especially the parotid gland. Although rare, BCA occurs in the minor salivary glands of the head and neck and is usually found in the sixth to seventh decade. 3 BCA shows 4 subtypes: tubular, trabecular, solid, and membranous patterns, but mixtures of these patterns are also found. 3 Membranous BCA is more common in malignant transformation and more likely to recur than the other 3 subtypes. 3 Malignant transformation of BCA to basal cell adenocarcinoma or adenoid cystic carcinoma may occur and has been reported in about 4% of cases. Membranous BCA is more common in malignant transformation than in the other types. 4 Surgical excision is the treatment of choice.
To the best of our knowledge, 3 cases of BCA occurred in the nasal septum and sinus as well as 2 cases of BCA in the maxillary sinus.4 –8 However, only one case of BCA in the nasal cavity was reported in the literature. 9 In that case, a 64-year-old male patient had a cribriform and trabecular mixed type of BCA originating from the inferior portion of the left inferior turbinate. 9 As mentioned in the previous cases, intranasal and sinus involvement of BCA is extremely rare, and this is the first case of BCA originating from the right sphenoethmoidal recess. In this case, olfactory neuroblastoma was suspected on preoperative CT scans and MRI, because the location of the tumor originated from the sphenoethmoidal recess and expanded toward the olfactory cleft.
BCA can often be difficult to differentiate from adenoid cystic carcinoma, basal cell adenocarcinoma, and pleomorphic adenoma. 3 Histological morphology analysis in Hematoxylin & Eosin staining is considered most useful for diagnosis. 3 In particular, it can be more difficult to distinguish BCA from early-stage basal cell adenocarcinoma, because BCA and basal cell adenocarcinoma are distinguished by invasive growth patterns of infiltration. 10 In this case, no definite invasive growth was shown in the totally removed mass, and the possibility of basal cell adenocarcinoma was ruled out. However, the tumor cells showed mild atypia and focal mitotic figures. The limitations of the frozen section examination may have resulted in prominent cellular atypia, which could have led to an incorrect diagnosis of malignancy during the intraoperative frozen section. It made the final diagnosis difficult because BCA in the nasal cavity was rare and the tumor was accompanied by cellular atypia and focal mitotic figures.
This patient has a tubular subtype of BCA; therefore, the possibility of recurrence is expected to be low. Nevertheless, this patient needs regular follow-up; first, malignant transformation of BCA is very rare but possible; 11 second, the BCA of this patient shows cellular atypia and mitotic figures.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This case was approved by the institutional review board of Nowon Eulji Medical Center (IRB No. 2023-02-008).
Informed Consent
The institutional review board of Nowon Eulji Medical Center waived the requirement for informed consent (IRB No. 2023-02-008). This study is a case report that does not involve collecting or recording personally identifiable information of the patient.
Data Availability
The authors confirm that the data supporting the findings of this study are available within the article.
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the institutional review board of Nowon Eulji Medical Center (IRB No. 2023-02-008).